Transcription
It’s Not You, It’s Just CultureKyle Finnerty, PharmD, MBAPGY-2 Health System Pharmacy Administration and Leadership ResidentUniversity of Utah HealthKyle.Finnerty@hsc.utah.eduKyle Finnerty, PharmD, MBANovember 10, 20201PollEverywhere Audience Response ACPE requires active learning and most prefer real-time participation rather than a graded post-test We are utilizing PollEverywhere software for this process. Disclosure Relevant Financial Conflicts of Interest CE Presenter, Kyle Finnerty, PharmD, MBA NoneYou may join to participate by 3 different ways:Web Browser: Go to PollEv.com/ushp CE mentor, Lauren Lowery, PharmDPollEverywhere app: Download app and join ushp presentation NoneText Messaging: Text ushp to 22333 We recommend the PollEverywhere app or web browser as they are easier to respond For each question, you can click on the correct answer in Web Browser or App or text correctanswer to 223332 Off-Label Uses of Medications None34Pharmacist Learning ObjectivesTechnician Learning Objectives Explain the differences between punitive culture, no-blameculture, and just culture Discuss the benefits of just culture in health care Design process improvement initiatives using just cultureprinciples to created highly reliable systems Analyze the role of shared accountability in processimprovement and system design Identify ways to monitor and assess system design changes Apply system design strategies to reduce risk and preventhuman error561
Culture TimelinePunitive Culture Mindset: expect perfection and settle for nothing less Equation for perfect performance Perfection care education professionalism vigilance Hold people accountable for their errors Violating protocol is not tolerated Mistakes Blame and Punishment Severe mistakes deserve severe punishmentRoyal Pharmaceutical Society. (2020). The Right Culture. Retrieved September 11, 2020,from guides/the-right-cultureSmetzer, J., R.N., B.S.N., FISMP. (2020, September 11). Moving from Punitive Retributionto Just Restoration. Lecture presented at Medication Safety Certificate Program.7Issues with Punitive CultureNo-Blame CultureFear No news good news All corrective actions focusedon people instead of system Response to negative effects of punitive cultureExcessiveerror Creates culture of fear Acknowledges human errorWorkaround Unsafe acts often were a result of honest mistakes, mental lapses Honest errors did not justify punitive actionPunishment Root of errors embedded in system processes Errors are unreported Lose opportunities to learn Patient safety compromised8 Error would continue until they were reportedPoorproblemsolving Encourages employees to report errorImproperutilizationSmetzer, J., R.N., B.S.N., FISMP. (2020, September 11). Moving fromPunitive Retribution to Just Restoration. Lecture presented atMedication Safety Certificate Program.Smetzer, J., R.N., B.S.N., FISMP. (2020, September 11). Moving fromPunitive Retribution to Just Restoration. Lecture presented atMedication Safety Certificate Program.9Characteristics of No-Blame CultureProblems with No-Blame Culture Appreciation for others Fails to confront individuals who repeatedly maydemonstrate unsafe behaviors Belief in honesty10 Little to no personal accountability for error Focus on behavioral expectations Allows for repeated error to occur Realistic understanding of humans Do not force employees to improve but encourage themevaluate and change their processes Regular use of debriefs Shared understanding of complexityInvestors in People. (2020, February 18). What does a no blame culture actuallylook like? Retrieved September 11, 2020, -blame-culture-actually-look-like/11Royal Pharmaceutical Society. (2020). The Right Culture. Retrieved September 11, 2020, nce-guides/the-right-cultureSmetzer, J., R.N., B.S.N., FISMP. (2020, September 11). Moving from Punitive Retribution to JustRestoration. Lecture presented at Medication Safety Certificate Program.122
