Transcription
2016Greater Lowell CommunityHealth Needs Assessmentin partnership with
2016Greater Lowell CommunityHealth Needs Assessmentin partnership with295 Varnum Avenue, Lowell, MA 01854-2193978-937-6000 TTY:978-937-6889 www.lowellgeneral.org
ACKNOWLEDGEMENTSWe would like to acknowledge and thank thefollowing individuals and organizations for theirassistance with the community health needsassessment and this report:Kerrie D’Entermont, Executive Director, GreaterLowell Health Alliance for her help with schedulingfocus groups and key informant interviews andparticipant recruitment;Focus group facilitators and note takers that arelisted in Appendix D;Paul Oppedisano, MassCHIP Director from theMassachusetts Department of Public Health forproviding public health data;University of Massachusetts Lowell Graduatestudent Katerin Ramirez and undergraduatestudents Daniel Barros, Syeda N. Nizami and ElenaMottola, for secondary qualitative data analysis andcreation of bar charts and graphs for the report andgraduate student Arthur Atokpa for proof reading thedraft;Members of the 2016 Community Health NeedsAssessment Advisory Committee (see Appendix E)and Greater Lowell Health Alliance, for their adviceand guidance;The Lowell Community Health Center, CambodianMutual Assistance Association (CMAA), Hungerand Homeless Commission, Lowell Senior Center,Massachusetts Alliance of Portuguese Speakers(MAPS), Non-Profit Alliance (NPA) and UpperMerrimack Valley Public Health Coalition forhosting focus groups and Edina Braga for recruitingindividuals from the Brazilian community toparticipate in a focus group;We also thank all of the individuals who participatedin the focus groups and interviews and all thosewho provided assistance with the community healthneeds assessment.Greater Lowell Community Health Needs AssessmentConducted on behalf of Lowell General Hospital andGreater Lowell Health AllianceAuthors: David Turcotte, ScD; Emily Chaves, MA, MSc;Michele Ross, MA,; and Kelechi Adejumo, MScUniversity of Massachusetts LowellSeptember 2016Executive Summary1Introduction3Community Health Needs Assessment Partners3Methodology4Service Area and Population5Findings about Community Health and Needs7Overall Perception About Community Health8Top Health Problems in the Community8Types of Residents at Greatest Risk9 Major Strengths of the Healthcare System12Major Weaknesses or Unmet Needs in the Healthcare System 13Barriers to Obtaining Healthcare Services14Analysis of Public Health Data16Figures – General Health21Figures – Mental Health 24Figures – Diabetes24Figures – Substance Abuse25Figures –Cardiovascular Disease28Figures – Obesity30Figures – Respiratory Diseases34Figures – Cancer38Figures – Hepatitis B39Social Determinants and Environmental FactorsAffecting Community Health41Recommendations to Improve the Healthcare System 46Next Steps: Identifying Top Priorities and Action Plans 49References & Appendices 51References 52Appendix A – Focus Group Attendees53Appendix B – Individuals Interviewed59Appendix C – Focus Group and Interview Questions 54Appendix D – Focus Group and Interview Note Takersand Facilitators 55Appendix E – 2016 Community Health NeedsAssessment Advisory Committee55
EXECUTIVE SUMMARYLowell General Hospital, in partnership with theGreater Lowell Health Alliance, commissioned theUniversity of Massachusetts Lowell to conduct anassessment of community health needs for theGreater Lowell area, which includes the towns ofBillerica, Chelmsford, Dracut, Dunstable, Lowell,Tewksbury, Tyngsborough, and Westford. Thepurpose of this assessment includes evaluatingthe overall health of residents by involving a broadspectrum of community members, identifying thetop health issues and strengths and weaknesses ofthe healthcare network, recommending actions toaddress priority concerns, and providing informationthat informs a community process to buildconsensus around strategies to improve the healthof Greater Lowell residents.This report summarizes the major findings from ourcommunity health needs assessment. Primary datacollection included interviews with four keyinformants and sixteen focus groups with 167participants, and secondary data sources includeddemographic, socioeconomic, and public healthdata, as well as local reports.The top health problems that were identified in thefocus groups and interviews in order of preferenceand supported by public health data include mentalhealth (e.g. depression), diabetes, substance abuse,hypertension and obesity (had the same level ofpreference), and respiratory diseases (e.g. asthmaand chronic obstructive pulmonary disease). Theresidents identified at greatest risk for these andother health problems include those with mentalhealth issues, those with substance abuse/addictionissues, immigrants, refugees, other non-Englishspeakers, and the elderly.providers, the strong community hospital and healthcenter, as well as a strong continuum of care.between Lowell’s urban community and thesurrounding suburban