Transcription
OCTOBER 26–29, 2020
You Weigh In: Medicare for All and theLatest Wave of Health Policy ProposalsAndrew Loewer & Chris SloanModerator: Chiara DragoOctober 29, 2020
SOCIETY OF ACTUARIESAntitrust Compliance GuidelinesActive participation in the Society of Actuaries is an important aspect of membership. While the positive contributions of professional societies and associations arewell-recognized and encouraged, association activities are vulnerable to close antitrust scrutiny. By their very nature, associations bring together industry competitorsand other market participants.The United States antitrust laws aim to protect consumers by preserving the free economy and prohibiting anti-competitive business practices; they promotecompetition. There are both state and federal antitrust laws, although state antitrust laws closely follow federal law. The Sherman Act, is the primary U.S. antitrust lawpertaining to association activities. The Sherman Act prohibits every contract, combination or conspiracy that places an unreasonable restraint on trade. There are,however, some activities that are illegal under all circumstances, such as price fixing, market allocation and collusive bidding.There is no safe harbor under the antitrust law for professional association activities. Therefore, association meeting participants should refrain from discussing anyactivity that could potentially be construed as having an anti-competitive effect. Discussions relating to product or service pricing, market allocations, membershiprestrictions, product standardization or other conditions on trade could arguably be perceived as a restraint on trade and may expose the SOA and its members toantitrust enforcement procedures.While participating in all SOA in person meetings, webinars, teleconferences or side discussions, you should avoid discussing competitively sensitive information withcompetitors and follow these guidelines: Do not discuss prices for services or products or anything else that might affect prices Do not discuss what you or other entities plan to do in a particular geographic or product markets or with particular customers.Do not speak on behalf of the SOA or any of its committees unless specifically authorized to do so.Do leave a meeting where any anticompetitive pricing or market allocation discussion occurs.Do alert SOA staff and/or legal counsel to any concerning discussionsDo consult with legal counsel before raising any matter or making a statement that may involve competitively sensitive information.Adherence to these guidelines involves not only avoidance of antitrust violations, but avoidance of behavior which might be so construed. These guidelines only providean overview of prohibited activities. SOA legal counsel reviews meeting agenda and materials as deemed appropriate and any discussion that departs from the formalagenda should be scrutinized carefully. Antitrust compliance is everyone’s responsibility; however, please seek legal counsel if you have any questions or concerns.
Presentation DisclaimerPresentations are intended for educational purposes only and do not replaceindependent professional judgment. Statements of fact and opinions expressed arethose of the participants individually and, unless expressly stated to the contrary, arenot the opinion or position of the Society of Actuaries, its cosponsors or itscommittees. The Society of Actuaries does not endorse or approve, and assumes noresponsibility for, the content, accuracy or completeness of the informationpresented. Attendees should note that the sessions are audio-recorded and may bepublished in various media, including print, audio and video formats without furthernotice.
BiographiesChiara Drago, Evolent HealthChiara studied at the University of Waterloo in Canada. Following graduation, she moved to Chicago to work for the Milliman HealthPractice where she focused on ACA rate filings, Medicare Part D bid development, and pharmaceutical analysis for drugmanufacturers and large employer groups. Chiara recently joined the Risk and Quality Analytics team at Evolent Health where herresponsibilities include quality reporting oversight and development of risk score forecasting models for Medicaid partners. Chiaracontinues to take actuarial exams in pursuit of her FSA.Andrew Loewer, Evolent HealthAndrew Loewer, FSA works at the intersection of actuarial science, data analytics, and public policy in Washington, DC for clientslooking to understand the financial impact of quickly evolving value-based care and risk-based relationships that are transformingour health system in Medicare, Medicaid, and the ACA marketplaces. In his current role at Evolent Health, he manages a team ofactuaries and data scientists that produce analytics, models, and forecasts around risk adjustment and quality metrics inhealthcare. In his spare time, he enjoys hiking, camping, traveling, and a nice glass of wine.Chris Sloan, Avalere HealthChris Sloan, Associate Principal, advises a number of clients, including pharmaceutical manufacturers, health plans, providers,and patient groups on key policy issues facing the healthcare industry. Chris’s economic analyses of key policy proposals andissues, including drug pricing and the repeal and replace efforts around the Affordable Care Act, have been featured in a widerange of publications, including the Wall Street Journal, the New York Times, the Washington Post, Politico, Axios, and Vox.Chris’s work has also been cited by policy makers on the Senate floor and by the Congressional Budget Office.