To Err is Human: Building a Safer HealthSystemJust Culture Published in 2000 by IOM Highlights medical errors inAmerican health systems Called for national efforts toimprove the safety ofhealthcare “the problem is not badpeople in health care it’sgood people working in badsystems that need to bemade safer.” Balance between punitive and no-blame cultures Does not focus on people or systems Focus on people in systems Employees accountable for actions under their control Employees evaluate process for risk that may compromisesafety Managers evaluate systems to identify areas forimprovementKohn, L., Corrigan, J., & Donaldson, M. (2000). To Err is Human:Building a Safer Health System. Retrieved September 11, 2020, ://foter.com/explore/search/?q to err is humanRoyal Pharmaceutical Society. (2020). The Right Culture. Retrieved September 11, 2020,from guides/the-right-cultureSmetzer, J., R.N., B.S.N., FISMP. (2020, September 11). Moving from Punitive Retributionto Just Restoration. Lecture presented at Medication Safety Certificate Program.1314PharmacistImportance of Just CultureWhich of the following is true regarding themanagement of error in no-blame culture? Creates psychological safetyA. Error results in punishment Empowers employees to speak up Encourages proactive monitoring and reporting of safety events No fear of retribution for reporting eventsB. Severity of outcomes drives the severity of punishmentC. A systems approach is used to evaluate error but theemployee bears little or no responsibility for error Improves patient safetyD. Employees are responsible for actions under their control Reduces risk Improves patient outcomes Improves QualityBoysen, P., II. (2013). Just Culture: A Foundationfor Balanced Accountability and Patient Safety.The Ochsner Journal, 13(3), 400-406.1516PharmacistJust culture believes that humans should beheld accountable for decisions under theircontrol.Elements of Just CultureA. True Align values and expectationsB. False Make better behavioral choices Learn to think systematically Design better systems17Smetzer, J., R.N., B.S.N., FISMP. (2020, September 11).Moving from Punitive Retribution to Just Restoration.Lecture presented at Medication Safety Certificate Program.183
Elements of Just CultureEvaluate Current CultureGenerative Culture Align values and expectationsCyclic flow of information and feedback Make better behavioral choicesProactiveThink ahead, create solutions before problems are seen Learn to think systematicallySystematic Culture Design better systemsSystems in place to manage hazardsReactive CultureReact to eventsPathologic CultureUnaware of safety culture Geared toward safety andimprovement Employees engage withdialogue, learning andsupport Processes for senior leadersto interact with front line staff Leadership shows up onlywhen something occurs Does not want to know aboutsafety related issuesInstitute for Healthcare Improvement. (2019). PatientSafety Essentials Toolkit. Institute for HealthcareImprovement.19Aligning Values and Culture Top down approach Determine what is important toyour organization Incorporate tools and channels tohonor your values and stayaligned20Elements of Just Culture Align values and expectationsSeniorLeadership Make better behavioral choices Learn to think systematicallyMid-levelManagement Design better systems Measure and monitor resultsFront Line StaffEdmonds, C. (2017, August 11). 4 Steps to Ensure ValuesAlignment and Reduce Workplace Stress. Retrieved September 11,2020, from aluesAlignment-and-Reduce-Workplace-Stress2122The Three BehaviorsWhat is the solution to this equation? Human Error 4 6 3 8 4A. 20 At-Risk BehaviorB. 5.5 Reckless BehaviorC. 3.5D. -2E. 11.2523244
