Transcription
B U F FA L OH O S P I TA L2011 Annual ReportCelebrating 2010 AccomplishmentsQuality, Patient Safety, and Performance Improvement2010 Report Buffalo Hospital1
Building a Culture of Excellenceand Safety at Buffalo Hospital2010 was a year of great strides at Buffalo Hospital. Overall quality, patient safety, patient experienceand performance improvement outcomes demonstrated a culture dedicated to achieving and sustainingexcellence.Buffalo Hospital is committed to transparency and to meeting the needs and expectations of ourpatients. Sharing performance results empowers patients, staff, leaders and stakeholders to makeinformed health care choices. To improve, we have to measure. This report reflects the enormous effortthat goes into measurement and serves as a means of conveying the organization’s accomplishments inkey areas.In addition to the information provided in this annual report, the organization realized the followingsignificant accomplishments in 2010: Thomson Reuters recognized Buffalo Hospital as one of the nation’s Top 100 Hospitals. BuffaloHospital was also one of 23 hospitals honored with the Everest Award, which recognizes both thehighest current performance and the fastest long-term improvement over five years. The Minnesota Department of Health designated the Buffalo Hospital Emergency Department as aLevel III Trauma center. Staff were recognized by the Minnesota Hospital Association’s “Good Catch for Safety” award fortheir diligent efforts in identifying significant patient safety opportunities for improvement. Allina recognized both the Birth Center and Med-Surg for their significant improvements in PatientExperience as demonstrated with significant improvement in HCAHPS scores. The American Association of Blood Banks surveyed and accredited the hospital laboratory foranother two years. The Minnesota Board of Pharmacy conducted an unannounced survey and inspection of the BuffaloHospital pharmacy in September of 2010 with no significant findings.The quality, safety and service work completed in 2010 serves as a strong foundation for the strategicinitiatives which lie ahead in 2011. This work is representative of a comprehensive quality and safetyprogram which encompasses the organization through the efforts of physicians, staff and leaders. As wecelebrate our 2010 accomplishments, we also recognize that we need to continually strive to meet theneeds of our patients and improve outcomes of care.Gretchen Frederick, RN, MADirector of Patient CareBuffalo Hospital2Buffalo Hospital 2010 ReportCorey Martin, MDDirector of Medical AffairsBuffalo Hospital
Table of ContentsC L I N I C A L Q UA L I T YQuality Scorecard. 4Core Measures & Readmission ReductionAcute Myocardial Infarction Optimal Care. 5Heart Failure Optimal Care. 5Pneumonia Optimal Care. 6Surgical Care Optimal Care. 7Outpatient Acute Myocardial Infarction/Chest Pain Measures. 8Outpatient Surgical Care Core Measures. 9Stroke Optimal Care. 10Readmission Reduction. 11SERVICEPatient Experience of CarePatient Satisfaction. 13Communication with Doctors. 14Pain Management. 15PAT I EN T S A F E T YPatient Safety CultureSafety Culture Survey. 16Patient Visitor Safety/Near Miss Reporting. 17Falls. 18Adverse Health Events/Critical Event Reviews. 19RE GUL ATO RYAccreditation and CertificationRegulatory and Accreditation Readiness. 20P E RF O R MA N C E I M PROV E M E NTDepartmental Performance Improvement2010 Accomplishments. 212010 Report Buffalo Hospital3
Quality and Patient SafetyScorecardCARE: Core Measures & Readmission Reduction2010Goal1st Qtr20102nd Qtr20103rd Qtr20104th Qtr2010Acute Myocardial Infarction (AMI) Optimal Care95%100%100%100%No ptsCongestive Heart Failure (CHF) Optimal Care95%92%94%100%100%Pneumonia (PN) Optimal Care95%96%89%82%92%Surgical Care Improvement Project (SCIP) Optimal Care90%96%97%99%92%Outpatient SCIP95%100%100%100%92%Outpatient AMI - ASA on Arrival95%100%100%100%95%Outpatient AMI - Median Time to EKG10 mins10 mins10 mins9 mins6 minsHeart Failure Re-admission Rate 17%13.3%33.3%40.0%23.1%Pneumonia Re-admission Rate 14%7.7%16.7%20.0%3.7% 10.6%0%100%50%No ptsInpatient mortality rate per 100 IP discharges0.600.700.650.480.51SERVICE: Patient Experience2010Goal1st Qtr20102nd Qtr20103rd Qtr20104th Qtr2010Patient Experience - Inpatients rating BH a 9 or 1064%61.1%69.2%73.9%69.0%Patient Experience - Outpatient Overall % Excellent51.0%50.0%49.5%51.0%51.2%Patient Experience - Pain Management Score71.9%67.3%73.8%72.1%69.2%Patient Experience - Physician Communication Score85.2%79.8%81.7%81.4%77.2%Grievances - Inpatient (Rate per 1000 adjusted pt. days) 1.000000Grievances - Emergency Department (Rate per 1000 ED visits) 3.501.170.550.700.74SAFETY2010Goal1st Qtr20102nd Qtr20103rd Qtr20104th Qtr2010Falls: Falls Rate (overall) per 1000 IP days 2.651.821.262.512.48Falls: Harmful falls rate per 1000 IP days 1.130.61000.62Hand Hygiene – Room Entry 90%83.7%72.1%80.2%81.4%Hand Hygiene – Room Exit 90%89.5%72.2%80.0%80.4%Hospital acquired C-Diff rate per 10,000 inpatient days12.6601.26000.260.610.530.480001AMI re-admission RateMedication error rate (overall) per 1000 doses chargedAdverse Health Events4Buffalo Hospital 2010 Report0
Core Measures Optimal CareInfarction (AMI), Heart Failureand Pneumonia Optimal CareDefinitions: Core Measures- Auniform set of measures based onbest practice guidelines which arenationally accepted standards ofcare across all hospitals. OptimalCare- Percent of patients receiving allinterventions appropriate totheir care.Clinical QualityMeasure: Acute MyocardialInclusions: Inpatients with aprincipal discharge diagnosis ofAMI, Heart Failure, or Pneumonia asdefined by the Centers for Medicareand Medicaid Services (CMS).Exclusions: Outpatients with thesame diagnoses; patients 18 yearsof age, and other measure-specificexclusions as defined by CMS.Goal: Overall average optimal carescore of 95% for AMI, Heart Failureand Pneumonia combined.Data Source: Medstat Database;QIWA ReportsSummary: The optimal care goalfor 2010 was met 2/4 quarters in2010. The overall end of year averagewas met at 95%. Core measures arechallenging due to unpredictable,often low volumes. Concurrentcase monitoring with real timefeedback/education to nurses andphysicians was sustained. The QualityDepartment and MedSurg/SCUPatient Care Supervisor work togetheras a team to assure a seamless processfor ongoing core measure compliance.2010 Report Buffalo Hospital5
Core Measures Optimal Care continuedData was shared on a quarterly basis with staff, hospital leadership, medical staff committees, and the Boardof Directors. The core measure leads participated in regularly scheduled Allina meetings/conference calls,implementing best practices based on Allina system tests of change.Core measures will remain an Allina and Buffalo Hospital strategic goal in 2011. Efforts will be focused onsustaining 2010 achievement. Additional core measures work planned for 2011: Increase use of standardized core measure order sets. Addition of Pediatric Asthma Core Measures. Plan for retirement of pneumonia immunization measures with addition of a globalimmunization measure set in 2012.Leads: Val Enter/Amanda Duerr6Buffalo Hospital 2010 Report
Surgical Care ImprovementProject Optimal CareClinical QualityMeasure: Surgical Care Improvement Project (SCIP)Optimal CareDefinitions: Core Measures- A uniform set ofmeasures based on best practice guidelines whichare nationally accepted standards of care across allhospitals. Optimal Care- Percent of patients receivingall interventions appropriate to their care.Inclusions: Antibiotic administration timing priorto incision, appropriate antibiotic selection, andtimely discontinuation of antibiotic (for surgical casetypes: hip and knee arthroplasty, colon resection, andabdominal/vaginal hysterectomy); hair removal, betablocker administration for patients on beta-blockersat home, VTE prophylaxis, urinary catheter removaland perioperative temperature management forselected surgical populations.Goal: 90%Data Source: Medstat Database; QIWA ReportsSummary: The SCIP optimal care goal was exceededin all four quarters in 2010, with an overall endof year score of 96%. Compliance sustainment isattributed to concurrent case monitoring with realtime feedback to nurses and physicians. In addition,Excellian order set changes, Best Practice Alerts(BPA’s), and flow sheet redesign have been ongoingwork to support care providers in attaining the goal.The SCIP score for 2011 will be compiled withthe heart failure, pneumonia and acute myocardialinfection measures. The overall optimal care goal forall four core measures will be 95%.Leads: Val Enter, Amanda Duerr, Jill BjornsonExclusions: Surgical procedures other than thoseidentified above.2010 Report Buffalo Hospital7
Outpatient Acute MyocardialInfarction Core MeasuresMeasure: Outpatient Core Measures - AMIInclusions: AMI/Chest Pain- Patientspresenting to the Emergency Department(ED) with chest pain and acute myocardialinfarction (AMI) who are not admitted forinpatient care. The chest pain measure is asample of all chest pain patients.Exclusions: AMIGoals: 95% points with AMI/Chestreceive ASA on arrival, Median timeto ECG 10 minutes.Data source: Medstat Database; QIWAReportsSummary: The majority of Buffalo HospitalAMI patients are cared for in the outpatientsetting (ED) rather than inpatient units.These patients are commonly transferred toa facility with cardiac specialists from theED. A large number of chest pain patientsare also seen in the ED. The outpatientcore measures are indicators of adherenceto evidence-based practice for this patientpopulation. Compliance with outpatientcore measures for AMI/chest pain is 98.6%for aspirin in chest pain patients, 100% foraspirin in AMI patients and 9 minutes formedian time to EKG.2010 quality improvement efforts focused on sustaining compliance with best practice care with focus on aspirinadministration on arrival.2011 quality improvement efforts will focus on sustaining and improving measure compliance: Improve median time to ECG time to less than National Benchmark of nine minutes. Improve documentation compliance for AMI/CP patients who have non-cardiac source of chest pain.Leads: Val Enter/Margo Binsfeld8Buffalo Hospital 2010 Report
Outpatient SCIPCore MeasuresClinical QualityMeasure: Outpatient Core Measures-SCIPInclusions: Outpatient surgical procedures (sample ofall outpatient procedures)Exclusions: Inpatient surgical proceduresGoals: 95% antibiotics administered within 1 hour ofincision time, 95% appropriate antibiotics orderedData Source: Medstat Database; QIWA ReportsSummary: Outpatient SCIP includes select surgicalprocedures performed on an outpatient basis. The sameinpatient procedure antibiotic measures for selectionand timing are applied to these outpatient procedures.The goal of 95% was met for 3/4 quarters in 2010,with an overall compliance of 98%. Strategies used forinpatient core measures were applied across outpatientprocedures.Leads: Val Enter, Jill Bjornson2010 Report Buffalo Hospital9
Stroke Optimal CareMeasure: Stroke Optimal CareDefinitions: Core Measures- A uniform set ofmeasures based on best practice guidelines whichare nationally accepted standards of care across allhospitals. Optimal Care- Percent of patients receivingall interventions appropriate to their care.Inclusions: Inpatients with a principal dischargediagnosis of ischemic or hemorrhagic stroke as definedby the Centers for Medicare and Medicaid Services(CMS).Exclusions: Outpatients with the same diagnoses;patients 18 years of age, and other measure-specificexclusions as defined by CMS.Goals: 75%Data Source: Outcome Science Database;QIWA ReportsSummary: A new measure set containing eightCMS stroke core measures was introduced in 2010.A system Stroke Core Measures Team was launchedwith active site lead participation in stroke education,10Buffalo Hospital 2010 Reportidentification of core measure failure trends, andExcellian support enhancements. In addition, amultidisciplinary site-based Stroke Core Measuresteam was initiated.Mandatory stroke education was provided to nursingstaff. Physicians also received stroke core measureeducation through department meetings and wereencouraged to use Allina stroke admission ordersets to promote best practice and core measurecompliance. Patient volumes for this measure setare small as most of these patients are transferredto a facility with neurology. Although the year-endoptimal care goal was not met at 52.6%, strokeoptimal care scores improved dramatically over thecourse of the year from 33% in 2nd quarter to 71.4%in 4th quarter. Additional stroke core measures workplanned for 2011: Sustain and surpass the substantial gains achievedin stroke core measures optimal care in 2010. TheAllina stroke core measures optimal care goal hasincreased to 85%.Leads: Katie Roers, Amanda Duerr and Stroke CoreMeasure Team
Readmission ReductionClinical QualityMeasure: Acute Myocardial Infarction (AMI), HeartGoals: Rolling 3-month average for Aug-Sept-Oct:Failure (HF) and Pneumonia (PN) 30 Day ReadmissionAMI: 10.6% Heart Failure: 17% Pneumonia: 14%Inclusions: Patients discharged with a primarydiagnosis of AMI, heart failure or pneumonia who arereadmitted for any diagnosis within 30 days of discharge(to any hospital).Data Source: Ace Web Reports, Qlikview DashboardExclusions: Elective procedures. Observation statusreadmissions.Summary: While the 2010 readmission rate goals wereachieved only for Pneumonia, the HF readmission ratedid improve slightly at year-end. The AMI readmissiongoal was not met, but included only four patients inthe denominator. Interventions initiated to support2010 Report Buffalo Hospital11
Readmission Reduction continuedreadmission reduction in 2010 included: Concurrent monitoring process developed to identify readmissions while in hospital. Care Management developed need assessment questionnaire for HF patients used during initial admission. Care Management referrals to cardiac rehab for HF patients started. Cardiac rehab assesses HF patients foroutpatient cardiac rehab referral.Work will continue in 2011 to optimize Excellian order sets and documentation templates, enhance ongoingeducation documentation throughout the patient’s stay, increase palliative care consults for HF patients, assurea low sodium (2 Gm) diet for all HF patients, hard wire teach back education by all disciplines and continueinterdisciplinary heart failure education.Leads: Val Enter, Gretchen Frederick and Readmission Steering Team12Buffalo Hospital 2010 Report
Overall Patient SatisfactionMeasure: Inpatient and OutpatientPatient SatisfactionHCAHPS Surveys (MedSurg,Specialty Care Unit, Birth Center)and Outpatient Allina Surveys(Emergency Department, Same DaySurgery, and Diagnostics).ServiceInclusions: Returned AdultExclusions: Outpatient services otherthan those identified as inclusions,inpatient pediatric unit.Goal: Inpatient: 64%Outpatient: 51%Data Source: Avatar web siteHCAHPS survey; Allina patientsatisfaction survey database, QlikviewDashboardSummary: Satisfaction goals weremet and far exceeded in 2010.Site-based teams were developedfor Patient Experience and PainManagement, with additionalparticipation in Allina-widecommittees for each of these aswell. Additional initiatives in 2010included: Leadership newspaper rounds onpatients. New care boards in all IP rooms. Staff hourly rounding on patients. Implementation of room service inBirth Center. Warm & welcoming training. Facility updates – creation of ahealing environment. Strong service recovery program.Leads: Katie Roers, GretchenFrederick2010 Report Buffalo Hospital13
Communication with DoctorsPatient SatisfactionMeasure: Communication with Doctors SatisfactionInclusions: Returned adult (Med Surg, Special CareUnit, Birth Center) HCAHPS surveys.Exclusions: Outpatient services other than thoseidentified as inclusions, inpatient pediatric unit.Goals: 85.2% rolling three month average forAug-Sept-OctData Source: Avatar web site HCAHPS surveySummary: The communication with doctorssurvey questions were selected as an Allina focusarea in 2010 to assist in increasing overall inpatientsatisfaction scores. Work at Buffalo Hospital hasfocused on: Developing hospitalist business cards with photos. Nurse-Physician Rounding.14Buffalo Hospital 2010 Report A plan for ongoing physician education wasdeveloped which included distribution of thesystem communication with doctors newsletter,inclusion of patient satisfaction information inmedical staff monthly meetings and launching theHospital Outstanding Patient Experience (HOPE)award recognizing exceptional physicians asrecognized by patients. Additional tactics included use of the Care Boardto identify the physician by name.While the annual goal was not achieved, significantwork was accomplished as the foundation forimprovement in 2011.Leads: Katie Roers/Gretchen Frederick/CoreyMartin, M.D.
Pain Management PatientSatisfactionServiceMeasure: Pain Management SatisfactionInclusions: Returned adult (Med Surg, Special CareUnit, Birth Center) HCAHPS surveys.Exclusions: Outpatient services other than thoseidentified as inclusions, inpatient pediatric unit.Goal: 71.9% rolling three month average forAug-Sept-OctData Source: Avatar web site HCAHPS surveySummary: This was the first year of a dedicatedsystem-wide pain experience initiative. Amultidisciplinary team was created at Buffaloto address patient pain experience goals. Therewere multiple system tactics which the site teamparticipated in: Nursing education (general and OB specific). Excellian enhancements, including redesign of painorder sets. Site-lead pain conference (Perspective on Pain). Revision of the patient pain brochure. Standardized Allina Care Boards were placed onMed-Surg, SCU and in the Birth Center.Leads: Katie Roers/Cindy Oquist and the PainExperience Team2010 Report Buffalo Hospital15
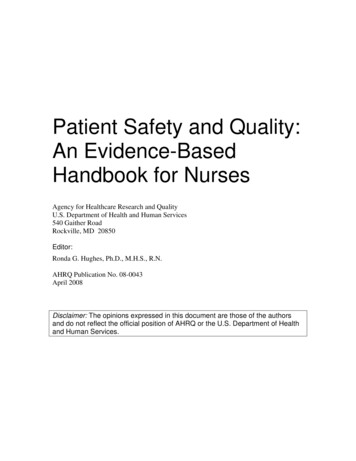
Safety Culture SurveyBuffaloAllina HealthSurvey Results November 2010HospitalSystemParticipants:50-99 bedBenchmarkHospitals2444,999338,607Overall perceptions of safety71%54%68%Frequency of events reported68%52%64%Supervisor/manager expectations & actions promoting safety85%67%77%Organizational learning – Continuous improvement79%64%73%Teamwork within units88%77%80%Communication openness73%58%63%Feedback & communication about error69%52%65%Nonpunitive response to error60%43%46%Staffing65%51%58%Hospital management support for patient safety80%60%74%Teamwork across hospital units67%53%60%Hospital handoffs & transitions51%41%48%Measure: Staff perception of patient safety cultureHospital Goals for 2011: Increase reporting of near misses and patientevents. Develop improved communication plan for sharingPVSR data and resulting actions.Data Source: AHRQ Survey on PatientSafety CultureSummary: In 2011, Allina chose to use the AHRQsurvey to evaluate our patient safety culture. Theoverall survey results for Buffalo Hospital were thesecond highest in Allina and above all NationalBenchmarks for hospitals of similar size. Results werereviewed by each department leader with staff andaction plans developed for departments whose scoreswere below benchmarks. This survey will be repeatedon an annual basis and scores trended from year toyear.Leads: Val Enter, Manager of Quality, Risk & PatientSafety16Buffalo Hospital 2010 Report
Patient Visitor Safety Event/NearMiss Reporting (PVSR)Miss ReportingInclusions: All inpatients, outpatients andvisitors.Exclusions: Employee or campus partner clinicpatient events.Patient SafetyMeasure: Patient Visitor Safety Event/NearGoals: 10% increase in reporting from 2009 rateData Source: Patient Visitor Safety Report(PVSR) DatabaseSummary: The majority of the events with harmfall into the temporary/minor harm category.Strategies used to increase PVSR reportingincluded communications in Patient Care NotesNewsletter, leadership support via patient safetymessages in the president Friday newsletter andmanager weekly emails, and completion of thepatient safety culture survey information sharingwith staff.Reporting for all events and good catch/nearmiss events increased significantly in 2010 withgoal achievement attained. The majority of theseevents are coded as no harm with a consistent4% harm rate for the past three years. Eventswith no severity assigned are laboratory reportedevents which have a coding process specific tothe department. The Laboratory Departmentis a strong patient safety advocate with eventreporting surpassing all other departments.Hospital Goals for 2011: 8% increase in Near Miss Reporting from2010 rate. Continue to increase reporting of patientevents. Implementation of leader rounding on staffwith patient safety questions.Leads: Val Enter, Manager of Quality, Risk& Patient Safety2010 Report Buffalo Hospital17
FallsSummary: The 2010 goal was achieved with aMeasure: Inpatient Falls/Falls with HarmInclusions: Inpatient FallsExclusions: Outpatient fallsGoal: Overall Falls Rate 2.65 falls per 1000 patient days;Harmful Falls Rate 1.13 falls per 1000 patient days.Data Source: Patient days from financial data; fall data fromClarity and PVSR databaserate of 0.47 harmful falls per 1000 patient daysor 3 inpatient falls with harm. The 2010 goalfor overall rate of falls was also achieved with arate of 2.17 falls per 1000 patient days or 14 falls.Interventions which assisted in goal achievementinclude: Real time audits done to measure required fallinterventions. Increased the representation from outpatientdepartments on falls team. Developed guidelines to match interventionswith Hendrich II assessment items. Met with ancillary departments to share fallreduction strategies, creating a safety net ofhealthcare workers to assist in fall reduction. Emphasis on toileting with patient rounding. Implemented post-fall huddle process. Reinforced staff education on use of thefall risk tool, specifically the get-up-and-gomeasurement. Staff shared “real life” accounts of experienceswith patient falls and learnings from falls.These accounts were communicated to staff innursing newsletter and staff meetings.Work will continue in 2011 in alignmentwith Allina system-wide strategies includinga focus on: equipment needs, vitamin D use,scheduled toileting and Within Arms Reachinitiatives, consistent messaging on Care Boards,development of a fall prevention toolkit, falleducation to all staff, role modeling of verbalcontracts and pharmacy review for medicationimpact.Leads: Katie Roers/Raelene Fairchild and theFall Prevention Team18Buffalo Hospital 2010 Report
Adverse HealthEvents/Critical Event ReviewsPatient SafetyDuring 2010, six Critical Event Reviews (CER) were conducted (3-newborn events, violent patient incident, fallwith injury, and an ED multiple trauma incident). These events included one reportable Adverse Health Event(AHE), a fall with injury requiring return to surgery. AHEs are those events deemed reportable by MN statute144.4065. Adequacy of staffing was assessed for all CERs. No staffing concerns were identified. Learnings fromCER’s were shared with staff as appropriate to prevent future occurrences.In 2010, Buffalo Hospital participated in the Minnesota Hospital Association “Calls to Action” for Safe Skin,Safe from Falls, Safe Site, Safe Count, and Safe Account. Buffalo has completed the improvement road map forfour of the calls to action, receiving a patient safety excellence award for these initiatives. Work continues onthe Safe Account initiative with plans to complete in 2011.Failure Mode Effect AnalysisTwo Failure Mode Effect Analysis (FMEA) were conducted on the universal protocol, one in surgical servicesand one in the diagnostic imaging department. Action plans were shared with the Allina system as a precursor toredesign of the universal protocol checklist/transition to the World Health Organization (WHO) checklist.Lead: Val Enter, Manager of Quality, Safety & Risk Management.2010 Report Buffalo Hospital19
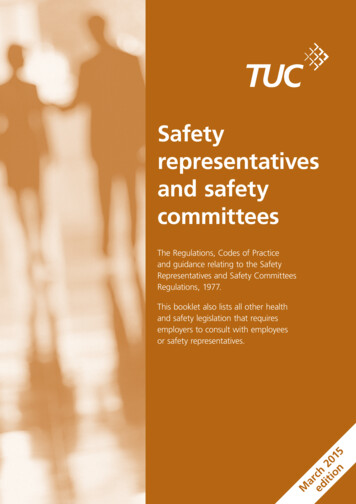
Regulatory &Accreditation ReadinessNumber of JointCommission StandardsNumber ofStandards in FullCompliance in 2010281278Summary3 at less than 66% compliance – Hand hygiene underInfection Control and the National Patient Safety Goal– Patient identification (patient banding in the ED and patientbeing entered into the EMR in the ED under wrong name)Measure: Compliance with regulatory andaccreditation standardsInclusions: Standards for which non-compliance orpartial compliance is determined and plans of actiondevelopedExclusions: Standards considered compliant or easilybrought into complianceGoals: Successful Allina Internal Regulatory Survey. Annual completion of the Joint CommissionPeriodic Performance Review.Data Source: Survey results from Allina Internal RegulatorySurvey. Chapter lead identification of partially compliant/non-compliant standards.Buffalo Hospital actively maintains compliance toThe Joint Commission (TJC) and CMS (Centers forMedicare and Medicaid Services) requirements withinthe framework of Allina’s Regulatory Reliability modelwhich supports ongoing regulatory compliance andsurvey readiness. Leads are identified for each of theJoint Commission chapters and work collaborativelywith the Regulatory Lead to provide oversight andsuccessful preparation and submission of the 2010Periodic Performance Review (PPR). This includesthe development of corrective action plans to addressreported areas of non-compliance. The correctiveaction plans were submitted and accepted by The JointCommission during the PPR follow-up phone call.Buffalo Hospital successfully transitioned to the Allina20Buffalo Hospital 2010 ReportRegulatory Accreditation System (ARAS) tool. Thistool is an electronic program that assists in managingongoing compliance to TJC standards. The tool isdesigned to score compliance and document supportingevidence for each of TJC standards and includes theability to enter corrective action findings and planswhen standards are identified as non-compliant. TheARAS tool is currently utilized by the Regulatory Leadfor documentation compliance input from ChapterLeads and for the annual PPR preparation.In March of 2010, Buffalo Hospital had a successfultwo day Allina internal regulatory accreditation surveywhich was coordinated and conducted by the Allinaregulatory leads from across the system. The surveys aredesigned to replicate an actual Joint Commission surveyby incorporating the same patient tracer methodologyutilized by TJC. Non-compliant internal findings wereevaluated by responsible individuals and correctiveactions were put in place to bring the requirements intocompliance. The internal survey findings were enteredinto the ARAS tool and became helpful adjunctsduring the preparation of the 2010 PPR.Additional regulatory readiness activities in 2010included the development of numerous educationalmaterials, such as the monthly Joint Commissioncalendars, 2011 NPSG poster, information submittedto Buffalo Hospital publications such as Patient CareNotes and This Week at Buffalo. These educationalmaterials are used to help prepare all employees andphysicians for a successful survey which will occurbefore the end of 2011.Lead: Pat Marschel, Quality Improvement Specialist/Regulatory Lead
Med-Surg/SCU Initiated physician/nurse rounding process. Standardizing nurse-to-nurse handoffs with PACU andImaging. Improved ED admit process. Behavioral Health education and pathway use. Trauma education for SCU nurses. Strengthening our Nursing Governance Model. Initiated processes to help improve the care experiencefor surgical ortho and peds patients. Safe Patient Moving fair held in October to educatestaff on moving patients safely – for the patient andthe staff person.Emergency Department Developed a quality scorecard for ED. Installed patient satisfaction vendor software to assist inanalyzing ED satisfaction at discharge and identify areasof improvement. Results shared with providers and staffregularly. Registration and ED staff worked collaboratively toimprove patient banding processes. Suicide Risk Screening increased from 50% to 97%compliance. Weekend staffing hours were increased and shifts timesaltered to better cover times of high census. New model of care called “pull til you’re full” trialedin November, and proved to decrease benchmark timesfrom the current average of 34 minutes to 27 minutes.This model will be fully implemented in January of2011. Implemented 24/7
Summary: Outpatient SCIP includes select surgical procedures performed on an outpatient basis. The same inpatient procedure antibiotic measures for selection and timing are applied to these outpatient procedures. The goal of 95% was met for 3/4 quarters in 2010, with an overall compliance of 98%. Strategies used for