Starting Questions
What best represents yourprofession?1. Traditional health actuary (pricing, reserving,forecasting)2. Non-traditional health actuary (value-based care,risk arrangements, policy)3. Non-health actuary (life, disability, pension)4. Other healthcare professional5. Other policy-focused professionalPOLLING QUESTIONOPINION POLL
Rank the biggest challenges with theUS healthcare system1. Member churn / enrollment changes / inability toinvest long-term2. Data / EMR interoperability / coordination &continuity of care / claims payment / paperwork /overhead3. Uninsured & underinsured members /uncompensated care4. Narrow networks / inadequate benefit design5. High costs / price transparency / hidden orinequitable subsidiesPOLLING QUESTIONOPINION POLL
How would you rate the current UShealthcare system?1. The current system works pretty well for most people,a few slight modifications are enough2. Modifications within the existing framework of payerswould make significant improvements without majordisruption.3. One or more major payers need comprehensivereform but big parts of the system can remainessentially as-is.4. We should start from scratch and eliminate all or mostcurrent payers (employer, Medicare, Medicaid, etc.)POLLING QUESTIONOPINION POLL
Current Environment
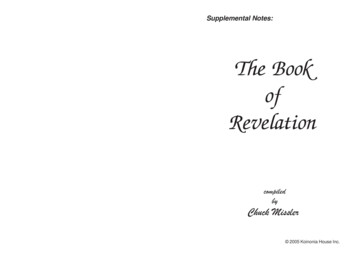
Healthcare Reform is Responding to Key Areas ofFriction in the Healthcare Environment30MUninsured individuals in 2019and growing67% 84% 90%of consumers filing bankruptcycited healthcare as primaryreasonof consumers believedrug prices areunreasonableof consumers supportMedicare pricenegotiation21% 102M 31% 21Kof Americans areunderinsuredAmericans have a preexisting conditionof employees are enrolledin a health deductiblehealth planAverage annual employeefamily health benefit cost
Public Payers are Growing as a Share of the US NationalPayer MixEmployer% of Enrollment(Pre-COVID)Average PremiumAverage SpendingAverage PaymentRate (% ofMedicare FFS)Average AV46% 104 / 599 /month1month1199%585%2Medicare19%Medicaid21% 145 / month(Part B, most beneficiarieswith income 87,000 /year) 1,058 /month4100%80%(Original Medicarewithout Medigap)3 0ACA72%6 100%Kaiser Family Foundation 2019 Employer Health BenefitsSurvey2.Peterson-KFF Health SystemTracker3.Kaiser Family Foundation How Does the Benefit Value ofMedicare Compare to theBenefit Value of Typical LargeEmployer Plans?4.2020 Medicare TrusteesReport5.Kaiser Family Foundation How Much More ThanMedicare Do Private InsurersPay? A Review of the Literature6.Kaiser Family Foundation Medicaid-to-Medicare FeeIndex7.Medicaid.gov8.Kaiser Family Foundation4% 143 / month (aftersubsidies)8 685 / month7(varies significantlybetween entitlementgroups)1. 612 /month8-68%
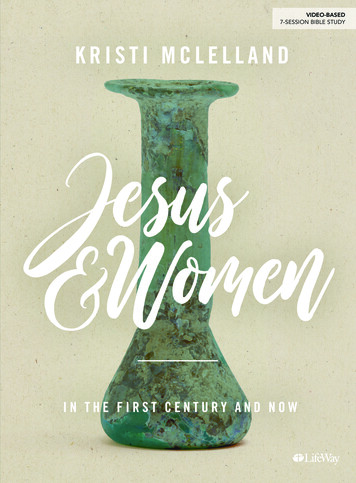
While the Uninsured Face Gaps in Access, Many Qualifyfor Financial Assistance to Purchase CoverageMakeup of Uninsured Population, 201911%Other17%40%30M13%Eligible for Subsidized Coverage Through aMarketplaceNot Lawfully PresentEligible for Medicaid or CHIPLiving in Non-Expansion State & Income LessThan 100% of FPL19%Source: CBO. September 2020. Federal Subsidies for Health Insurance Coverage for People Under Age 65: 2019 to 2029. Link.CHIP: Children’s Health Insurance Program; FPL: Federal Poverty Limit
Medicare-for-All and Public ProgramExpansions
“Medicare-for-All” Has Gone Mainstream as Americansare Increasingly Dissatisfied with their Coverage“Not since the Great Society era has soambitious a social program been soactively promoted by influentialDemocrats. ” – NY Times Magazine HR 1384 – Medicare for All Actof 2019 – 118 cosponsors (of435 members) S 1129 – Medicare for All Actof 2019 – 14 cosponsors (of100 members)Sanders won 1,119 delegates (1,991 needed to win Democraticnomination) including majority from New Hampshire, Nevada,California, Colorado, Utah, