Transcription
CQSPI:Clinical Quality, Safety &Performance ImprovementMichael Edmond, MD, MPH, MPAChief Quality Officer1
BioMichael B. Edmond, MD, MPH, MPA is the Chief Quality Officer and AssociateChief Medical Officer for University of Iowa Health Care and Clinical Professor ofInfectious Diseases at the University of Iowa Carver College of Medicine. Hepreviously served as the Richard P. Wenzel Professor of Internal Medicine, Chair ofthe Division of Infectious Diseases, and Hospital Epidemiologist at VirginiaCommonwealth University in Richmond.He is a graduate of the West Virginia University School of Medicine (MD), theUniversity of Pittsburgh Graduate School of Public Health (MPH), and the VirginiaCommonwealth University School of Government and Public Affairs (MPA). He wasa resident and chief resident in Internal Medicine at West Virginia UniversityHospitals. He then completed a fellowship in Infectious Diseases at the University ofPittsburgh Medical Center and a fellowship in Hospital Epidemiology at theUniversity of Iowa College of Medicine.Dr. Edmond’s areas of research focus on the epidemiology of healthcare-associatedinfections and the public policy implications of infection prevention. He has published350 papers, abstracts and book chapters, and co-writes a blog entitledControversies in Hospital Infection Prevention.2
Vision To ensure every patient highquality, compassionate care, freeof all preventable harm3
Mission To effectively and continuously measure the state of quality,value and safety at UIHC To proactively seek latent causes of harm and effectivelymitigate their risk To implement evidence-based best practices for improving thequality and safety of patient care To promote stewardship of healthcare resources To ensure regulatory compliance To serve as an educational resource To create and disseminate knowledge in infection prevention,healthcare quality, and patient safety To enhance the visibility of quality and safety internally, and thereputation of the institution externally4
High value healthcare is now the goal Components of value:– Quality (outcomes)– Cost– Patient experience5
CQSPI StructureChief Medical OfficerDr. Theresa BrennanChief Quality OfficerDr. Michael EdmondAssociate CQO,Surgical & Procedural AreasDr. John CromwellAssociate CQO,Children’s HospitalDr. Erik EdensQuality Executive CommitteeAssociate CQO,Adult Inpatient AreasDr. Kim StaffeyDirector, CQSPIBeth HannaInfectionPreventionHospitalEpidemiologist:Dr. Michael EdmondInfectionPreventionists:Nancy CoulterLaurie LederJean PottingerDeb JensenMary Beth KuklaAntimicrobialStewardshipDirectors:Dr. Dilek InceDr. Brian HoffAssociate HospitalEpidemiologists:Student HandDr. Dan Diekema Hygiene ObserversDr. Nathan PriceSupportAdministrative: Neana Clark, Sam MitchellDr. Teresa BrennanDr. Michael EdmondDr. John CromwellDr. Erik EdensDr. Kim StaffeyDr. Maia HightowerDr. Rashmi MuellerDr. Sharon TuckerCindy DawsonEmily WynnBeth HannaPerformanceImprovementRegistry Coordinators:Diana RettigTonya NaughtonQuality Specialists:Angie OvertonDr. Sue DasovichTim RossiDr. Debra PiconeAmy EischensDr. Jennifer McDanelLori FoxenDr. Susan BerendsPeggy WarrenKim HermiePatient SafetySafety Specialists:Jill FisherJonathan BothellHR: Heidi BodensteinerIT: Mark Renshaw, Mark Ackman, Barbara ZillesData Analysts: Anita Frazier, Vicki IbarraInfography: Jeff Kritzman6
CQSPI DomainsInfection Prevention Healthcare-associated infections Resistant organisms Community acquired infections of publichealth importance Hand hygiene compliance Education related to outbreaks,exposures or infection prevention Regulatory compliance for infectionprevention Infection prevention consultation inconstruction projectsPatient Safety Review & investigate events entered inthe Patient Safety Net (PSN) system Safety culture Publicly reported Patient Safety Indicators& Hospital-Acquired Conditions Failure Modes and Effects Analysis(FMEA) and Root Cause Analysis (RCA) Safety educationPerformance Improvement TJC/CMS core measuresBlood utilizationUHC metricsIowa Hospital AssociationClinical Dept PI projectsNational registries:o National Surgical Quality ImprovementProgram (NSQIP): Adult & pediatrico The Society of Thoracic Surgeons: Adult &pediatric CT surgeryo Virtual Pediatric Intensive Care Unit Systemso Strokeo ResuscitationAntimicrobial Stewardship Optimize antimicrobial usage through: Guidelines Formulary optimization Prospective audit and feedback Education Management of antibiotic shortages7
