Transcription
Protocol for Postmortem Diagnosis of Rabies in Animals by DirectFluorescent Antibody TestingA Minimum Standard for Rabies Diagnosis in the United StatesI. IntroductionAmong the findings of the National Working Groupon Rabies Prevention and Control was the needfor a minimum national standard for thelaboratory diagnosis of rabies (Hanlon et al.,JAVMA, 215:1444-1446, 1999). In response tothis recommendation, a committee was formedfrom representatives of national and state publichealth laboratories (Appendix 1) to evaluateprocedures employed by rabies diagnosticlaboratories in the United States. Both theNational Working Group and this committee haveas their goal the improvement of the overallquality of rabies testing through the formulationof guidelines and standards for equipment,reagents, training, laboratory protocols, qualityassurance, and laboratory policy for rabiesdiagnosis.As a first step to attaining this outcome, thecommittee prepared a standardized protocol forthe analytical phase of rabies testing using thedirect fluorescent antibody (DFA) test andevaluated the protocol by comparison testing of435 samples submitted to public healthlaboratories for rabies diagnosis (Appendix 2) .Later documents will address other elements thatcan affect the quality of laboratory testing such asthe pre-analytical steps (rationale for specimensubmission), the post-analytical phase (resultreporting and confirmatory testing), laboratorypolicy, and quality assurance.The standardized protocol was developed frompublished procedures and the collective laboratoryexperience of the committee members. The grouprecognizes that a range of possible methods mayachieve the desired outcome for some of the lesscritical steps in the diagnosis of rabies and thatlaboratory policy may be regionally defined insome cases; however, the goal of the group wasto establish a single protocol by which all othermethods could be validated by comparison. Therecommendations included in this documentshould be closely followed to ensure a test ofhighest sensitivity and specificity. Modifications orshort cuts in procedures often lead to falsepositive and false negative results and non specific or uninterpretable reactions. A laboratorywishing to incorporate elements of test methodsother than those presented in this documentshould validate and confirm those methods byconsultation with one of the laboratories listed inAppendix 1.The standard protocol for DFA will be madeavailable to each rabies testing laboratory bypostal or electronic mail and by participation in atraining workshop. In addition, the protocol andother documents will be placed on the web sitesmaintained by the Centers for Disease Control andPrevention (CDC) at www.cdc.gov/rabies and theAssociation of Public Health Laboratories (APHL)at www.aphl.org. A listserve is planned so that aninteractive dialogue may be established toaddress questions and disseminate informationabout rabies testing.In addition to the procedural aspects detailed inthis document, each testing laboratory mustmaintain the competency of its employees. Thereis no substitute forconstant practice and experience in performingDFA testing. All new employees should be trainedin all aspects of the procedure, and competencyshould be evaluated by the senior technologist ona routine basis. Competency can be assessed byobservation of all procedural aspects on a routinebasis, as well as performance on proficiency testsamples, and testing on internal blind samples. Alltraining should be documented throughout thetraining period, and observations of breakdown intechnique or procedures should be noted andcorrected before the lead technologist can beassured that the trainee can perform theprocedure in a competent and reliable manner. Alllaboratories performing this DFA test for rabiesshould participate in national rabies virusproficiency testing, available through theWisconsin State Laboratory of Hygiene.Enrollment information may be obtained throughtheir web site (www.slh.wisc.edu/pt) or by calling1-800–462–5261.At least once every 6 years, each laboratoryshould send a representative to the NationalLaboratory Training Network sponsored course"Laboratory Methods for Detecting Rabies Virus".The course, held at least every 2 years, details allaspects of rabies testing and provides anopportunity for diagnosticians to meet colleaguesfrom other states and discuss common problemsand their solutions. Advances in rabies diagnosisand research are presented at the Rabies in theAmericas meeting, held every year at locations inNorth and South America.Bench training and consultation on basic aspectsof rabies diagnosis are available at the state
