Transcription
Chapter 13: Level 2Ultrasound Physics & Instrumentation5th EditionCompanion PresentationFrank MielePegasus Lectures, Inc.License AgreementThis presentation is the sole property ofPegasus Lectures, Inc.No part of this presentation may be copied or used for any purpose other thanas part of the partnership program as described in the license agreement.Materials within this presentation may not be used in any part or form outside ofthe partnership program. Failure to follow the license agreement is a violationof Federal Copyright Law.All Copyright Laws Apply.Chapter OutlineChapter 1: MathChapter 11: Quality AssuranceChapter 2: WavesChapter 12: Fluid DynamicsChapter 3: AttenuationChapter 13: HemodynamicsChapter 4: Pulsed WaveChapter 14: MSKChapter 5: TransducersChapter 6: System OperationsChapter 7: DopplerChapter 15: HIFUChapter 16: ElastographyChapter 8: ArtifactsChapter 17: IMT Ultrasound ImagingChapter 9: BioeffectsChapter 18: Strain ImagingChapter 10: Contrast and HarmonicsChapter 19: Patient Care1
Chapter 13: Level 2Removing Assumptions MadeIn Chapter 13: Fluid Dynamics, the basic equations were derivedbased on the following assumptions: The flow conduit is a rigid, cylindrical tube The flow is steady state, laminar flow The fluid is NewtonianIn this chapter, we remove these restrictions which clearly do not hold true forblood flow.The Assumption of Steady State FlowThe driving pressure for blood flow is highly pulsatile, as shownin the figure below. Since the driving pressure is dynamic, there are manychanges which affect flow relative to the simplified equations introduced in theprevious chapter.Fig. 1: (Pg. 403)The Assumption of Rigid Flow ConduitsThe arteries are elastic and not rigid conduits for flow. This elasticity isimportant since: The elasticity allows the aorta to be capacitive The capacitance of the aorta allows energy to be stored in the wallsaorta, to provide energy to propel blood during diastoleof the Run off from the capacitive aorta through the resistive arterioles andcapillaries reduces the pulsatility, improving heart efficiency.2
Chapter 13: Level 2Pressure Volume Relationship (CompliantVessel)The simplified law expresses that therate of change in pressure isproportional to the rate of change involume. As seen by this graph, thecompliance of the vessel (non-rigid flowconduit) is not linear, explaining thenaming of the equation as “simplified”.In reality, there is a non-linearrelationship between a change inpressure and the resulting change involume.(A 25% increase in pressure at 100mmHg results in a 50% increase involume.)Fig. 2: (Pg. 405)(Redrawn from Berne, R.M. and Levy,M.N., Cardiovascular Physiology)Pressure Volume Relationship (Compliantvs. Non-compliant Vessel)In this graph we see what happens toflow with an increase in pressure for anon-compliant vessel. At lowerpressures, the relationships is relativelylinear, but at higher pressures, anincrease in pressure results in virtuallyno increase in volume.(A 25% increase in pressure at 100mmHg results in only a 7% increase involume.)Fig. 3: (Pg. 405)(Redrawn from Berne, R.M. and Levy,M.N., Cardiovascular Physiology)Single Flow Conduit “Tacit” AssumptionAlthough not explicitly stated, the equations were all derived makingthe simplistic assumption of a single flow conduit. The effective resistanceof multiple flow conduits can become relatively complex based on the geometryof the multiple vessels.3
Chapter 13: Level 2Series ResistanceFor flow conduits in series (the exit of one connected to the input of the next)the effective (overall) resistance is simply the sum of resistances of eachindividual component, as shown below.Fig. 4: (Pg. 406)Parallel ResistanceFor flow conduits in parallel (the inputs connected to each other and theoutputs connected to each other) the effective (overall) resistance is morecomplicated to calculate than a series resistance. The inverse effectiveresistance is calculated as the sum of the individual inverse resistances asshown below.Fig. 5: (Pg. 406)Note the effective resistance decreases with increasing parallel vessels.Example of Series ResistanceFor this simple case as shown below, we see that the effective resistance offour shorter segments connected in series is simply four times the resistance ofone short segment. Equivalently, four shorter segments connected in serieshave the same effective resistance as one longer segment of the samediameter.Fig. 6: (Pg. 407)4
Chapter 13: Level 2Example of Parallel ResistanceNotice that by placing the same four short segments in parallel,the effective resistance now decreases by a factor of four, as shown below.Fig. 7: (Pg. 407)Comparing Parallel with Larger DiameterBe careful not to assume that theresistance would be the same fora vessel of four times the radius r,as for four vessels in parallel eachof radius r. As shown, theeffective resistance for a singlelarger diameter vessel is muchless than for the parallelcombination (in fact 64 timesless).Fig. 8: (Pg. 407)Parallel Series NetworkApplying the rules we learned for series and parallel combinations,the effective resistance for the following network is calculated as:Reff R1 R2 R34To view specificcalculation refer topage 783Fig. 9: (Pg. 408)5
Chapter 13: Level 2The Assumption of Smooth Straight VesselsThe amount of energy lost bytransporting blood over rough vesselsurfaces is obviously greater thanthe energy lost transporting oversmooth surfaces. This fact isimportant since the determination ofdisease severity does not take intoaccount changes in frictional energylosses associated with the geometryof the lesion.Fig. 10: (Pg. 409)“Discretized” Energy LossThis figure demonstrates frictional and viscous energy losses asis existing in discrete layers as a means to more simply visualize energy loss.Fig. 11: (Pg. 410)Energy Losses with Varying Stages DiseaseThis diagram demonstrates how energy losses increase with decreasing vesselsize as a result of increased frictional and viscous energy loss (using the“discretized” model of the previous slide).Fig. 12: (Pg. 410)6
Chapter 13: Level 2Velocity ProfilesThe following diagram demonstrates the boundary effects on the flow profilethrough varying vessel sizes.Fig. 13: (Pg. 410)The Cardiovascular SystemThis figure shows asimplified model of thecardiovascular system,demonstrating the keyfunctions required.Fig. 14: (Pg. 411)Arterial Vessel SizesVarying vessel diameter is aprincipal mechanism incontrolling the effectiveresistance throughout thearterial system. Control of theresistance is critical to controlpressure decrease as well asregulate volumetric flow (asindicated by the simplified law).Fig. 15: (Pg. 412)7
Chapter 13: Level 2Complex Resistance Network of the ArterialSystemEven though there are increasingnumbers of vessels progressingfrom the left heart toward theperiphery, the resistancedecreases in progression from thelow resistance of the aorta to therelatively high resistance of thearterioles. The effectiveresistance in the capillaries is stillvery high, although generallylower than the resistance of thearterioles because of the sheernumber of capillaries.Fig. 16: (Pg. 413)Relative ResistancesThe following graph (linear and logarithmic) display the resistance of the vesselsrelative to the resistance of the aorta. Note the high resistance of the arteriolesgiven rise to the terminology of the arterioles as the “resistance component” ofthe cardiovascular system.Fig. 17: (Pg. 413)Fig. 18: (Pg. 413)Velocity versus Total Cross Sectional AreaThe velocity of the flow iscontrolled primarily by the varyingtotal cross sectional area of thevessels. According to thevolumetric flow equation(continuity), for a fixed volume, asthe area increases the velocitydecreases, as seen in theassociated figure.Fig. 19: (Pg. 415)8
Chapter 13: Level 2Pressure Across the Arterial SystemImportant Characteristics:1. Slight increase in pulsepressure from aorta tosmall arteries2. Pulsatility is damped atlevel of arterioles3. Rapid pressure dropoccurs at arterioles4. Significant pressure dropoccurs across capillariesFig. 20: (Pg. 416)5. Pressures in venous sideare very low and relatively“steady-state”The Venous SystemThe pressure in the venous system (as seen in the diagrams from a few of thelast slides) is relatively low. The result is that people often underestimate therole of the venous system as a subsystem of the cardiovascular system.Specifically, the capacitance of the venous system is critical to controlling themean circulatory pressure.Note: The venous system is referred to as the “capacitive” component of thecardiovascular system.Blood Volume Distribution (patient at rest) 65 – 70% in the veins and venules 10 - 12% in the systemic arteries 5% in the heart 5% in the pulmonary veins 5% in the systemic capillaries 3% in the pulmonary capillaries 3% in the pulmonary arteriesCan you see why the venous system is referred to as the capacitive componentof the CV system?9
Chapter 13: Level 2Reference for Hydrostatic PressureBy referencing the hydrostaticpressure to the right atrium ofthe heart, the central pressureof a patient does not need tobe corrected by the hydrostaticpressure differences fordifferent height patients. Theresult of referencing the RA as0 mmHg is that the hydrostaticpressure is considerednegative in the head for astanding patient.Fig. 21: (Pg. 418)Calf Muscle PumpThe calf muscle pump helps overcome the effect of gravity to aid with venousreturn for a patient in the standing position. By muscle contraction, the venousvolume is ratcheted back toward the right heart through a series of valves whichopen and close with muscle contraction.Fig. 22: (Pg. 419)Transmural PressureThe transmural pressure is a measure of the difference of the pressure inside thevessel (intravascular pressure) relative to the pressure outside the vessel (tissuepressure). Note that the transmural pressure is always referenced from theinside of the vessel to the outside of the vessel.Intravascular Pressure(higher)Tissue Pressure(lower)Fig. 23: (Pg. 420)Intravascular Pressure(lower)Tissue Pressure(higher)Fig. 24: (Pg. 420)10
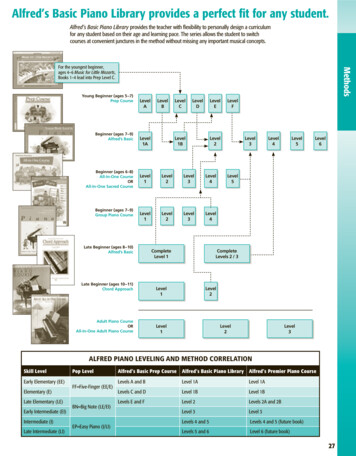
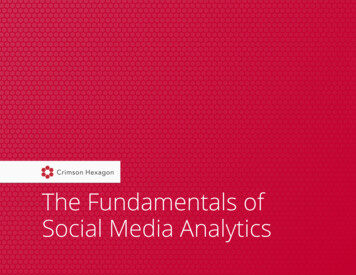
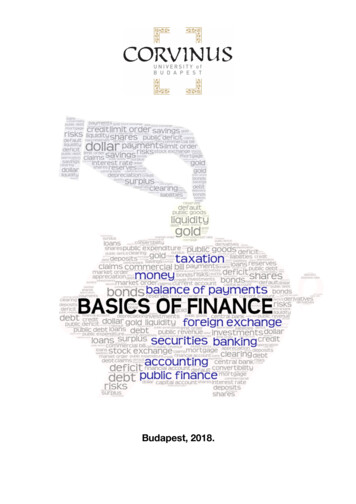
Chapter 13: Level 2Sub-critical DiseaseAt the sub-critical stage of disease, the energy losses under normal metabolicdemand are small enough that the body can adequately compensate, and theend organ is adequately perfused. Since perfusion requirements are met, thepatient is asymptomatic for normal metabolic demand.Fig. 25: (Pg. 421)What Would Happen with Disease and NOArteriole CompensationIn comparison to the pressuregraph of the normal system(shown on an earlier slide), noticethe pressure decreases acrossthe large arteries (whereaspreviously the pressure wasmaintained or actually slightlyincreased). The large pressuredrop across the arterioles nowresults in inadequate pressure toprovide flow across the capillariesand the rest of the CV system.Fig. 26: (Pg. 422)Normal versus Diseased Arteries withAdequate CompensationIn comparison to the graph of the lastslide, notice now that there is adecrease in the pressure droppedacross the capillaries to compensatefor the pressure loss across thearteries as a result of the disease.The decrease in pressure dropacross the arterioles results from thedecreased resistance fromvasodilation of the arterioles. Theresult is now adequate pressure toperfuse the end organ.Fig. 27: (Pg. 422)11
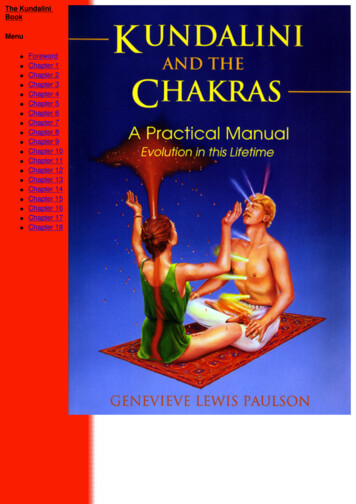
Chapter 13: Level 2Inadequate Compensation(More Severe Disease)In this case, the energy loss acrossthe arteries is so great because ofthe more significant increase inresistance that the arterioles areunable to adequately compensate.As a result, there is inadequateperfusion of the end organ and thepatient is symptomatic even at rest(rest pain).Fig. 28: (Pg. 422)Pressure Gradient with Normal VolumetricDemandTo fully appreciate this slide, a comparison must be made with the next slide.Notice that with the normal metabolic demand, the pressure drop as depictedbelow is related to 4 times the velocity v squared.Fig. 29: (Pg. 423)Increase in Pressure Gradient with Increasein Volumetric DemandIn comparison to the normal volumetric demand, an increase in demand by afactor of four, as can occur with exercise, results in a factor of 4 increase invelocity. Now notice that the pressure gradient, as depicted below, is related to4 times the square of 4v. This represents an increase in the pressure gradientby a factor of 16. This fact explains why exercising a patient often unmaskssub-critical disease.Fig. 30: (Pg. 423)12