Human Error Two general classificationsof error Skill-based errorSlip of ActionHuman Error Unintentional action thatresults in undesiredconsequenceProbabilities of Human ErrorSkill-based errorMemory LapseRule-based errorMistakeKnowledge-based error Attention diverted from a task Mistake Failure in planningNOPSEMA. (2020). Human Error. Retrieved September 11,2020, from human-error/Description of errorProbabilityUnfamiliar task performed at speed50%Failed task involving high stress level30%Inspection or verification of tasks with moderate stress20%Failed task conducted in the first 30 minutes of an emergency10%Failure to perform a check correctly5%Error in a routine operation where care is required1%Error during read-back0.5%Selection of wrong package (well labeled)0.3%Human-performance limit: Single person working alone0.01%Human performance limit: team of people performing a well designed task0.001%Cohen, M. R., Smetzer, J. L., & Westphal, J. E. (2012). Riskmodels to improve safety of dispensing high-alert medications incommunity pharmacies. Journal of the American PharmacistsAssociation, 52(5), 584-602. doi:10.1331/japha.2012.1014526Marx, D. (2014). Whack-a-mole: The price we pay for expecting perfection. Plano, TX: By Your Side Studios.Smetzer, J., R.N., B.S.N., FISMP. (2020, September 11). Managing Behaviors in a Just Culture. Lecturepresented at Medication Safety Certificate nt of Human ErrorAt-Risk Behavior Ask yourself Behavioral choice Did the employee’s choices align with the task at hand? Operate with known risks ResponseEmployee “Drifting” Actions become habitual Support the employee Respond to personal performance factors andbehavioral choices Reasons for at-risk behavior Rules are weak Decreased perception of risk Quicker rewardSystem Examine steps within the system Respond to steps that may have contributed to humanerror No harm no foulMarx, D. (2014). Whack-a-mole: The price we pay for expecting perfection.Plano, TX: By Your Side Studios.Smetzer, J., R.N., B.S.N., FISMP. (2020, September 11). Managing Behaviorsin a Just Culture. Lecture presented at Medication Safety Certificate Program.27At-Risk BehaviorManaging At-Risk Behavior Most-problematic behavior Everyone engages in behavior, but not everyone is caught First-order problem solving is used for those who are caught Encourage reporting of at-risk behaviors Investigate the behavior How often does this behavior occur Evaluate the system and the steps in the system Identify “upside-down” consequences “Fix it and forget it” mentality Create workarounds to speed up process Never report the problem so it can be addressed for othersEmployee Coach and support Mentor colleagues to prevent risk in the future Second-order problem solving is necessary for long-termsolutionsMarx, D. (2014). Whack-a-mole: The price we pay for expecting perfection.Plano, TX: By Your Side Studios.Smetzer, J., R.N., B.S.N., FISMP. (2020, September 11). Managing Behaviorsin a Just Culture. Lecture presented at Medication Safety Certificate Program.System Respond to system flaws to prevent future risks Reduce barriers that may impede compliance Add barriers to deter noncompliance29Marx, D. (2014). Whack-a-mole: The price we pay for expectingperfection. Plano, TX: By Your Side Studios.Smetzer, J., R.N., B.S.N., FISMP. (2020, September 11). ManagingBehaviors in a Just Culture. Lecture presented at Medication SafetyCertificate Program.305
Reckless BehaviorDifferentiating between at-risk and recklessbehaviors Conscious disregard of risk At-Risk Risk is substantial and unjustified Reckless Perception of risk decreases asexperience increases Does not choose to place othersin harm’s way Believes risk is justified orinsignificant Behavior motivated by perceivedconsequences Expectation of staff is toavoid behavior at all costs Harm does not have toresult to classify behavior asrecklessMarx, D. (2014). Whack-a-mole: The price we pay for expecting perfection. Plano, TX: ByYour Side Studios.Smetzer, J., R.N., B.S.N., FISMP. (2020, September 11). Managing Behaviors in a JustCulture. Lecture