public health laboratories in New York, California,Texas, Wisconsin, and Ohio and at the nationalrabies laboratory at CDC (Appendix 1). Theselaboratories can be contacted at any time withquestions or requests for consultation andtraining. Laboratories that annually process 100samples may have particular difficulty maintainingrabies diagnostic proficiency and may want towork closely with larger laboratories whereadditional resources are available. Sources offunding are being investigated for those statesthat have no travel budget to attend meetings,workshops, or seminars. Potential sources thatare being explored include ASM, APHL, or theEpidemiology and Laboratory Capacity (ELC)program at CDC.II. Safety All persons involved in rabies testingshould receive pre-exposure immunization withregular serologic tests and booster immunizationsas necessary (CDC, MMWR, 48: 1-22, 1999).Unimmunized individuals should not enterlaboratories where rabies work is conducted. Alltissues processed in an infectious diseaselaboratory must be disposed of as medical wasteand all activities related to the handling of animalsand samples for rabies diagnosis should beperformed using appropriate biosafety practices toavoid direct contact with potentially infectedtissues or fluids (CDC and National Institutes ofHealth, Biosafety in Microbiological andBiomedical Laboratories, 4th edition, U.S.Government Printing Office, 1999). Personnelworking in rabies laboratories are at risk of rabiesinfection through accidental injection orcontamination of mucous membranes with rabiesvirus contaminated material and by exposure toaerosols of rabies infected material. Allmanipulations of tissues and slides should beconducted in a manner that does not aerosolizeliquids or produce airborne particles. Barrierprotection is required for safe removal of braintissue from animals submitted for rabies testing.At a minimum, barrier protection during necropsyshould include the following as Personal ProtectiveEquipment (PPE): heavy rubber gloves, laboratorygown and waterproof apron, boots, surgicalmasks, protective sleeves, and a face shield.Fume hoods or biosafety hoods are not required,but they provide additional protection from odor,ectoparasites, and bone fragments. Glass chipsand shards from slide manipulations are alsopotential sources of exposure to rabies. Careshould be taken to protect eyes and hands duringmanipulation and staining of slides and duringclean up of the microscope and surrounding area.A microscope adaptor is available to provide eyeprotection from any glass slivers produced whenslides are moved across the microscope stage.Ergonomic equipment (fatigue mat, microscopecontrols) should be used to prevent fatiguerelated injuries to employees during lengthynecropsy and slide-reading procedures.III. Equipment and Reagents(Use of trade names and commercial sources isfor identification only and does not implyendorsement.)A. Equipment1. Necropsy instruments should be of sufficientquantity for 1 set per sample to prevent crosstransfer of infected tissue between samples.2. Autoclave and/or instrument sterilizer. Allinstruments should be cleaned and sterilizedbefore reuse.3. Specimen storage containers must be largeenough that reserved portions of brain stem andcerebellum (and hippocampus, if tested) remainas recognizably separate pieces. Because of therisk of breakage, glass vials and tubes areunacceptable for specimen storage. Wide mouth,screw cap, polypropylene jars or sample bottlesare used in many laboratories (e.g., Nalgene 2118or 2189).4. Refrigerated storage. An explosion proof 20 C freezer is required for fixation ofimpression / smear slides and storage of acetoneand other reagents; long term sample storagerequires a freezer at -70 C. Frost-free freezersshould not be used. Heat cycles in frost-freefreezers will denature proteins in reagents andspecimens and may compromise test results.5. Microscope slides should be of highestquality with coverslip matched to the