Chapter 13: Level 2Critical StenosesWhen the disease becomes critical, the amount of energy lost to frictional andviscous effects become so severe, that volume is not maintained across thelesion. As depicted below, a point is reached at which there is a narrow streamof flow at a high velocity with most of the flow traveling at a relatively low velocity(“string flow”).Fig. 31: (Pg. 423)Velocity and Flow Changes with PercentageStenosisNotice that the volumetric flow ismaintained for percentagedecreases in cross-sectional areaup to about 75%. Past 75%, thevolume begins to drop rapidly.Notice that as the percentstenosis increases, the velocityincreases to maintain thevolumetric flow. Eventually, theincreased energy loss related tofrictional and viscous lossesdominates and the peak velocitydecreases precipitously.Fig. 32: (Pg. 424)Spectral Doppler Assessment ofHemodynamicsSpectral Doppler displays velocity information versus time. From the Dopplerspectrum, the peak velocities, the mean velocities, the variance in velocity, andacceleration/deceleration can be visualized and measured. By understandingthe hemodynamic laws which govern flow and relating those concepts tovelocity and changes in velocity, Doppler can therefore be used to assessmany hemodynamic situations.13
Chapter 13: Level 2Systolic Acceleration and PressureStep 1: Relate pressure with volume change. P Q RSo as the pressure increases, the volume increasesFig. 33: (Pg. 425)Step 2: Relate volume change with velocity change.Q v areaSo as the volume increases, the velocity increasesFig. 34: (Pg. 425)Measuring AccelerationAcceleration v tFig. 35: (Pg. 425)Doppler Risetime for a Diseased VesselWith proximal disease, the volume of flow cannot increase as rapidly withincreasing systolic pressure, decreasing the acceleration. The decrease inacceleration results in a longer risetime. Typically, a risetime of greater than 144msec is indicative of a flow limiting proximal stenosis.Fig. 36: (Pg. 425)14
Chapter 13: Level 2Spectral WindowsThe presence of a spectral window implies the presence of laminar flow. Theconverse is not necessarily true. The absence of a spectral window does notnecessarily imply the absence of laminar flow (turbulence). The loss of thespectral window can be affected by many parameters such as proximity of thesample volume to the vessel wall, a large sample volume or CW Doppler,overgaining, spectral broadening, etc.Fig. 37: (Pg. 426)Spectral Display of TurbulenceIn this case, the absence of the spectral window is indicative ofturbulence resulting from a renal artery stenosis.Fig. 38: (Pg. 426)Relating Pressure Characteristics withSpectral CharacteristicsFig. 39: (Pg. 427)15
Chapter 13: Level 2Arterial Signal ComponentsThe normal lower extremityarterial signal is multi-phasicwith a rapid, antegradeacceleration during systolefollowed by one or morediastolic componentsaca: rapid accelerationb: short flow reversal causedby high resistance ofdistal bedbFig. 42: (Pg. 428)c: diastolic forward flowcomponent.Doppler IndicesResistive Index:A - B Systolic Diastolic ASystolicPulsatility Index:A - B Systolic Diastolic vmean velocitySystolic Diastolic Ratio:Fig. 43: (Pg. 429)ASystolic B DiastolicBruits in DopplerFig. 44: (Pg. 430)Doppler BruitFig. 45: (Pg. 430)Fig. 46: (Pg. 430)Harmonic BruitFluttering Bruit16
Chapter 13: Level 2Flow ExamplesThe following slides are taken from the animation CD demonstrating various flowconditions and states (videos courtesy of Flometrics of Solana Beach California).It is very beneficial to review the animation CD for more in depth descriptions.Stent Entrance (Animation)(Pg. 430)Stent Exit (Animation)(Pg. 431)17
Chapter 13: Level 2Blood Reservoir (Side View) (Animation)(Pg. 431)Blood Reservoir (Top View) (Animation)Carotid Bifurcation Flow (Animation)(Pg. 431)18
Chapter 13: Level 2Flow in an Aneurysm (Animation)(Pg. 431)Add TitleBlank Slide:This blank slide is here to help facilitate adding new content. If you would liketo add material to this presentation, copy this slide and place in the correctlocation.19
Sub-critical Disease At the sub-critical stage of disease, the energy losses under normal metabolic demand are small enough that the body can adequately compensate, and the end organ is adequately perfused. Since perfusion requirements are met, the patient is asymptomatic for normal metabolic demand. Fig. 25: (Pg. 421)