Transcription
Trauma-Informed Peer Supportfor People Living with HIVSubstance Abuse and Mental Health Services AdministrationU.S. Department of Health and Human ServicesDeveloped by the National Center for Trauma-InformedCare and Alternatives to Seclusion and Restraint (NCTIC)
DisclaimerThe views, opinions, and content expressed in thispresentation do not necessarily reflect the views,opinions, or policies of the Center for Mental HealthServices (CMHS) or the Center for Substance AbuseTreatment (CSAT), the Substance Abuse and MentalHealth Services Administration (SAMHSA), or the Bureauof Justice Assistance (BJA), Office of Justice Programs(OJP) Department of Justice (DJS), or the U.S. Departmentof Health and Human Services (HHS).2
Learning Objectives/Goals Define “peer support” Define “trauma” and its impact Define “culture” and its influence Discuss principles of trauma-informed practiceand their application in peer support Explore strategies for applying this knowledge inpeer-support relationships3
Peer Support Basics4
Peer Support Principles Voluntary Non-judgmental Respectful Reciprocal Empathetic5
Peer Support Definition Peer support is a flexible approach to buildinghealing relationships among equals, based on acore set of values and principles. Peers serve as role models for living and thrivingwith HIV, provide hope to clients living with HIV,and share strategies for overcoming thechallenges of living with HIV (Boston University,2009).6
Denver Principles In 1983, a group of people living with HIV cametogether to create a manifesto, called the DenverPrinciples. It was a call to action for the community, health careproviders, and policymakers. "We condemn attempts to label us as ’victims,’ whichimplies defeat, and we are only occasionally ’patients,’which implies passivity, helplessness, and dependenceupon the care of others. We are ‘people with AIDS.’”- Denver Principles opening statement7
What Peer Support is NOT A “program model” About “helping” in a top-down way Being a “counselor” Pressuring people to comply with adherence or treatment Monitoring people’s behavior8
Avoid Helping that Hurts “Helping” in a top-down way may:– Reinforce feelings of helplessness.– Imply that one person is more “together” or“recovered” than the other.– Send the message that people living with HIV areincapable of directing their own lives.9
Peer Support Can Focus On . . . 10Educational pursuitsSocial activitiesAdvocacyHarm reduction strategiesCommunity connection
Co-optationCo-optation occurs when a group tries toassimilate a weaker or smaller group, with theintention of neutralizing a perceived threat fromthe weaker group.11
Co-optation (con.) Co-optation can happen if people loseconnection with peer support values andbegin to take on views and beliefs thatdemean people who use services. If the organization doesn’t support peer rolesthrough policy and practice, peers can feelalienated or threatened.12
To Avoid Co-optation Develop strong relationships with other peersupport staff. Educate yourself about the history of themovement of people living with HIV. Reach out to local, state, and nationalorganizations by and for people living with HIV. Talk about peer support values to non-peer staff.13
Strategies to Thrive Educate people who use services about traumaand peer support. Educate staff about trauma and peer support. Have collaborative conversations by:– Exploring each others’ perspectives and experiences.– Using your story strategically.– Offering new solutions and ideas.14
Self-awareness“In the thick of this work we oftenforget about our own needs . . . ”- Shery Mead, founder of Intentional Peer Support15Self-care is essential
Self-awareness (con.) Be aware of:– The impact of trauma on your own life.– Your own emotional “hot-spots”—words, sights,smells, sounds, behaviors, characteristics, andemotions.– How your own experiences may influence yourfeelings and responses to people you support.16
Trauma & Its Impact17
Defining Trauma The 3 Es:– “Individual trauma results from an event, series ofevents, or set of circumstances that is experienced byan individual as physically or emotionally harmful orlife threatening and that has lasting adverse effects onthe individual’s functioning and mental, physical,social, emotional, or spiritual well-being.”(SAMHSA, Concept and Guidance for a Trauma-InformedApproach, 2014)18