lens workingdistance. Teflon or pre-ringed well slides can beused to denote stained areas for touch impressionslides. User-specified templated slides can beordered through Cel-Line/ERIE Scientific Co. (1 800-258-0834). Wells of 14 mm or 15 mmdiameter are adequate for rabies tests. Markinginstruments that contact tissue (e.g., wax pencilor Martex pen) should not be used to denotestained regions of the slides, because this processcan transfer infected tissue between slides. Slipsmears cannot be made on pre-ringed slides. A 16mm area to be stained on a slip smear can bemarked by dipping the rim of a 16 x 100 mm testtube into a small pool of nail polish poured onto asquare of aluminum foil. A well is made on theslip smear by lightly touching the test tube rim tothe surface of the smear. To avoid crosscontamination between specimens, a separatetest tube and pool of nail polish is used for eachspecimen submitted for testing. Best contrast isobtained with red pigmented nail polish.Alternatively, separate slides can be made for
staining with each reagent. The addition of acounter stain such as Evans Blue to the conjugatewill also denote stained areas.6. Acetone fixation and post-stain rinsecontainers should be in sufficient quantity suchthat slides made from each test animal areprocessed in a container separate from the slidesfrom other animals. Positive control slides areprocessed in a container separate from test clides.A false-positive test may result from crosstransfer of tissue between slides from differentanimals if a common container is used for fixationor washing.7. Syringe filters (0.45um). Anti-rabiesconjugates should be filtered to removedissociated fluorescein isothiocyanate (FITC) andprotein aggregates that may bind non-specificallyto tissue. Conjugates should be filtered only onceand should be evaluated for the effect of filtrationon the titer of the working dilution (see sectionVI). Syringe filters allow the conjugates to befiltered as they are added to test slides. Similarly,syringe filters will remove contaminants andprecipitates as mountants are added to slides.Filters for the conjugate must be low proteinbinding (e.g., cellulose acetate) to prevent loss oflabeled antibody from the conjugate. Filtermaterials that bind proteins with great avidity(e.g., mixed cellulose esters) should not be usedfor conjugate filtration. Both large volume, midvolume, and small volume filters are available(Schleicher & Schuell, Uniflo; Millipore, Millex-HV).Smaller volume filters avoid dead volume loss tothe filter membrane. Evans Blue counterstain alsobinds to the membrane, but the filter is saturatedquickly. To avoid slide to slide difference incounter stain, laboratories that employ Evans Bluecounterstain in the conjugate should discard thefirst three drops of conjugate expressed thoughthe filter.8. Incubator (37 C) and humidified stainingtray or chamber. Constant humidity must bemaintained during the staining process. Conjugatedried on the slides during the staining processmay be mistaken for specific staining, resulting ina false positive test, or may obscure specificstaining, resulting in a false negative test.9. Fluorescence microscope. The quality of thefluorescence microscope is critical to thesensitivity of the DFA test. Manufacturers offermany equipment options. Appendix 3 contains adiscussion of oculars, objective lens, filter sets,and light sources and their effects on instrumentperformance. At a minimum, all rabies diagnosticlaboratories should have a reflected light (incidentlight) fluorescence microscope with high qualityobjective lenses. Both magnification and andnumerical aperture (NA) must be considered inlens selection. Although image size increases withmagnification, both resolution and imagebrightness are related to the NA of the objectivelens, and brightness decreases with magnification.For example, a high quality 20X dry objective witha NA of 0.75 provides a brighter image over alarger field of view with no loss of resolution ascompared to a dry 40X objective with an NA of0.75. (See the discussion of magnification, imagebrightness and resolution in Appendix 3.) The useof immersion oil increases image brightness bypreventing the loss of emitted light in the airspacebetween coverslip and dry objective. Although notevery slide must be observed with a 40X