towns.The major weaknesses identified include fragmentedcare and lack of communication between providers,insufficient patient education about general health,lack of education about family planning andaccessing services for family planning, inadequatetransportation for patients, lack of insuranceand insufficient coverage (dental and vision careespecially), lack of diversity and cultural competencyand awareness of LGBTQ health issues. In addition,other weaknesses included a shortage of behavioraland mental health services, a lack of integratedmental health and substance abuse services andservices in general, insufficient physicians trainedto work with the elderly, a lack of education amongproviders about pediatric mental health issues andstrategies to educate diverse cultural groups abouthealth, limited access to specialty care for nonEnglish speakers, lack of translators and additionalinterpretation (especially for emergency services)and LGBTQ services, and the difficult-to-navigateinsurance and healthcare system.Social determinants of health and environmentalfactors that affect community health are alsohighlighted. Housing affordability is an issue asindividuals and families may have problems affordingnecessities such as food, clothing, medical care andtransportation. Lowell has the highest gross rent as apercent of income in the area (2010-2014 AmericanCommunity Survey) and is the fourth most expensivecity in Massachusetts (National Low Income HousingCoalition, 2016). Homeless individuals can havedifficulty maintaining their health due to lack ofbasic necessities and poor insurance coverage. Themajority of Lowell’s housing stock is old. About halfof the housing stock was built in 1939 or earlier,and 85% was built in 1979 or earlier (2010-2014American Community Survey), leading to higherrates of lead exposure and increased exposure toasthma triggers. The large numbers of multifamilyhousing units in Lowell also contributes to higherexposure to environmental tobacco smoke. Accessto nutritious foods is adequate, though moreaffordable nutritious foods are less accessible tothose without transportation.The key barriers to obtaining healthcare servicesthat were identified include lack of providers, longwaits for appointments for those with MassHealth,lack of access to care due to patient work hours,cultural barriers and cultural competency issues,communication difficulties between LGH and LCHC,lack of transportation (especially for referrals locatedin Boston), inadequate insurance and understandingof the healthcare system, insufficient services andresources for addicts, the general approach of usingmedicine as the first response to health problems,lack of education about health care in general andlack of self-advocacy and patient education.The major strengths of the healthcare systemidentified include the increased availability andquality of health services in the area, collaborationand communication between Lowell General Hospital(LGH), the Lowell Community Health Center (LCHC),area providers, the various programs, and thecommunity, increase in the availability of doctorsand walk-in facilities, improved access to insurance,improved coverage for those with MassHealthinsurance, and good translation and interpretingservices, increased cultural diversity amongIndicators of health based on public health andother secondary data are presented and discussedfor Lowell, Greater Lowell, and Massachusetts on thefollowing topics: general health, diabetes, substanceabuse, mental health, cardiovascular disease,obesity, respiratory diseases, cancer, and hepatitisB. Most of the health indicators show greater needfor the city of Lowell than Greater Lowell. This isexpected because of socioeconomic differences1The next step is to identify top priorities and actionplans using the information provided in this report.Lowell General Hospital and the Greater LowellHealth Alliance are committed to a collaborativeapproach involving other community stakeholders.Key recommendations to improve the healthcaresystem from focus groups and interviews includeincreasing community health education on severaltopics including the healthcare system, as well aseducation for first responders on mental healthpatients, increases in various services, increasesin homeless shelters and affordable housing andhealthcare access for homeless individuals, adoptinga more global approach to healthcare, increasingprovider awareness of locally available social servicesand LGBTQ community health needs, increases inprimary care providers with geriatric experience,greater provider collaborations, improvements inreimbursements, an increase in interpreters andcultural competency, integration of dental healthwith primary care. Recommended changes to thehealthcare system are also presented, as well assuggestions from the Cambodian, African, Brazilian,Portuguese speaking, and Latino communities.2