Some Potential Sources of Trauma Childhood sexual, physical,emotional abuse, neglect,abandonment Rape, sexual assault,trafficking Domestic violence,experiencing/witnessing otherviolent crime Catastrophic injury or illness,death, loss, grief Institutional abuse and neglect War/terrorism19 Community and school violence,bullying Cultural dislocation or suddenloss, historical/ generationaltargeted violence Chronic stressors such as racism,homophobia, transphobia,misogyny, poverty, discriminationrelated to HIV diagnosis Natural disasters Invasive medical procedures Any misuse of power by oneperson over another
ActivityTracing Trauma in Your Life20
Talking about Trauma If, how, and when a person chooses to talkabout experiences is personal. Some may not label what happened to themas “trauma.” Be aware of the words you use and beprepared that others’ words may be different.21
Trauma Affects the Developing Brain Brain development isaffected by earlyexperiences, includingtraumatic experiences. We develop ways to cope,survive, and defendourselves against deep andenduring wounds.22
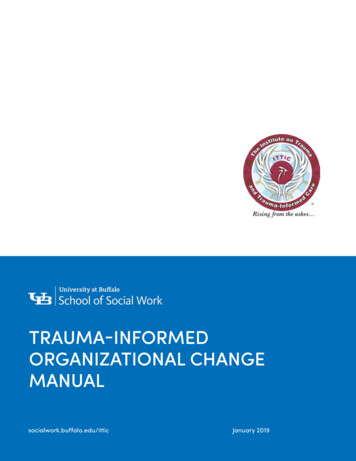
Fight, Flight, or Freeze The brain signals the body to respond to aperceived threat and the body prepares. Ordinarily, when the threat is gone, the bodyreturns to “baseline.” If an ongoing threat is perceived, the bodydoesn’t return to baseline and remains preparedfor threat, resulting in a “trauma response.” The switch is stuck in the “on” position.23
24Source: Levine, 1997
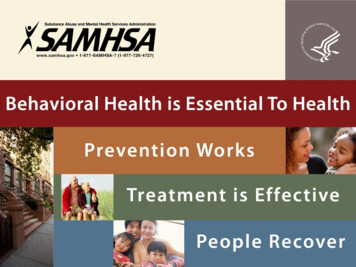
Trauma Linked to Health Challenges Over the Lifespan25Adverse ChildhoodExperiencesBiological Impacts and Long-term Health andHealth RisksSocial ProblemsThe more types ofadverse childhoodexperiences The greater thebiological impacts andhealth risks, and The more serious thelifelong consequencesto health and well-beingSource: Felitti, V.J., Anda, R. F., et. al., 1998
Factors That May Intensify Trauma The earlier in life trauma occurs, the more severe thelikely long-term effects. Deliberate violence is particularly damaging, especiallywhen inflicted by trusted caregivers. Violence, compounded by betrayal, silence, blame, orshame, impacts the ability to form intimaterelationships. Sanctuary trauma occurs when a person or institutionthat is supposed to be safe, is not. The betrayal is deepand enduring.26
Impact of Trauma Survivors may be responding to the present throughthe lenses of their past. Things survivors do to cope may be misinterpreted bystaff deliberately being uncooperative with a medicalor medicine protocol; a term for this is “nonadherence.” This can lead to punitive reactions by staff to peoplewho are struggling with trauma responses. Often, people are unaware that their challenges arerelated to trauma.27
Trauma Disconnects Trauma can:– Leave people feeling powerless.– Have lasting effects on the ability to trust othersand form intimate relationships.– Impact relationships with self, others,communities, and environment.– Create distance between people.28
Trauma and HIV: What’s the connection? People living with HIV experience disproportionately highrates of trauma throughout the life span. Traumatic experiences, including histories of childhoodsexual and physical abuse, are far more common amongpeople living with HIV than in the general U.S.population. People living with HIV also are disproportionatelyaffected by adult/ongoing trauma, including intimatepartner violence (IPV). Lifetime trauma impacts both HIV-risk behavior and theability of people living with HIV to engage in HIV care.29
Why Must We Focus on Trauma? The vast majority of women living with HIV are dying not fromHIV-related causes but from murder, suicide, addiction, andother causes associated with lifelong trauma (French et al.,2009). A 2018 California-wide study found that women living with HIVwere 25 times more likely to die from an overdose or a mentalhealth condition related to substance use than the generalpopulation of women in the state (Hessol et al., 2018). The same study found that men living with HIV were nearlythree times as likely to die by suicide than the generalpopulation of men in California. HIV (like many other health conditions) is a symptom of a far30 larger problem: widespread, unaddressed trauma.