oilobjective of high NA, resolution of very fine dustlike inclusions and recognition of some types ofnon-specific staining is aided by examination withthis type of lens. An oil immersion lens requires ahigh quality immersion oil. An oil should bechosen that produces the least autofluorescenceand thus the best contrast between FITC andtissue (e.g.,Cargille type DF). The oil should havethe same refractive index as glass (1.515).B. Reagents1. Acetone. Only American Chemical Society(ACS) Reagent Grade acetone should beemployed and the acetone should not be reused.2. FITC-conjugated anti-rabies antibodies.Reagents presently available commercially arelisted in Appendix 4. Every laboratory shouldmaintain stocks of anti-rabies conjugates fromtwo different sources. The two sources should betwo different monoclonal antibody pools or onemonoclonal antibody conjugate and onehyperimmune serum conjugate. (Note: CentocorFITC-Anti-rabies Monoclonal Globulin and LightDiagnostics Rabies DFA II contain the sameantibody pools and are not considered differentsources.) Antigen presentation and antibodyavidity and affinity vary with different rabies virussamples, and viral inclusions may appear quitedifferent when stained with different reagents.Although hyperimmune serum reagents containmany different anti-rabies antibodies that can thatproduce a wide-spectrum of rabies virusrecognition, these reagents also containextraneous antibodies that can produce severaltypes of non-specific reactions (Appendix 5).Extraneous antibodies are not a problem withmonoclonal antibody reagents but the finespecificity of these reagents may result in non recognition of some variants of rabies virus. Theuse of two reagents prepared from different poolsof monoclonal antibodies greatly reduces the riskof non-recognition of any one variant.FITC-labeled conjugates should not be used past
the manufacturer's expiration date. Upon receipt,a conjugate should be reconstituted (iflyophilized) and titrated to determine a workingdilution (section VI). Stock solutions of conjugateare stored as frozen aliquots in a non-frost-freefreezer at -20 C or below ( -30 C is preferred).Conjugate diluted to the working dilution is storedat 4 C and discarded after 7 days. The workingdilution of the conjugate is filtered as it is addedto the test slide. Excess diluted conjugate can bestored at 4 C in the syringe and attachedsyringe-filter unit used for dispensing it, if care istaken to remove any remaining droplets from thefilter outlet and the outlet is sealed against dryingwith a syringe tip or plastic wrap.3. Specificity controls. Appendix 4 listscommercially available control reagents. Thespecificity control for an FITC-labeledhyperimmune serum rabies reagent is an FITClabeled serum reagent produced in the sameanimal host as the rabies reagent (typically goator horse), but either as normal serum orhyperimmune serum directed to an agent otherthan rabies virus (e.g., FITC-labeled antidistemper reagents). The control reagent shouldbe diluted to the same mg protein concentrationas the rabies reagent. Similarly, the specificitycontrol for a rabies reagent prepared from amouse monoclonal antibody is an FITC-labeledmouse monoclonal antibody of the same isotypeand protein concentration as the rabies reagentbut directed to an agent other than rabies virus.Suspensions of Normal Mouse Brain (NMB) andRabid Mouse Brain (RMB) are no longer used asspecificity controls. Historically, RMB and NMBwere used as diluents for FITC-labeledhyperimmune serum conjugates to control for thepresence in the conjugate of extraneousantibodies present in animals used for theproduction of rabies hyperimmune serum as aresult of a natural exposure. False positivereactions were identified when staining wasobserved both with a conjugate adsorbed withNMB (which should have no effect on anyantibody in the conjugate) and a conjugateadsorbed with RMB (which should remove onlythe rabies antibodies and have no effect onantibodies to other infectious agents). Becausemonoclonal antibody reagents contain onlyantibodies reactive with antigens on rabies virus,it is not possible for these reagents to containextraneous antibodies and adsorption controls forthese reagents are meaningless. A more lengthyexplanation of control reagent use is found inSection VII and in Appendix 5.4. Conjugate