QI and safety activities organized along 4 verticalservice hildren’s& Women’sTeamAdultAmbulatoryTeam8
Quality & Safety Service Domains Each of the 4 domainscreates a cross-functionalteam (a group of people withdifferent functional expertiseworking toward common goals) Each team is led by anAssociate CQO and aNursing Leader Team members:– Physician Value Officers– Medical Directors– Nurse Managers– Physician Informaticist– PI/Safety Engineer(s)– Operations ExcellenceEngineer– Infection Preventionist– Office of Patient ExperienceRepresentative– Pharmacist9
Quality & SafetyOversight CommitteeChief Medical Officer & Chief Nursing OfficerChief Quality ildren’s& Women’sTeamAdultAmbulatoryTeamNursing Quality/SafetyGME Quality/SafetyAntimicrobial StewardshipCardiovascular Noninvasive Diagnostics/Imaging, PICC ServiceDialysis ProgramsPathology, RadiologyCQSPI Support (Administrative, IT, Data Analytics)10
Quality Oversight StructureHospital Advisory CommitteeCriticalCare SCHIM SCEnvironmentof Care SCQuality & SafetyExecutive CommitteeInfectionControl SCNursingQI & SafetyCommitteeQuality and SafetyOversight SCAmbulatory CareQuality CommitteeSafetyOversight TeamDepartmentalQuality & SafetyCommitteesInterprofessional TransfusionPharmacy &DiagnosticPractice &SCTherapeutics SC Services SCWellbeing SCSTAR CommitteeRestraint CommitteePain CommitteeOffice of thePatient ExperienceAdvisory CouncilChildren’s HospitalQuality & SafetyCommitteeSurgicalQuality & SafetyCommitteePerformance Improvement TeamsFalls CommitteeNICHE CommitteeSafe Patient HandlingCommitteeReporting of qualityand safety issues only11
Quality & Safety Oversight Subcommittee Charge Coordinate the quality and performance improvement activitiesof the subcommittees of the University Hospital AdvisoryCommittee and the quality and performance improvementcommittees of the Clinical Services and hospital departments. Review, analyze and evaluate on a continuing basis theperformance of the Clinical Service quality and performanceimprovement committees in formulating standards of care;measuring outcomes of care; and taking constructiveintradepartmental action on the evaluation results, as specifiedin the UIHC Performance Improvement Program. Submit recommendations to the University Hospital AdvisoryCommittee on the establishment of and adherence to standardsof care for the purpose of improving the quality of patient caredelivered in the hospital.12
Quality & Safety Oversight SubcommitteeMembershipQuality ExecutiveCommitteeDepartment/Unit/Institutional Representatives Chief Medical Officer Chief Nursing Officer Chief Quality Officer Assoc. Chief Quality Officers Director, CQSPI Chief Medical InformationOfficer Hospital Epidemiologist Director, Nursing Research& Evidence Based Practice Director, GME Quality andPatient Safety Initiatives Chief Pharmacy Officer Director, Office of the PatientExperience Director, Operations Excellence Assistant Vice President forCompliance/Accreditation Associate VP for Legal Affairs Housestaff (4) Director, Advanced PracticeProviders Co-Chief Operating Officers Associate Chief Medical Officer,Critical Care Executive Director, University ofIowa Physicians Chief of Medical Staff Director, Perioperative NursingServicesPhysician Value Officers Anesthesiology Emergency Medicine Family Medicine Internal Medicine Internal Medicine (Hospitalists) Neurology and Neurosurgery Ambulatory Care Obstetrics-Gynecology Orthopedics and Rehabilitation Pathology Pediatrics Psychiatry Radiology, Radiation Oncology Surgery, Cardiothoracic Surgery Dermatology, Otolaryngology,Urology, Ophthalmology,Dentistry13