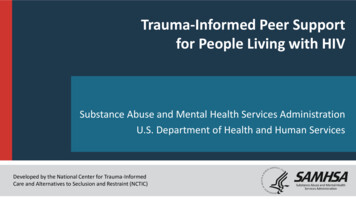
Impacts of Trauma on Health: Structural bia, prejudice,discriminationIntimate PartnerViolenceDisclosure, isolation,fear, depression,PTSDHealth &WellbeingLiving with HIV istraumatic.Source: Sonia Rastogi, 2012InstitutionalViolenceSubstance use andHIV criminalizationlaws, educational,vocational, housingand health carediscrimination
How Trauma Impacts Engagement in HIV CareStudies indicate that peopleliving with HIV with past and/orrecent trauma: Take longer to be linked tocare after being diagnosed. Are less likely to stayengaged in care. Are less likely to adhere toantiretroviral therapy (ART).32
Trauma and Antiretroviral Medications Taking antiretroviral therapy (ART) differently thanprescribed is correlated with frequent childhood trauma,childhood sexual abuse, depression, and PTSD (Whettenet al., 2013; Meade et al., 2009). HIV-positive women with recent trauma are four timesmore likely to experience ART failure (Machtinger et al.,2012b). Sexual trauma is associated with greater likelihood ofART being unable to control HIV infection; a term for thisis “treatment failure.”33
Trauma & Mortality from HIVTraumatic experiencesover the life span areassociated with fasterdevelopment of anopportunistic infection orAIDS-related death(Leserman, 2007).34
Resilience SAMHSA defines resilience as the ability of anindividual, family, or community to cope withadversity and trauma and adapt to challengesor change. Resilience is promoted in part by supportiverelationships and social connectedness, aswell as addressing sources of adversity.35
The Brain Can Heal“Our brains are‘neuroplastic,’ meaningthat they can changeand adapt based on ourenvironments andexperiences.”Source: Dr. Celeste Campbell. What is eleste-campbell/qa/what-neuroplasticity36
Healing is Possible!“Healing from trauma, likehealing from a physicalinjury, is a natural humanprocess.”- Richard Mollica, 200837
Healing from Trauma Healing from trauma requires:– Regaining a sense of control over one’s life andenvironment;– Maintaining a sense of safety;– Developing the ability to trust self and others; and– Reconnecting with others. Healing happens in relationships.38
Trauma-Informed Practices39
SAMHSA’s Key Principles of Trauma-Informed Approaches 40SafetyTrustworthiness and TransparencyPeer SupportCollaboration and MutualityEmpowerment, Voice, and ChoiceCultural, Historical, and Gender Issues
Non-Trauma-Informed Practices Non-trauma-informed practices:41– Recreate the fear and helplessness of the originaltrauma.– Cause distrust, sadness, anger, frustration, andconfusion.– Can result in people disengaging from care.– Lead to survivor reactions being viewed as“symptoms,” which can increase the rationale for“management” and potential for coercion.