diluent should be 0.01Mphosphate buffered isotonic saline solution at pH7.4 to 7.6 (e.g., phosphate buffered saline (PBS)Sigma P3813 is 0.01 M phosphate buffer, pH 7.4,with 0.138 M NaCl and 0.0027 M KCl). No proteinstabilizer (e.g., bovine serum albumin) is neededin the diluent.5. Counterstains added to the working dilutionof the conjugate provide contrast and lowerbackground and also serve as a marker foraccidental omission of the diagnostic reagent.Counterstain use is optional. Evans Bluecounterstain (0.5% in PBS, Sigma, Product #E 0133, for use in immunofluorescent assays) canbe aliquoted and stored at 4 C for up to 6months and indefinitely at -20 C. The amount ofcounterstain added to a conjugate is determinedby titration when the working dilution of theconjugate is determined (section VI). Due tocounterstain, the tissue will be noticeably red, butshould not be so strongly red as to diminish thespecific green fluorescence of rabies virusproteins. An Evans Blue concentration of0.00125% works in many laboratories. Thisconcentration is prepared by adding 2.5microliters of 0.5% stock dye solution per ml ofconjugate diluent.6. Rinse / soak buffer. A PBS formula of thesame pH and molarity as the conjugate diluent isused as the rinse/soak buffer (e.g., Sigma P3813is 0.01 M phosphate buffer, pH 7.4, with 0.138 MNaCl and 0.0027 M KCl). Carboys or other largecontainers used for storage and dispensing ofrinse buffers should be disinfected by autoclavingon a regular schedule.7. Mountant ( 0.05 M Tris-buffered saline pH9.0 with 20% glycerol). Prepare 0.05 M Tris /0.15 M NaCl solution by dissolving 0.623 grams ofTrizma pre-set crystals and 0.85 g NaCl in a totalvolume of 100 ml distilled water. Filter (0.45 um)and store at room temperature. Remake at leastonce per year; check pH quarterly. Prepare a onemonth supply of mountant by mixing 4 parts Tris saline pH 9.0 with 1 part glycerol. Store at roomtemperature. Glycerol concentrations above 20%affect the antigen binding capacity of someantibodies and should not be used. Glycerolshould be replaced at yearly intervals because thepH changes slowly with time. The mountantshould be remade or the pH tested once a month.The mountant is added to the coverslip bydispensing with a syringe fitted with a 0.45 umsyringe filter. (Trizma pre-set crystals, Sigmacatalog # T6003 ; ACS Reagent Grade glycerol,Sigma catalog #G7893)8. Immersion oil should be formulatedspecifically for fluorescence applications (e.g.,Cargille DF). Immersion oils formulated forgeneral microscopy may produce significant autofluorescence.
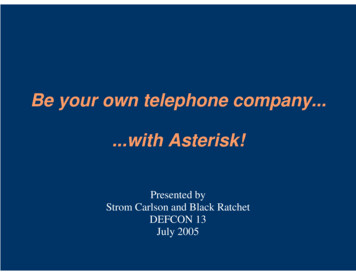
IV. Sample Collection and HandlingA. Rationale for sample collection. When ananimal develops rabies (most often when the biteof another animal transfers rabies-virus-ladensaliva to the wound), rabies virus movestransneuronally from the site of entry to thespinal cord and brain. Patterns of virus spreadwithin the central nervous system suggest that athorough examination of the brain stem is criticalto rabies diagnosis. Viral antigen is widespread inthe brain of most animals positive for rabies, butbecause spread may also be unilateral, especiallyin larger animals (Figure 1), a negative finding forrabies can be made only if a complete crosssection of the brain stem is examined.Examination may be made at the level of thepons, medulla, or midbrain.Figure 1. DFA test of a transverse section (cross-section) ofbrain stem from a rabies infected donkey showing unilateral virus spread (200X magnification, frozen section).Cerebellar tissue should also be included in arabies test. Although brain stem is the tissue mostreliably found to contain viral antigen, thecharacteristic size and shape of intracytoplasmicinclusions produced as rabies virus accumulates inthe large neurons of foliar regions of thecerebellum are easily detected and recognized byDFA. Inclusion of this tissue yields a moreconfident diagnosis than examination of brainstem alone. Although the hippocampus was oncethe tissue of choice for histologic tests for Negribodies, hippocampus is of limited additional valuewhen brain stem and cerebellum are examined. Ifthe cerebellum is missing from tissue submittedfor rabies testing, however, a negative findingmay be made from examination of brain stem andhippocampus. While a negative finding for rabiescan