presented at Medication Safety Certificate Program.Fllickr.com/photos/gangliuphotos Understands risk is substantialChooses behavior intentionallyUnable to justify behaviorUnjustified risk does not agreewith social norms Puts ones self before othersSmetzer, J., R.N., B.S.N., FISMP. (2020, September 11).Managing Behaviors in a Just Culture. Lecture presented atMedication Safety Certificate Program.31Managing Reckless Behavior32The Three Behaviors Reckless behavior cannot continue Punishment must occur to prevent future harmHuman ErrorAt-Risk BehaviorReckless BehaviorProduct of system designand behavioral choicesChoice: risk is perceived asinsignificant or justified.Conscious decision to ignoresubstantial riskManage Through:Manage through: Manage through changesin:Employee Remedial or disciplinary actionsSystem Evaluate system design Respond to system flaws to prevent future aining Removing incentives forat-risk behaviorCreating incentives forhealthy behaviorsIncreasing situationalawarenessConsoleSmetzer, J., R.N., B.S.N., FISMP. (2020, September 11).Managing Behaviors in a Just Culture. Lecture presented atMedication Safety Certificate Program.CoachRemedial actionDisciplinary actionPunishMarx, D. (2014). Whack-a-mole: The price we pay for expecting perfection.Plano, TX: By Your Side Studios.Smetzer, J., R.N., B.S.N., FISMP. (2020, September 11). Managing Behaviorsin a Just Culture. Lecture presented at Medication Safety Certificate Program.3334TechnicianWhich of the following examplesrepresents at-risk behaviorElements of Just Culture1. Forgetting to adjust times on an order prior to verification Aligning values and expectations2. Reading back orders on rounds prior to verifying them Making better behavioral choices3. Ignoring medication DURs during product verification Learning to think systematically4. Following a policy to prevent missing a step Designing better systems35366
Thinking SystematicallyElements of Just Culture Examines processes holistically Aligning values and expectations Helps unify all parties understanding of a concept Making better behavioral choices Allows for deeper insights into situations by identifyinginteractions between groups Learning to think systematically Designing better systems Removes blame from any one group or person and focuseson shared accountabilitySnedaker, S. (2018, January 07). Lean Leader #4 - Think Systematically.Retrieved September 20, 2020, from 7/Lean-Leader-4---Think-Systematically37System Design38Designing Reliable Processes Goal: Design reliable systems that decrease possibility ofhuman error System reliability Refers to level of performance over timeIdentify theProblem Healthcare has a reliability of 10-1-10-2 Aviation has a reliability of 10-6 Nuclear power plants must have a reliability of 10-6 before even beingbuiltVisualizethe ProcessSegmentthe ProcessStandardizeand Simplifythe ProcessDevelop aBack-upPlanNolan T, Resar R, Haraden C, Griffin FA. Improving the Reliability of Health Care. IHI Innovation Serieswhite paper. Boston: Institute for Healthcare Improvement; 2004.Resar, R. (2006, August). Making noncatastrophic health care processes reliable: Learning to walkbefore running in creating high-reliability organizations. Retrieved September 21, 2020, 955343/39Designing Reliable Processes40Identify the Problem Move too quick from understanding the problem toimplementing a solution True cause may be confused with symptom of the root causeIdentify theProblemVisualizethe ProcessSegmentthe ProcessStandardizeand Simplifythe Process Tools for identifying root causeDevelop aBack-upPlanInstitute for Healthcare Improvement. (2019). PatientSafety Essentials Toolkit. Institute for HealthcareImprovement. 5 whys Fishbone Diagram Failure Modes Effects Analysis (FMEA)41Institute for Healthcare Improvement. (2019). PatientSafety Essentials Toolkit. Institute for HealthcareImprovement.427
