Transcription
Postnatal care planning
Postnatal care planningThe message we are getting fromour members is clear. We must dosomething to address the state ofpostnatal care. That’s what ourcampaign Pressure Points is allabout. Presenting the evidence andmaking a case for better provisionof postnatal care – enablingmidwives, maternity support workersand student midwives to givewomen and their families the carethat they deserve.This report continues our study byfocusing on postnatal care planningand demonstrating how the situationcould be improved through thefunding of more midwives. One thingis certain – our members cannotcontinue to paper over the cracks inan underfunded and under-resourcedpostnatal environment, withoutthere being detrimental effects onthe health of women, children andthe over-stretched maternity teamswho are crying out to be given thetools to support them.Pressure Point 4Postnatal care planningThe backgroundThe impact that good postnatal care could have on women’sexperiences and their long-term health in the context of theincreasing complexity of the health of women who becomepregnant, more intervention in labour, the high rate of caesareansections and widespread morbidity should not be underestimated.Surveys of women’s views of maternity carerepeatedly inform us of their unhappiness with thecurrent provision of postnatal care which is not ableto provide them with the support they need.Despite policy rhetoric that supports women’schoice and their involvement in decision making,the findings in this report evidence the fact thatthe NICE recommendation for individualised careplanning that could improve continuity of care andensure women and their babies receive the numberof postnatal contacts appropriate to their needs, isnot being implemented.The role of the maternity team in supportingwomen and recognising the onset of complicationsis vital. However, there has been a decrease inthe length of postnatal stay in hospital and thenumber of home visits and there appears to be littlerecognition of the value of continuity of care.This has led to a situation where the currentcontent and timing of postnatal care is not meetingwomen’s health needs.Chief Executive,Royal College of Midwives23
Postnatal care planningWhat should women be receiving?Individualised care is key to providingimportant information at the appropriate time,recognising when additional support is neededand offering targeted interventions through theappropriate multiple agency care pathways.We know that women are asking for postnatalcare that is able to be supportive and listeningand where possible in their own home. Theseaspirations are reflected in the NICE qualitystandard on postnatal care.What NICE guidance saysPostnatal care should be a continuation ofthe care the woman received during herpregnancy, labour and birth and involveplanning and regularly reviewing the contentand timing of care, for individual women andtheir babies. Each postnatal contact should beprovided in accordance with the principles ofindividualised care.The NICE quality standard recommends that:A documented, individualised postnatal careplan should be developed with the womanideally in the antenatal period or as soon aspossible after birth. This should include:4 relevant factors from the antenatal,intrapartum and immediate postnatal period details of the healthcare professionalsinvolved in her care and that of her baby,including roles and contact details plans for the postnatal period including: details about adjustment tomotherhood, emotional wellbeing andfamily support structures plans for feeding, including specificadvice about either breastfeedingsupport or formula feeding.The survey resultsBetween September and November 2013 the RCM surveyed ourmidwife, maternity support workers and student midwife membersacross the UK. We then asked the mothers at www.netmums.com fortheir experiences within the postnatal care period. These are the results.MidwivesMSWsStudent MidwivesMothersThe plan should be reviewed at each postnatalcontact. Planning and regularly reviewing thecontent and timing of care for individual womenand their babies, and communicating this(to the woman, her family and other relevantpostnatal care team members) through adocumented care plan can improve continuityof care. Women and their babies should receivethe number of postnatal contacts appropriate totheir care needs.5
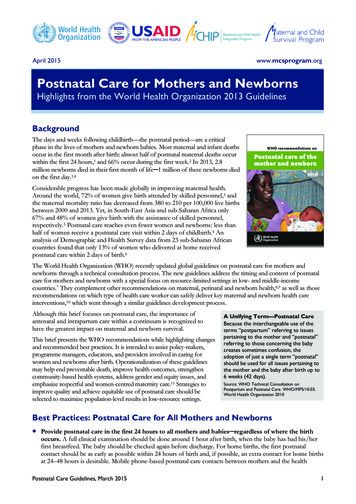