be made only if brain stem tissue is amongthe tissues examined, incomplete specimensshould be tested, if possible. Specific staining inany tissue reacted with anti-rabies antibody isdiagnostic of rabies infection.Virus is present in the saliva of an infected animalonly after virus proliferation in the central nervoussystem and subsequent centrifugal spread fromthe brain to the salivary glands. A negative DFAtest for the presence of rabies virus in brain tissueassures that contact with saliva of a biting animalcould not have transmitted rabies. Because virusmay not spread to all salivary glands and may bepresent only intermittently in saliva, negativetests of salivary glands or saliva cannot rule outrabies infection.B. Shipment of samples. Because rabiesprophylaxis is usually delayed pending alaboratory report, specimen transit time to thelaboratory should be as short as possible,preferably within 48 hours. A fresh, unfixed brainsample is critical to a rapid and accurate diagnosisof rabies. Refrigeration will preserve a sample forat least 48 hours. Freezing of the sample fortransit will not reduce the sensitivity of the test,but may introduce additional testing delays andimpede recognition and dissection of appropriatetest samples. Repeated freeze-thaw cycles mayreduce test sensitivity and should be avoided.Biocontainment during specimen transport iscritical, to prevent both contamination of theoutside of the package and cross-contaminationbetween samples within the package.C. Unacceptable deterioration ordecomposition of a sample is a qualitativeassessment of the condition of each sample uponarrival in the lab. Substantial green color,liquefaction, desiccation, or an unrecognizablegross anatomy can indicate an unsatisfactorysample. A substantial loss of tissue duringstaining and washing or the presence of bacteriaon the stained slide may also indicate sampledeterioration. If negative results are obtained ondeteriorated tissue, the test report should stateonly that the condition of the sample is such thattests cannot rule out the presence of rabies virusin the specimen. The negative findings should notbe mentioned, since this is often misinterpretedas a negative diagnosis. Positive test results arereported as such.D. Chemical fixation (e.g., formalin) can altertissue to make a sample unsuitable for testing.Methods for testing fixed tissue exist, but thesetests are performed by other than standard DFAmethods on tissues prepared by controlledfixation procedures. These methods are notavailable in all laboratories and referral toreference laboratories will delay test results.E. Laboratory handling of samples. Samplessubmitted to the laboratory may be a completecarcass, an intact head, or dissected brain tissue.
Dissected brain tissue must include a completecross section of the brain stem and eithercerebellum or hippocampus. All materialsubmitted with a sample, including the carcass,should be held frozen until the test is completedand results reported. A single additional freezethaw cycle will have no effect on rabies-specificstaining if repeat testing of the sample should berequired, and the freeze-thaw cycle may eliminateor reduce some non-specific staining. Retention ofthe carcass is necessary to verify the identity ofan animal in the case of unusual test results, andto identify a wild animal to species. Sampleidentifiers (accession numbers) should be used tolabel boxes and all items accompanying thesample. All necropsy and tissue processing mustinclude proper identification of each sample andavoidance of any practice that could lead to crosscontamination of samples. Each specimen shouldbe handled on a clean work surface with newdisposable gloves. All instruments used duringnecropsy, dissection, and slide preparation mustbe thoroughly disinfected by boiling or autoclavingfollowed by thorough washing before reuse.Instruments not in use should be kept in closedstorage. Only those instruments in use forprocessing a single sample should be exposed.Frozen reference material taken at necropsyshould be retained in the laboratory for all testsamples. Most laboratories maintain test samplesfor 2 to 6 months, but representative positivesamples should be maintained for longer periodsfor use as controls, for epidemiologic typing, andfor other purposes. Storage containers forreference