INTRODUCTIONPARTNERSMETHODOLOGYIn July 2012, Lowell General Hospital joined theparent organization, Circle Health, and mergedLowell General Hospital and the former SaintsMedical Center into one unified system for theGreater Lowell area, including the city of Lowelland seven surrounding towns: Billerica, Chelmsford,Dracut, Dunstable, Tewksbury, Tyngsborough andWestford. The new Circle Health System unifiedhealth providers in Greater Lowell and continues towork toward significant quality improvements andcost savings in the delivery of healthcare inthe region.Lowell General Hospital in partnership with theGreater Lowell Health Alliance intend to use theinformation within this report to inform a communityprocess in collaboration with other stakeholders toidentify priority health needs and develop actionplans to improve the local healthcare system andoverall community health.This assessment involved primary data collectionusing focus groups and key informant interviews,as well as secondary data sources, such as theMassachusetts Department of Public HealthMassCHIP database and the United StatesCensus. A more detailed description is below.Lowell General Hospital is an independent, not-forprofit, community hospital serving the Greater Lowellarea and surrounding communities. With two primarycampuses located in Lowell, Massachusetts, thehospital offers the latest state-of-the-art technologyand a full range of medical and surgical services forpatients, from newborns to seniors.To fulfill its commitment to the community andstatutory requirements, Lowell General Hospital, inpartnership with the Greater Lowell Health Alliance,contracted with the University of MassachusettsLowell Center for Community Research andEngagement to conduct an assessment of communityhealth needs. The University of MassachusettsLowell team that worked collaboratively to completethis assessment included faculty, staff, students andcommunity partners. The objectives of this studywere to:The Greater Lowell Health Alliance of the CommunityHealth Network Area 10 is comprised of healthcareproviders, business leaders, educators, and civic andcommunity leaders with a common goal to help theGreater Lowell community identify and address itshealth and wellness priorities. Assess the overall health of area residents Identify the strengths and weaknesses of thelocal healthcare system Determine the top health problems facing arearesidents and the populations at greatest risk Involve a broad spectrum of professionals andresidents, including newer immigrant communities Provide recommendations to improve thehealthcare system and address unmethealth needs Inform the process to identify priority healthneeds and develop action plans to addressthese priority needshealth directors, nurses and agents, first responders(including police, fire and ambulance), Circle Healthleaders, non-Circle Health providers, physicians,Greater Lowell Health Alliance members, and LowellGeneral Hospital Patient Family Advisory Councilmembers. The Non-Profit Alliance of Greater Lowell(NPA) and the Hunger and Homeless Commissionallowed us to conduct the focus group during thetime allotted for their March and April monthlymembers’ meeting. The Upper Merrimack ValleyPublic Health Coalition helped organize and recruittheir members for the public health directors, nursesand agents focus groups. Individuals were asked toparticipate as private individuals and not as officialspokespersons for their organizations.Focus GroupsSixteen focus groups with 167 total participantswere conducted from February 2 through April20, 2016 (see attendees who agreed to havetheir name published in Appendix A). Each focusgroup averaged 90 minutes and included 7-9questions, depending on the group (see questions inappendix C). Focus group questions inquired aboutperceptions of overall health of community, tophealth problems in the community, who is at greatestrisk, the strengths and weaknesses of healthcarein Lowell and Greater Lowell, and suggestionsfor improvements to the healthcare in Lowell andGreater Lowell. The Portuguese speaking, Latino,African, Cambodian and Brazilian focus groups werealso asked to comment on the healthcare prioritiesspecific to their communities and the overall qualityof the healthcare system and its ability to meetneeds specific to their communities.The other six focus groups represented variousimmigrant and ethnic communities including theBrazilian community, the Cambodian community,the African community, the Latino community, thePortuguese community, as well as participants ofTeen Block at the Lowell Community Health Center.Key Informant InterviewsThe University of Massachusetts Lowell conductedfour interviews that included an individual whorequested anonymity. Individuals were identifiedby Lowell General Hospital, Greater Lowell HealthAlliance and members of the 2016 CommunityHealth Needs Assessment Advisory Committee,as key community informants because of theirpositions and knowledge of community health needs(see appendix B). These individuals were asked