Postnatal care planningInfluencing factorsOverwhelmingly, two-thirds of midwives said themost important factor influencing the numberof postnatal visits a woman receives was not thewoman’s needs, but was the pressure on the servicefrom, for example, the midwife shortage.We asked midwives- What is the mostsignificant factorinfluencing the decisionabout the number ofpostnatal visits awoman receives?23%65%9%3%6That only one midwife in four told us that it waswomen’s needs which determined the number ofvisits received, is deeply worrying.Postnatal care should always be based onwomen’s needs and not on how underfunded andoverstretched local maternity services are.Midwives’ ability to plan care with womenwill reflect the directives from managers andcommissioners. It is clear that our members feel it isthis which is seen to be prescribing and limiting thenumber of visits.Women’s needsOrganisational pressuresCommissioners’ directivesTraditional service provisionRecommendationPostnatal services must be commissioned andprovided in a way that is consistent with NICE qualitystandard recommendations It is unacceptablethat women are not currently provided with anindividualised postnatal care plan and equallyunacceptable that there are not enough midwives toensure women receive the number of postnatal visitsthat are appropriate to their needs.7
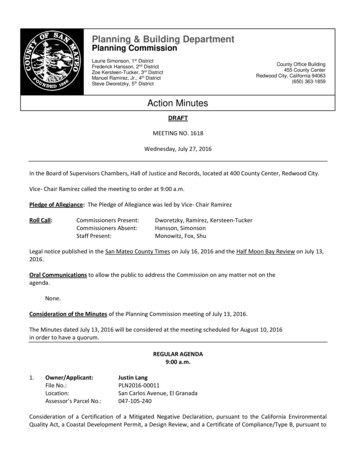
Postnatal care planningOpportunities for developing andreviewing the care plan.We askedmothers - Didthe midwife tell youbefore you had thebaby what sort of careyou would receiveafter birth?8Weasked mothers- Did you discussyour postnatal planwith a member of thematernity teamafter the birth?NoNearly half of women did not remember discussinga postnatal care plan before the birth. Although anexplanation for this may be that most women areunlikely to receive postnatal care from the midwifethey met while they were pregnant, it is worrying thatmothers are not made aware of the level of service andsupport that they can expect in the postnatal period.10%Yes she told me exactly when and how often she would visit37%Yes but only in general terms44%No she didn’t tell me9%I don’t remember if we discussed this or not64%21%15%YesDon’t rememberIt is perhaps even more worrying that nearly twothirds of mothers had not discussed the postnatalcare plan after the birth either.If these conversations between women andmidwives are not happening because resourcesare stretched, it is no wonder that both are leftdisappointed with the postnatal care being offered.9
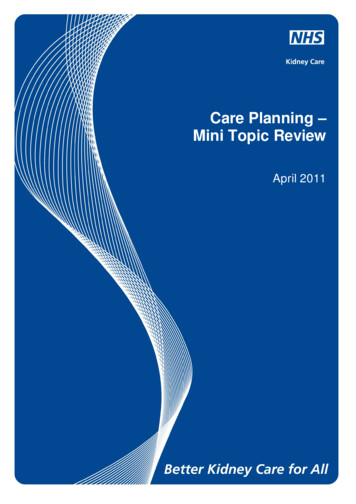
Postnatal care planningWe asked midwivesand MSWs - Can youidentify in which of thefollowing subjects you thinkthere is usually enough timeand resources to supportand inform women?10Home safety (eg room temperature, smoking)59%60%Hand hygiene and general cleanliness51%45%Changing the nappy50%64%Cord care68%74%Bathing the baby – demonstration20%46%Breastfeeding – latching71%76%Breastfeeding – position70%71%Artificial feeding – sterilisation of equipment33%45%Artificial feeding – preparation of feeds34%46%Safer infant sleeping74%62%Normal infant behavior35%39%Maternal physical wellbeing67%55%Maternal emotional wellbeing41%40%Contraception44%33%Reviewing the postnatal care plan35%35%Our members have consistently reported thatthere is seldom enough time to convey all theinformation they would like to about postnatalcare. It is particularly concerning that only 35% ofmidwives and MSWs say they have enough timeto review the postnatal care plan. This makes itclear that individualised care is not the case for themajority of women. The care being offered cannotbe responsive to women’s needs when there is notenough time to discuss it with them.11
Postnatal care planningmother - “I had a specialist ‘gateway’ midwife who gave meamazing care in the community. I dread to think how I wouldhave done without the amazing service and care I received.”Number of visitsWe asked midwivesand MSWs - What isthe average numberof postnatal visits awoman receives?MidwivesMaternity Support 8%OneTwoThe number of postnatal contacts has decreasedsignificantly during recent years, with littleevaluation of the impact. Despite nationalpolicy describing the need for effective careto meet the needs of women and their babiesup to 6 to 8 weeks after birth and if need bebeyond, postnatal services are currently beingdramatically cut. Serious attention needs to be128%7.2%ThreeFourWe asked mothers - Howmany postnatal visitsdid you receive once youwere at home?None3.4%One14.4%Two25.6%Three25.0%More than three31.6%It is disappointing but not surprising in the currentcontext that 14% of women only received one visitand a small minority received no visit whatsoever.Individualised care plans centred on a continuity ofcare model, would help ensure that women receivethe care and support they need in the postnatalperiod and reduce the risk of the needs of womenfalling between overstretched midwives.mother - “Once I gothome I saw a midwife forno more than 10 minuteson two occasions – bothwithin 8 days of givingbirth. I never, before orafter birth, saw the samemidwife twice, so I oftenhad to explain everythingover and over whichtook up all the time inmy appointments ratherthan them being a timefor discussing my care.”Despite strong policy rhetoric advocating women’schoice and involvement in decision making inmaternity care, the findings here confirm thatmidwives and maternity support workers do nothave enough time to appropriately review thepostnatal care plan and offer the women in theircare involvement in the decision making.Fivegiven as to whether the three visits, which themajority of midwives and MSWs thought to bethe average number undertaken, is an acceptableaverage, and whether it is capable of offeringsafe care, in the context of early discharge fromhospital and increasing readmission rates ofmother and babies, increasing infection ratesand postnatal morbidity.RecommendationProviders of NHS maternity care need to ensure thatmidwives and MSWs are given time to prioritise apostnatal care plan with women. This would be aidedby offering models of care that provide continuity.The RCM recognises that continuity of care is a verysignificant factor in determining the satisfactionwomen feel when reviewing their postnatal care. Weask that NHS commissioners now listen to women,midwives and maternity support workers and help usimplement a truly effective model of care.13
Postnatal care planningWhere postnatal care takes placeWe asked mothers Do you feel you hadenough time in hospitalafter giving birth?9%No - I felt rushed out before I was ready31%I was keen to get home but also feltunsupported and not quite ready to leave29%Yes - they made me feel I washappy to stay until I was ready31%I had to stay longer than I would haveliked because me (or my baby) were unwellAlarmingly only 29% of women felt able tostay as long as they felt they needed. Even moredisturbingly, 9% felt that they were rushed outbefore they were ready. The length of stay hassteadily decreased over the last fifteen yearswith the majority of women now leaving hospitalwithin six hours of the birth. This reduction inpostnatal length of stay is in the context of14mother - “I had great care with my firstbaby, with the 2nd I was rushed homewithin couple hours of giving birth,distressed and in pain, probably still inshock, which contributed to my PND.”increased instrumental and caesarean deliverieswhich requires more intensive postnatal care.NICE recommends that: “Length of stay in amaternity unit should be discussed betweenthe individual woman and her healthcareprofessional, taking into account the health andwell-being of the woman and her baby and thelevel of support available following discharge”.mother - “Definitely feelthat staff are under hugestress and the quality ofcare is affected. After Ihad my first baby I feltawful and wanted to stayovernight but was told nothat it was not a hotel!”midwife - “The women aredischarged inadequately preparedfrom the ward because thehospital is grossly understaffed.”midwife - “The managementtold me that I had to dischargethis woman who was strugglingwith breast feeding as weneeded the bed. There is littlesupport for the women due toour early discharge policy.”15
Postnatal care planningmother - “A midwife never came tome; I had to go to the maternity unit.”We asked midwivesand MSWs - Where ispostnatal care providedin your area?Midwivesmidwife - “Since re-structuring delivery of care continuity hasdisintegrated. Lack of staff and money has led to a fragmented service.”We askedmothers - Wheredid your postnatalcare take place?MSWs100%95%80%84%66%60%88%At home7%At the hospital2%At the GP surgery3%At a postnatal %15%11%0%HomeStand alone Alongsidemidwifery midwiferyled unitled unitmother - “I had togo all over for it evenhaving a new baby,a C-section scar andbeing a single clinicChildren'scentreOn thephonemother - “I think parents should have a fewvisits at home; I had to travel on a bus withmy baby to a clinic that isn’t even near myhouse. Nobody came to my house eithera day or a few days after to help withbreastfeeding I had to ask a neighbour. Ifelt pretty let down after the birth of mydaughter, luckily I had my mum.”These findings demonstrate that a considerablenumber of women still receive at least some oftheir postnatal care at home. Good postnatal careplanning should enable women to take part in thedecision about where it takes p
documented care plan can improve continuity of care. Women and their babies should receive the number of postnatal contacts appropriate to their care needs. Individualised care is key to providing important information at the appropriate time, recognising when additional support is needed and offering targeted interventions through the