Trauma-Informed Practices Based on the universal expectation thattrauma has occurred and/or may be ongoing. Focused on understanding “What happenedto you?” not “What’s wrong with you?” Seek to understand the meaning people makeof their experiences.42
Trauma-informed Practices (2) Ensure all staff and people who use servicesare educated about trauma. Incorporate knowledge about trauma in allaspects of service delivery. Minimize revictimization—“do no more harm.” Take particular care to create a welcomingenvironment.43
Trauma-informed Practices (3) Trauma-informed practices:– Strive to be culturally responsive.– Focus on resilience, self-healing, mutual support, andempowerment.– Ensure that trauma-informed principles (safety;trustworthiness and transparency; peer support;collaboration and mutuality; empowerment, voice andchoice; and cultural, historical, and gender issues) arespecifically addressed. Trauma treatment is different: specific modalities ortherapies to treat manifestations of trauma (works bestin a trauma-informed setting).44
“Radars”Trauma survivors oftenhave sensitive “radars”for detecting dishonestyand good reasons to besensitive to any misuseof power and authority.45
Those working with survivors “have a tendencyto deal with their frustration by retaliating inways that often uncannily repeat the earliertrauma.”- Bessel van der Kolk, 2003, trauma expert46
What does help look like? NOT Trauma Informed:– Needs are defined by staff– Safety is defined as riskmanagement protocol– The helper decides whathelp looks like– Relationships based onproblem-solving andaccessing resources– Help is top-down andauthoritarian47 Trauma Informed– Needs are identified bysurvivor– Safety defined by eachsurvivor– Survivors choose the helpthey want– Relationships are based onautonomy and connection– Help is collaborative andresponsive
Cultural Considerations48
“We don’t see things as they are,we see things as we are.”- Anais Nin, writer49
What is culture?Culture is defined as the shared values, traditions,arts, history, folklore, and institutions of a group ofpeople that are unified by race, ethnicity,nationality, language, religious beliefs, spirituality,socioeconomic status, social class, sexualorientation, politics, gender, age, disability, or anyother cohesive group variable.- Singh, Williams, & Spears, 199750
Cultural ConsiderationsSelf Identity Race Ethnicity Age Gender Sexual orientation Language Family Beliefs about capabilities History Country of birth51Belonging and Participating Spirituality Education Illness/wellness Literacy Incarceration Military Employment/Income Where you live Immigration status Parenting
My Cultural Pie52
Cultural Considerations & TraumaSelf IdentityBelonging and Participating Race Spirituality Ethnicity Education Age Illness/wellness Gender Literacy Sexual orientationTRAUMA Incarceration Language Military Family Employment/Income Beliefs about capabilities Where you live History Immigration status Country of birth Parenting53
Culture Counts Culture influences:– The experience of trauma.– The meaning people make of what has happened.– How and whether people express their pain. One’s cultural experience affects beliefs,behaviors, and attitudes toward self and others. Assumptions made about others may becomebarriers to effective support.54
No Assumptions Every conversation can be a cross-culturalconversation. We may not know the source of someone’s joy,pride, or pain. We do not know how oppression/trauma haveimpacted a person’s life. We do not know what self-protecting copingstrategies people need to use.55
BE CURIOUS,BE EMPATHETIC,BE FLEXIBLE56
Trauma-Informed Peer Support57
Effective Peer Support 58Validates personal realityFosters trust and connectionLeads to empowermentBreaks patterns of helplessness and hopelessnessEncourages use of voice and choiceRespects personal boundariesCreates a sense of safety in relationship
Trauma-Informed Peer Support Trauma-informed peer support:– Sees behaviors as strategies for coping with pastand current trauma.– Helps survivors make sense of how they arecoping and surviving.– Creates a safe space to consider new copingstrategies.59
Conflicting Definitions of “Safety” For people who use services, “safety”generally means maximizing control over theirown lives. For providers, “safety” generally meansmaximizing control over the serviceenvironment and minimizing risk.60