Physician Value Officers Oversees and/or executes work on improving key areas, including but notlimited to:– Quality metrics (e.g., CMS, TJC, UHC, institutional)– Patient safety– Patient experience (e.g., HCAHPS, CG-CAHPS, Press Ganey scores)– Department clinical re-design initiatives that foster the consistent delivery ofhigh-value care– Documentation improvement– Provider support (e.g., Epic optimization)– Strategic planning (e.g., providing input for space and facilities planning) Works with ACQO, Medical Directors, Nurse Managers, training programdirectors, and administrative leadership within his/her domain to supportinitiatives and foster and improve collaboration Formally presents and distributes key information with departmentleadership, faculty, advanced practice providers, and trainee, as applicable14
InfectionPrevention15
Types of Isolation PrecautionsStandard PrecautionsApplies to all PatientsTransmission-Based PrecautionsFor patients with documented or suspected infections3 types: airborne, droplet, contact16
MicroGuide Free App for Smart Devices(Apple/Android/Windows)17
Key Prevention Strategies for HAIsUTICLABSIVAP Place foley catheteronly when necessary Hat, mask, sterile gownfor the operator(s) Keep head of bedelevated Remove foley catheterASAP Large sterile drape onthe bed Use chlorhexidine toprep the insertion site Use central linechecklist for insertion Remove IV lines ASAPHand hygiene18
1919
20
Preventing infection:Get your flu shot!2121
Preventing infection:If you’re sick stay home!22
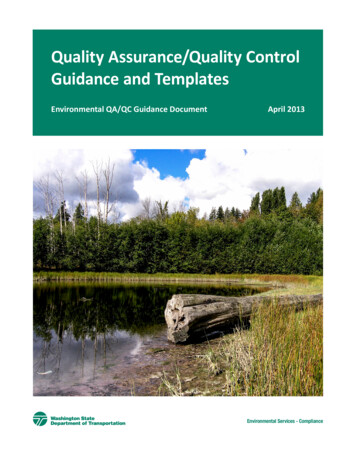
PresenteeismAn example from UIHCAttending MDSpouseMedical studentIndex case:Residentwho came towork ill withinfluenzaStaff RNChildStaff RNChildStaff RNPartnerStaff RN23
Sharps Injury orBlood/Body Fluid Exposure Sharps injury: clean wound with soap and waterimmediately Splashes:– flush mucous membranes with clean water– for eye exposure: remove contacts, if present and flusheyes for a minimum of 5 minutes. Do not delay evaluation:– During business hours, report to Employee Health– After hours, report to the Emergency Department24
25
Patient Safety Program26
HorizontalInterventionsSepsis bundleBest practice alertsDischarge planningCentral line bundleDVT prophylaxisVertical InterventionsSafety CultureBehavior Expectations for Error PreventionService Excellence27
Behavior Expectations for Error PreventionExpectationToolsPay attention to detail STAR (Stop, Think, Act, Review) Performing multiple tasks Distracted or fatigued Under time pressure Before any safety critical actionCommunicate clearly Have a questioning attitude Validate & verifyHandoff effectively Patient, Plan, Purpose, Problems, Precautions3-way repeat back / read backAsk and encourage clarifying questionsPhonetic & numeric clarificationsSBAR (situation, background, assessment,recommendation) Direct physician to physician communication28
Stop the Line Policy:Escalating ConcernConcernedindividualunable toresolve safetyor qualityissueLocal leader: Nurse managerMedical DirectorCharge NurseAttendingphysicianHouse leader: Nursesupervisor Dept ChairCNO/CMOor designee29
Safety EventsSerious Safety Event Reaches the patient Results in moderate to severe harm or deathSeriousPrecursor Safety Event Reaches the patientResults in minimal harm or nodetectable harmPrecursorNear Miss Safety Event Does not reach the patientError is caught by a detectionbarrier or by chanceNear missHPI. https://tipqc.org/wp-content/uploads/Johnson Keynote Presentation.pdf30
How to enter a Patient Safety Net Report Click on PSN icon on clinical desktopOR Access through The Point31
Tim Rossi Amy Eischens Lori Foxen Peggy Warren Kim Hermie Patient Safety Safety Specialists: . (FMEA) and Root Cause Analysis (RCA) Safety education Optimize antimicrobial usage through: . Ophtha