toparticipate as private individuals and not as officialspokespersons for their organizations. Key informantinterviews averaged 45 minutes and included thesame questions used in the focus groups. As withthe focus groups, notes were taken and recordingswere made for all key informant interviews.The team of nine focus group facilitators includedUMass faculty, undergraduate and graduatestudents, as well as individuals from the CambodianMutual Assistance Association and LowellCommunity Health Center (see list of facilitators inappendix D). Focus groups were generally conductedin English, with the exception of the Cambodiancommunity group which was conducted in Khmerand the Latino group, which was in Spanish.Notes were taken and recordings were made forall focus groups.This report summarizes the major findings from ourcommunity health needs assessment.The composition and number of the focus groupsorganized and the list of individuals invited weredetermined in collaboration with Greater LowellHealth Alliance, Lowell General Hospital, and the2016 Community Health Needs Assessment AdvisoryCommittee, as well as other community partners.Analysis of Secondary Data SourcesMost population health data were obtained fromthe Massachusetts Community Health InformationProfile database (MassCHIP), which is maintainedby the Massachusetts Department of Public Health.We also received data on incidences of non-invasivecancers from the Massachusetts Cancer Registry.This data was used to provide an overview of healthstatus of residents of Lowell General Hospital’sTen focus groups were organized by professional ororganizational grouping: nonprofit organizations,organizations providing senior services, public34
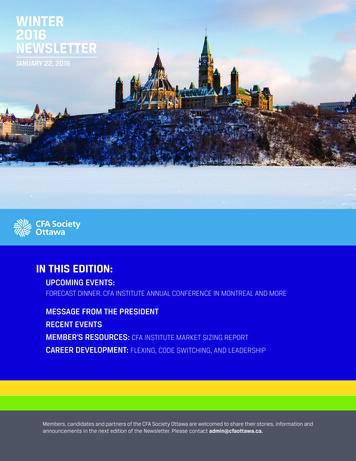
Service Area and PopulationThe Greater Lowell area had an estimated populationof 282,520. The City of Lowell is estimated to have108,491 residents, which represents over 38%of the area’s population. Billerica is the largestcommunity outside of Lowell with 41,446 residents.Chelmsford, Dracut and Tewksbury are next inpopulation size, with 34,495, 30,350 and 29,718respectively. The smallest community is Dunstablewith a population of 3,299.service area, the Greater Lowell Community HealthNetwork Area (also known as CHNA-10). Datawere comparatively analyzed and presented at theLowell, Greater Lowell CHNA, and statewide levels.We analyzed and presented data on the City ofLowell because it is the largest and most diversecommunity and has greater health issues and needs.Data are presented using bar charts and graphs. Themost important health information included wasdetermined based on findings from focus groupsand key informant interviews. Additional datasources included the US Census, the MassachusettsHealth Data Consortium (courtesy of LowellGeneral Hospital), local newspaper articles, localgovernmental reports, as well as local organizationaland research reports.The City of Lowell, as the largest community, differssignificantly from its surrounding suburbs. Since itsfounding in 1820 as a planned industrial city fortextile manufacturing, the City of Lowell has been agateway for immigrants arriving to Massachusetts.Immigration has been an important factor forLowell’s population growth in its early history andpopulation stability over the last 30 years. In the1800s, immigrants predominately arrived fromEurope and Quebec, Canada. More recently, arrivalshave come from Latin America, Asia and Africa.Accordingly, Lowell has the largest percent of foreignborn at 25.2% in the service area. In contrast, mostsuburban communities have 10% or fewer foreignborn, with Westford the exception at 13.8%. Lowellis also more diverse, with 42% non-white withAsian and Latino populations at 20.9% and 18.2%respectively. Westford and Chelmsford have sizableAsian populations, 14.8% and 8.1%, respectively,compared to other area towns.LimitationsThe findings from the focus groups and interviewsare from a qualitative, non-random sample. Theyreflect the opinions of those participating and arenot necessarily representative of all residents theGreater Lowell community. In addition, we analyzedpublic health surveillance data to provide additionalevidence of community health needs, but in somecases the data is 3-4 or more years old and may notreflect current health needs.The economy of Lowell has also changed significantlysince the 1800s; it is no longer an economic centerfor the region. As the overall regional economyhas moved from traditional manufacturing to hightechnology and services, the number of jobs inLowell has declined significantly; few manufacturingjobs remain. As is common in today’s economy,immigrants who lack higher education encountera job market consisting of mainly low-payingservice jobs which lack the upward mobility of thehistorically available manufacturing opportunities.While Lowell’s unemployment rate is the highestin the region at 6.5%, it has declined from 9% in2013. Lowell also has the highest poverty rate