Power Dynamics If we’re not alert to the use of power, peersupport relationships may unintentionallyrecreate the power dynamics of the originaltrauma. Being mindful of peer-support principles canhelp address this issue.61
MutualityThere are no static roles of “helper” and“helpee” . . . reciprocity is the key to buildingnatural connections.- Shery Mead and Cheryl MacNeil, 200562
ActivityWhat gets in the way of sharing power?63
What gets in the way of sharing power? Lack of role clarityStruggling to manage strong emotionsPreconceived attitudesDesire to manage other’s behavior (particularly ifviewed as harmful, self-inflicted violence) Fear, discomfort, misunderstanding How “safety” is defined and used64
Maintaining Your Integrity Be transparent in your relationships. Let people you support know up front thelimits of your relationship within the programand agency. Don’t assume the people you work with knowwhat peer support is: teach them, and theycan offer each other peer support.65
Understanding Self-Injury and Other CopingStrategies66
Understanding Self-Injury The intentional injuring of one’s body as ameans of coping with severe emotionaland/or psychic stressors The primary purpose is to provide a way ofcoping with what feels intolerable.- Ruta Mazelis, 200867
Self-Injury Evolves as a way to cope with trauma Is a response to distress, past and/or present Has meaning for each survivor, such as:– Regaining control– Asserting autonomy– Relief of emotional pain68
ActivityOther Coping Strategies69
Relationships and Coping How does trauma impact our choices inrelationships? How might trauma impact a person’s abilityto protect him or herself in relationships? Can we understand what is called “riskysexual behavior” as the best coping strategya person might have? How?70
Substance Use as Coping“The attempt to escape from pain, is whatcreates more pain. We should be asking not‘why the addiction,’ but ‘why the pain?’”― Gabor Maté, What is Addiction video71
A Shift in ThinkingFromSeeing the person asengaging in meaningless,frustrating, and dangerousbehaviorToUnderstanding self-injuryas an expression ofprofound pain that hasmeaning for the personIT IS NOT YOUR JOB TO FIX ANYONE72
Personal Narratives73
Personal Narratives Personal narratives can:– Help organize one’s experience and help makesense of what has taken place.– Lay the groundwork for survivors to develop hopeabout the future.– Be told through talking, music, dance ormovement, drumming, art, and writing.74
Trauma Narratives Trauma narratives may include:– All or part of the traumatic events.– The impact on one’s life.– The meaning one has made out of whathappened.– Beliefs about who one is and who one is capableof becoming.75
What Creates Distance? Narratives that are difficult to listen to or hard tounderstand Telling the same narrative over and over again Competing trauma narratives Narratives told through the language of behavior(e.g., running out of a group, harm to self) Talking about the “taboo”76
Is telling necessary for healing? People must be supported if they choose NOT toshare their experience. Not everyone can or wants to share theirexperience. There may be cultural constraints on selfdisclosure. It may be too painful. It may be currently unsafe.77
Support Narrative Sharing Ask whether the person wants to sharehis/her/their experiences. Offer opportunities and materials to supportdifferent ways of expressing the narrative. Listen for meaning.78
Reclaiming Power through Social Action79
The Personal is Political“All violence focuses on the unfair distribution ofpower and the abuse of this power by thepowerful against the helpless. The solutions tothese problems are not individual solutions;they require political solutions.”- Tedeschi, Park, & Calhoun (Eds.)(1998)80
Reclaiming Power through Social Action Trauma often leaves survivors feeling bothpowerless and full of rage. Taking social action can be a:– Positive act of healing.– Productive way to channel anger.– Way for survivors to reclaim a sense of purposeand personal power.81
Reclaiming Power through Social Action (con.) Social action can include:– Organizing around a common goal.– Giving witness testimony.– Working to change harmful policies & practices.– Challenging injustice.– Creating supportive alternatives.82