material must be large enough thatreserved portions of brain stem and cerebellum(and hippocampus, if desired) remain asrecognizably separate pieces and allow completecross sections to be made if repeat testing isrequired. A video describing necropsy proceduresis available from the CDC.V. Preparation of Impression Slides /SmearsA. Sampling. While a positive finding of rabiesvirus antigen in any tissue is diagnostic of rabiesinfection, a negative finding for rabies can bemade only if the diagnostic test includesexamination of at least two areas of the brain:brain stem and preferably cerebellum (Figures2,3,4,5,6,7,8,9,10,11,12,13). A complete crosssection of the brain stem is required. If brain stemis unavailable and other brain tissues arenegative,the sample must be consideredunsatisfactory for testing. If cerebellum isunavailable, a diagnosis may be made byexamination of brain stem and hippocampus(Figures 14 and 15). Each brain area is testedFigure 2. Dorsal view of brainHindbrainMedullaMidbrainPonsBrainstemFigure 3. Ventral view of brain showing areas of brain stemsuitable for rabies testingFigure 4. Lateral view of brain with cerebrum removed toshow the extension of brain stem beneath the cerebellum. Arabies diagnosis should include an observation of the cutsurface of a cross section of the brain stem (through the medulla, pons, or midbrain area) and the cerebellum (througheach hemisphere and the vermis). For example, a cross section of the midbrain area (dashed line) would include alltissues necessary for rabies diagnosis
Figure 5. Surface of cut section through midbrain areashowing convoluted gray matter and white foliar regions ofthe cerebellum, and the cerebellar connection to pons andmedulla.Figure 6. Dissected transverse (cross) section of brainstem.Figure 7. Two 15 mm tissue sections dissected from thecut surface of a brain stem cross section.Figure 8. Touch impression of brain stem cross section.with FITC-labeled anti-rabies reagents preparedfrom two different sources (i.e., two differentmonoclonal antibody reagents or a monoclonalantibody reagent and a hyperimmune serumreagent; see note in section III.B.2). For mostanimals a diagnostic test will include 4observations: a smear or impression made frombrain stem stained with reagent 1 and a smear orimpression made from brain stem stained withreagent 2; a smear or impression made fromcerebellum stained with reagent 1 and a smear orimpression made from cerebellum stained withreagent 2. Each sampled brain area should be of asize sufficient for examination of 40 separateviews (microscopic fields) at a magnification ofapproximately 200X. With most microscopes animpression made in a 15 mm diameter well or asmear of 10 mm2 meets this recommendation(Figures 7-8 and 12-13).1. Brain stem. The brainstem is anterior to thecerebellum and continuous with the spinal cord(Figures 2, 3 and 4). The uppermost portion ofthe brain stem is the midbrain; the hindbrainportion of the brain stem is composed of pons andmedulla oblongata. A cross (transverse) section ofone of these areas is necessary for rabies testing.Slides are prepared from the cut surface of thecross section to expose multiple ascending anddescending nerve tracts (Figures 4, 5, and 6). Formany animals (e.g., dog-sized or smalleranimals), a complete cross section will fit in a 15mm diameter well. A duplicate impression of thecross section is made for staining with the secondreagent. If the cut surface of the cross section is 15 mm, but 30 mm, two impressions are madefrom the cut surface by dissecting the tissue(Figures 6, 7, 8). One impression / area is stainedwith each reagent. If the cut surface of the crosssection is 30 mm, one impression is made fromeach of four tissue sections dissected fromdifferent areas of the lateral surface of the crosssection (two impressions / areas are stained witheach reagent.)Slip smears are also made from the cut surfac
binding (e.g., cellulose acetate) to prevent loss of labeled antibody from the conjugate. Filter materials that bind proteins with great avidity (e.g., mixed cellulose esters) should not be used for conjugate filtration. Both large volume, mid-volume, and small volume filters are available (Schleicher & Schuell, Uniflo; Millipore, Millex-HV).



![[MS-OFBA]: Office Forms Based Authentication Protocol](/img/3/ms-ofba.jpg)