at19.1%, markedly higher than other communities.Overall, Lowell is the least affluent community with amedian household income of 49,164, which is lessthan half the income of the towns of Westford and5Dunstable at 125, 143 and 116, 125 respectively.Lowell’s median family income also lags behind theaverage for gateway cities in Massachusetts, accordingto a report by the Massachusetts Budget and PolicyCenter (Welker, 2016). Income inequality as well asother social determinants of health are discussed inmore detail in the Social Determinants section.Table - Basic Demographic Data, Cities/towns in the Greater Lowell CHNACity/TownPopulation %% Foreign % Aged %% BelowWhite Born0-17AgedPoverty65 Billerica41,44691.0 9.121.213.05.6Chelmsford34,49589.7 10.821.017.53.5Dracut30,35088.5 7.523.112.85.0Dunstable3,29994.9 ksbury29,71893.7 6.520.615.94.0Tyngsborough 11.12.7Total/Weight- 282,52077.215.322.612.610.1ed AverageMassachusetts 6,657,291 80.0 15.321.114.411.6Data retrieved from the American Community Survey 2010-2014 5 year 87,49693,108125,14391,903%%Black .467,8467.05.810.2
Overall Perception About Community HealthFindings AboutCommunity Healthand Needsit manifests in a geographic contrast between poorerhealth in the lower income urban areas of Lowell,and better health in the suburban areas, especiallyin the more affluent towns like Westford. As inour 2013 report, specific health issues identifiedas being associated with SES or geographic areainclude health awareness and education, diet,physical activity, insurance coverage and access toproviders and healthier housing in general.The majority of professional and provider focusgroups and two key informants perceived Lowell andGreater Lowell residents to be generally unhealthy.One professional focus group perceived Lowelland Greater Lowell residents to be in fairly poorhealth. Three professional and provider focus groupsperceived Lowell and Greater Lowell residents to begenerally healthy. Of the professional and providerfocus groups who perceived residents as generallyunhealthy or in fairly poor health, the majority arein direct delivery of care–with exception was thePhysicians’ focus group, which perceived residentsas healthier in Westford, and readily acknowledgedthat income determines insurance options whichoften determine health choices. One key informantindicated that “there are [health] issues that aremore prevalent in urban communities with lowincome, immigrant, residents.” The professionaland provider focus groups who perceived residentsas generally healthy, the majority of which are notinvolved in the direct delivery of care, cited thatresources at Lowell Community Health Center arevery good and that providers have good connectionsto other social service agencies.The crisis of substance abuse was acknowledged byevery focus group in response to an overwhelmingnumber of questions. Substance abuse and relatedmental health issues are concerns described in moredetail in the sections titled Top Health Problems inthe Community, Types of Residents at Greatest Riskand Major Weaknesses and Unmet Needs in theHealthcare System.Top Health Problems in the CommunityTop health problems are listed in order of importancebased on the focus groups and interviews.Mental health - The majority of both provider/professional focus groups and community focusgroups identified mental health issues, includingstress, depression, PTSD and anxiety, as top healthissues for Lowell and Greater Lowell residents.Provider/professional focus groups acknowledgedan increase in mental health issues in childrenand young adults. As in our 2013 report, thosewith mental health issues were named as a type ofresident at greatest risk for poorer health and unmetneeds. One key informant stated “there are a highincidence of addiction and mental health issueshere.” On provider/professional focus group cited anincrease in dual diagnosis patients – mental healthand addiction issues.See page 24 for related public health data.The majority of community focus groups alsoperceived Lowell and Greater Lowell residents asgenerally unhealthy. The groups that perceivedresidents as generally unhealthy were the Latinofocus group, African community focus group,the Cambodian focus group and the Portuguesespeaking community focus group. However, theBrazilian focus group perceived their overallhealth status as average. Among issues cited werelong working hours, lack of support networks andtranslated materials, insufficient understandingabout medication, chronic disease, following doctors’instructions, and the high cost of healthy food.While the remaining community focus group feltthat residents were generally healthy, they, too, citedlack of access to care, cultural barriers to care, lowsocioeconomic status (SES), and lack of access tohealth food as concerns for their communities.Diabetes - The majority of both provider/professionalfocus groups and community focus groups identifieddiabetes and diabetes related health concerns astop health issues for Lowell and Greater Lowellresidents. Two provider/professional focus groupsfelt that there is a need for access to healthierfood options, including healthy fast food options.Community groups also cited the lack of accessThere is an awareness among all focus groupsthat health varies based on SES. Among provider/professional focus groups, there is a perception that78