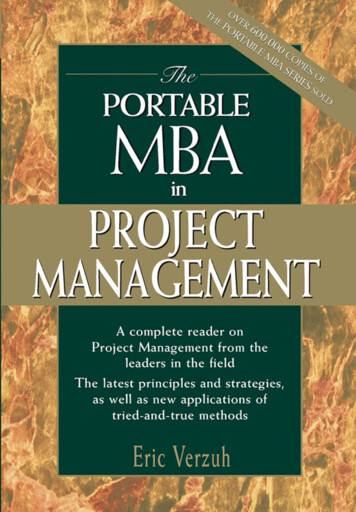
5 WhysFishbone (Ishikawa) DiagramEnvironmentPeople Gather a interprofessional teamwho are familiar with theproblemClocksLab SecretaryLab techInaccurateHeavy workloadRoundingUnavailable when MD calledTranscription errorDispatcher Define the problemNo tracking processLab suppliesUnnecessary stepsUnavailableSpecimen vialsSpoiledToo many peopleinvolvedUnavailableLong testresults timeLab EquipmentHandling in lab Ask the question “why?” at least5 times and provide answerseach timeCapacitySlowDo-overPhone SystemCapacityDownSpoiled Examine the best way to solvethe problemMaterialsInstitute for Healthcare Improvement. (2019). PatientSafety Essentials Toolkit. Institute for HealthcareImprovement.MethodsEquipmentInstitute for Healthcare Improvement. (2019). PatientSafety Essentials Toolkit. Institute for HealthcareImprovement.43Failure Modes and Effects Analysis44Failure Modes and Effects Analysis Proactive approach to preventing harmSteps inProcessFailureModeOrdersplaced onpatientadmissionMed 0)LikelihoodofDetection(1-10)Severity(1-10)Risk ProfileNumber(RPN)Actions toReduceOccurrencePatient gets Patienttwo doses of already tookwarfarindose ofmedicationtoday8510400RequireMed Recwithin 2hours ofadmitMed Recnotcompletedfor multiplehours51630Createprioritizationfor med recs Useful for evaluating new processes before implementation Multidisciplinary team predicts where, how, and to whatextent a system may fail Ability to correct processes before they fail to prevent harmLack ofprioritizationtool for MedRecs4546TechnicianWhich of the following is true of FMEAswhen identifying root causes?Designing Reliable ProcessesA. Requires collaboration among an interdisciplinary teamB. Places blame on a single person or departmentC. Retroactively addresses failure modesD. The risk prioritization score helps the team prioritize failuremodesIdentify theProblemVisualizethe ProcessSegmentthe ProcessStandardizeand Simplifythe ProcessDevelop aBack-upPlanE. Both A and D47Institute for Healthcare Improvement. (2019). PatientSafety Essentials Toolkit. Institute for HealthcareImprovement.488
Visualize the ProcessProcess Mapping Identify the first and last step in the process Visual representation of the steps required to complete aprocess Create a high level flow diagram of all steps between thefirst and last Useful informing all members of the process Brainstorm all steps in a given process Identify all potential room for error Prioritize those which pose significant risk or may lead to additional error Connect steps to each other Identify steps in the process which may lead to problemsInstitute for Healthcare Improvement. (2019). PatientSafety Essentials Toolkit. Institute for HealthcareImprovement.Process MappingPharmacistcontactsclinical teamforclarificationReach out toclinical teamagainNoProblemcorrected?50Designing Reliable ProcessesPharmacistreviewsorderPhysician placesmedication orderInstitute for Healthcare Improvement. (2019). PatientSafety Essentials Toolkit. Institute for erifiedIdentify theProblemYesVisualizethe ProcessSegmentthe ProcessStandardizeand Simplifythe ProcessDevelop aBack-upPlanYesInstitute for Healthcare Improvement. (2019). PatientSafety Essentials Toolkit. Institute for HealthcareImprovement.51Segment the Process52Designing Reliable Processes Identify the entire population affected by the process beingchanged Who does this problem effect? Select a segment of the population to test changeIdentify theProblem Employees who are willing to engage Volume high enough to allow for daily change and continuedmeasurement of changeInstitute for Healthcare Improvement. (2019). PatientSafety Essentials Toolkit. Institute for HealthcareImprovement.53Visualizethe ProcessSegmentthe ProcessStandardizeand Simplifythe ProcessDevelop aBack-upPlanInstitute for Healthcare Improvement. (2019). PatientSafety Essentials Toolkit. Institute for HealthcareImprovement.549