Self-awareness is EssentialSelf-care is a priority and a necessity –not a luxury – in our work.83
WHAT WILL YOUR COMMITMENT BE?84
References (1) American Psychological Association. (n.d.). The Road to Resilience. Retrieved from http://www.apa.org/helpcenter/road-resilience.aspx Arriola, K. R., Louden, T., Doldren, M. A., & Fortenberry, R. M. (2005). A meta-analysis of the relationship of child sexual abuse to HIVrisk behavior among women. Child Abuse & Neglect, 29(6), 725-746. Bensley, L. S., Van Eenwyk, J., & Simmons, K. W. (2000). Self-reported childhood sexual and physical abuse and adult HIV risk behaviorsand heavy drinking. American Journal of Preventive Medicine, 18(2), 151-158. Boston University, Center for Advancing Health Policy and Practice. (2009). Building Blocks to Peer Program Success: A Toolkit forDeveloping HIV Peer Programs. Retrieved from AIDS United. (n.d.) The Intersection of Women, Violence, Trauma, and HIV. Retrievedfrom https://www.aidsunited.org/data/files/Site 18/IntersectionofWomenViolenceTrauma3.pdf Briere, J., & Elliott, D. M. (2003). Prevalence and psychological sequelae of self-reported childhood physical and sexual abuse in ageneral population sample of men and women. Child Abuse & Neglect, 27(1), 1205-1222. Campbell, C. (2009). What is neuroplasticity? Retrieved from qa/whatneuroplasticity Centers for Disease Control and Prevention (CDC). (2016). HIV Surveillance Report. Retrieved .pdf CDC. (2016a). Issue Brief: HIV and Transgender Communities. Retrieved from ender-brief.pdf CDC. (2017). Diagnoses of HIV infection in the United States and dependent areas, 2016. HIV Surveillance Report, 28. Retrieved .pdf85
References (2) CDC. (2017a). HIV among transgender people. Retrieved from ndex.html Child Welfare Information Gateway (2013). Child Maltreatment 2011: Summary of Key Findings. Children Bureau, DHHS Administrationfor Children, Youth and Families, February, 2013. ats.cfm Child Witness to Violence Project (n.d.). Facts and myths. Retrieved from .html Choi, K-H., Paul, J., Ayala, G., Boylan, R. & Gregorich, S. E. (2013). Experiences of discrimination and their impact on the mental healthamong African American, Asian and Pacific Islander, and Latino men who have sex with men. American Journal of Public Health, 103(5),866-874. Edelman, E.A., Corado, R., Lumby, E.C., Gills, R.H., Elwell, J., Terry, J.A., & Emperador Dyer, J. (2015). Access Denied: Washington, DCTrans Needs Assessment Report. DC Trans Coalition. Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., . Marks, J. S. (1998). Relationship of childhoodabuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study.American Journal of Preventive Medicine, 14(4), 245-258. Fergusson, D. M., Boden, J. M., & Horwood, L. J. (2008). Exposure to childhood sexual and physical abuse and adjustment in earlyadulthood. Child Abuse & Neglect, 32(6), 607-619. Finkelhor, D., Turner, H. A., Shattuck, A., & Hamby, S. L. (2013). Violence, crime, and abuse exposure in a national sample of childrenand youth: an update. JAMA pediatrics, 167(7), 614-621. French, A. L., Gawel, S. H., Hershow, R., Benning, L., Hessol, N. A., Levine, A. M. Anastos, K., Augenbruan, M., & Cohen, M. H. (2009).Trends in mortality and causes of death among women with HIV in the United States: a 10-year study. J Acquir Immune Defic Syndr, 1,51(4):399-406.86
References (3) Galtung J. (1969). Violence, peace, and peace research. J Peace Res, 6(3),167–91. Geter, A, et al. (2016). Experiences of antihomosexual attitudes and young black men who have sex with men in the South: a need for communitybased interventions. LGBT Health, 3(3), 214-218.Hessol, N. A., Schwarcz, S. K., Hsu, L. C., Shumway, M., & Machtinger, E. L. (2018). Gender differences in causes of death among persons withHIV/AIDS in San Francisco, California, 1996–2013. International journal of STD & AIDS, 29(2), 135-146. James, S. E., Herman, J. L., Rankin, S., Keisling, M., Mottet, L., & Anafi, M. (2016). The Report of the 2015 U.S. Transgender Survey. Washington, DC:National Center for Transgender Equality. Kaiser Family Foundation. (2014). Analysis: Opportunities Under the ACA for Addressing Intimate Partner Violence Among Women With HIV. Retrievedfrom