to healthy food options as well as the high cost ofhealthy food as concerns in their communities. Oneprovider/professional group cited a concern for theincrease in diabetes in the Cambodian community.See page 24 for related public health data.respiratory disease (including smoking relatedconcerns and COPD) as top health issues for Lowelland Greater Lowell residents. See page 34 for relatedpublic health data.Other health issues raised by provider/professional,community focus group participants and keyinformants include poor dental health due to lack ofinsurance and providers, heart disease, back painand seasonal allergies.Substance abuse and addiction - The majorityof both provider/professional focus groups andcommunity focus groups identified substance abuseand addiction issues, including alcohol addiction,as top health issues for Lowell and Greater Lowellresidents. Two provider/professional groups expressedconcern for the number of babies born with opioidaddiction issues. One professional/provider groupacknowledged that Lowell is a ‘hot spot’ for opioidissues, it is also a growing problem in surroundingtowns. First responders cited an increase in drugrelated mental health issues among residents.Community groups expressed concern at the lack ofservices/care for drug and alcohol addicted in theircommunities. See page 25 for related public health data.Behaviors or conditions that were named ascontributing to poor health include low SES, poornutrition, smoking, domestic violence, elder abuse,and stress.Types of Residents at Greatest RiskTop health problems are listed in order of importancebased on the focus groups and interviews.Those with Mental Health IssuesProvider/professional as well as community focusgroup participants and key informants indicated thatfor those dealing with mental health issues, there isnot enough funding for care. For those with mentalhealth issues who have Mass Health and Medicarehealth plans, mental health coverage is insufficient.Access to mental health services is very difficultfor the undocumented population. There are manypeople with dual diagnosis of substance abuse andmental health issues and there is a lack of servicesfor this population. Participants acknowledged thelink between mental health issues, drug addictionand overdose.Hypertension – All five ethnic and immigrantcommunity focus groups indicated that high bloodpressure and related issues were health concernsfor their communities. See page 28 for related publichealth data.Obesity - The majority of both provider/professionalfocus groups and community focus groups identifiedobesity, including lack of exercise and healthy diet,lack of nutritional education, and sedentary lifestyleas top health issues for Lowell and Greater Lowellresidents. One provider/professional focus groupacknowledged a rise in early childhood obesity.Another expressed concern for the lack of patientunderstanding about healthy weight. Participantsin the Teen Block community focus group sharedthat, while there is an increase in awareness ofweight management and staying healthy, the lack ofavailability of healthy snacks around homes resultsin unhealthy snacking habits because unhealthysnacks are more readily available. See page 30 for relatedpublic health data.Those with Substance Abuse/Addiction IssuesProvider/professional as well as community focusgroup participants expressed concern that thereis a lack of services, funding, counseling andcare for those addicted to drugs and alcohol inthe community. They indicated a high no showrate for the services that are available. Focusgroup participants indicated an increase in thenumber of infants born with addiction issues, andacknowledged that there is a lack of establishedprograming in the area designed to help mothersand children with substance abuse. Participants alsoacknowledged the link between mental health issues,Asthma and respiratory disease - The majorityof both provider/professional focus groups andcommunity focus groups identified asthma and9drug addiction and overdose. A key informantindicated that children are an especially vulnerablepopulation touched by substance abuse issues:school age children “growing up just alone in ahousehold where drug use is a crime.it impairstheir ability to be successful.” Many of thesechildren ar
Coalition, 2016). Homeless individuals can have difficulty maintaining their health due to lack of basic necessities and poor insurance coverage. The majority of Lowell’s housing stock is old. About half of the housing stock was built in 1939 or earlier, and 85% was built in 1979 or earlier