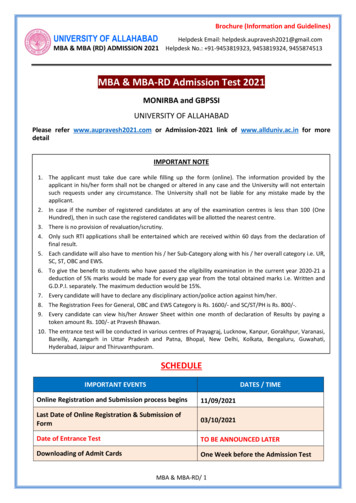
Standardize and SimplifyTools for Standardization and Simplification Identify which defect you want to fix and why Involve people who do the work Ask the following questions to standardize the process Automation Force functions and fail safes Limit access or centralize workWho will complete the task?What is the task they will complete?When will they complete the task?Where will they complete the task?How will they complete the task?What will they use to complete the task? Add redundancies or cross checks Increase AwarenessInstitute for Healthcare Improvement. (2019). PatientSafety Essentials Toolkit. Institute for HealthcareImprovement.Smetzer, J., R.N., B.S.N., FISMP. (2020, September 11).Managing Systems in a Just Culture. Lecture presented atMedication Safety Certificate Program.55Designing Reliable Processes56Develop a Back-up Plan Not all plans will be implemented successfully Identify which processes require a back-up plan Processes with multiple identified opportunities for errorIdentify theProblemVisualizethe ProcessSegmentthe ProcessStandardizeand Simplifythe Process Ask yourself the same questions use during the standardizeand simplify stepDevelop aBack-upPlan Incorporate your plan into the existing workflowInstitute for Healthcare Improvement. (2019). PatientSafety Essentials Toolkit. Institute for HealthcareImprovement.Institute for Healthcare Improvement. (2019). PatientSafety Essentials Toolkit. Institute for HealthcareImprovement.57Putting it all together58Visualize the ProcessPatient AL has just woken up from surgery in the surgical ICUand is in the worst pain of her life. The physician places anorder for ketamine 30 mg for pain. The nurse rememberedketamine is overrideable in the ICUs so nursing does not haveto wait for pharmacy to verify the order. Two strengths ofKetamine are stocked in the Omnicell: 10 mg/mL and 100mg/mL. The nurse pulls the 100 mg/mL and pulls up 3 mL toadminister the patient’s dose. During reconciliation, the nurserealizes the mistake and alerts the physician. The patient isprepared for intubation in case loss of airway occurs.Patientarrives fromsurgeryNurseadministerspainmedication59Patient is inpainYesPainordersplaced?NoNurseasks MDfor painorderMD givesnurse a verbalorder and sayshe’ll place anorder ASAPNurseoverridesmedicationfrom ADCWrongstrength ofmedicationadministeredto patient6010
Pharmacist & TechnicianWhich of the following could be potentialoptions for simplify and standardize theprocess?Identify Potential Breakdowns in theProcessPatientarrives fromsurgeryNurseadministerspainmedicationPatient is inpainYesPainordersplaced?NoNurseasks MDfor painorderMD givesnurse a verbalorder and sayshe’ll place anorder ASAPNurseoverridesmedicationfrom ADCWrongstrength ofmedicationadministeredto patientA. Develop standardized admission order sets for all patientsin the ICUB. Decrease the number of overrideable medications fromADCsC. Destock one strength of ketamine from ADCsD. Place “High Alert” stickers on different strengths ofketamine in ADCsE. Require witness for all medications overridden from theADCsF. All of the above6162In Summary Just culture empowers employees to proactively monitoringand report safety events Requires teams to practice shared accountability and thinksystematically about safety eventsQuestions? Increases the safety and quality of care we provide to ourpatientsK yl e F i n n e r t y P h a r m D , M B A , P GY- 2 HS PA L Re si d e n tUn i ve r si t y o f Ut a h He a l t hK yl e . f i n n e r t y@ h sc .Ut a h .e d u636411
To Err is Human: Building a Safer Health System 13 Published in 2000 by IOM Highlights medical errors in American health systems Called for national efforts to improve the safety of healthcare "the problem is not bad people in health care it's good people working in bad systems that need to be made safer."