te-partner-violence-among-women-withhiv/Lane, S. D., Rubinstein, R. A., Keefe, R. H., Webster, N., Cibula, D. A., Rosenthal, A., & Dowdell, J. (2004). Structural violence and racial disparity in HIVtransmission. Journal of Health Care for the Poor and Underserved, 15(3), 319-335. Lark, H,. Babu, A. S., Wiewel, E. W., Opoku, J., & Crepaz, N. (2016). Diagnosed HIV Infection in Transgender Adults and Adolescents: Results from theNational HIV Surveillance System, 2009-2014. AIDS Behav., 21(9), 2774-2783. doi: 10.1007/s10461-016-1656-7. Leserman, J. (2008). Role of depression, stress, and trauma in HIV disease progression. Psychosomatic Medicine, 70(5), 539–45. Epub 2008/06/04.doi: 10.1097/PSY.0b013e3181777a5f. PubMed PMID: 18519880. Leserman, J., Whetten, K., Lowe, K., Stangl, D., Swartz, M. S., & Thielman, N. M. (2005). How trauma, recent stressful events, and PTSD affectfunctional health status and health utilization in HIV-infected patients in the south. Psychosomatic Medicine, 67(3), 500–7. Epub 2005/05/25. doi:10.1097/01. James, S. E., Herman, J. L., Rankin, S., Keisling, M., Mottet, L., & Anafi, M. (2016). The Report of the 2015 U.S. Transgender Survey. Washington, DC:National Center for Transgender Equality.87
References (4) Kaiser Family Foundation. (2014). Analysis: Opportunities Under the ACA for Addressing Intimate Partner Violence Among Women With HIV. Retrievedfrom te-partner-violence-among-women-withhiv/ Levine, P. (1997). Waking the tiger. North Atlantic Books. Machtinger, E., Haberer, J. E., & Weiss, D. S. (2012). Recent trauma is associated with antiretroviral failure and HIV transmission risk behavior amongHIV-positive women and female-identified transgenders. AIDS Behav., 16(8):2160-70. Maniglio, R. (2009). The impact of child sexual abuse on health: A systematic review of reviews. Clinical Psychology Review, 29(7), 647-657. Mazelis, R. (2008). Self-Injury: Understanding and Responding to People Who Live with Self-Inflicted Violence. Retrieved .pdf Mead, S., & MacNeil, C. (2005). Peer support: A systemic approach. Family Therapy Magazine Meade, C. S., Hansen, N. B., Kochman, A., & Sikkema, K. J. (2009). Utilization of medical treatments and adherence to antiretroviral therapy amongHIV-positive adults with histories of childhood sexual abuse. AIDS Patient Care STDS, 23(4), 259–266. Miller, N. (2008). Trauma-informed Approaches in Custody Settings. NHDOC Academy Training Curriculum. Concord, NH. Mueser, K.T., Salyers, M.P., Rosenberg, S.D., Goodman, L.A., Essock, S.M., et al. (2004). Interpersonal Trauma and Posttraumatic Stress Disorder inPatients With Severe Mental Illness: Demographic, Clinical, and Health Correlates. Schizophrenia Bulletin, 30 (1), 45-57. NAM. (2017) Who are trans women acquiring HIV from? Retrieved from ng-HIVfrom/page/3167205/88
References (5) National Child Traumatic Stress Network (2011). Facts for policymakers: Trauma exposure, psychosocial functioning and treatmentneeds of youth in residential care. Retrieved ts/pdfs/policybrief3 traumaexposure.pdf Pence, B. W., Reif, S., Whetten, K., et al. (2007). Minorities, the poor, and survivors of abuse: HIV-infected patients in the US deepSouth. South Med J, 100(11), 1114–1122. Rastogi, S. (December 2012). Integrating trauma-informed and sexual and reproductive health care in the domestic HIV response. U.S.Positive Women’s Network: Revitalizing the U.S. Domestic HIV Response. Retrieved from tic-hiv-response Read, J., Fink, P.J., Rudegeair, T., Felitti, V., and Whitfield, C.L. (2008) Child maltreatment and psychosis: A return to a genuinelyintegrated bio-psycho-social model. Clinical Schizophrenia and Related Psychoses, 235-254. Schafer, K. R., Gupta., S., & Dillingham, R. (2013). HIV-infected men who have sex with men and histories of childhood sexual abuse:Implications for health and prevention. J Assoc Nurses AIDS Care, 24(4), 288-298. Senn, T. E., Carey, M. P., & Vanable, P. A. (2008). Childhood and adolescent sexual abuse and subsequent sexual risk behavi
prescribed is correlated with frequent childhood trauma, childhood sexual abuse, depression, and PTSD (Whetten et al., 2013; Meade et al., 2009). HIV-positive women with recent trauma are four times more likely to experience ART failure (Machtinger et al., 2012b). Sexual trauma is associated with greater likelihood of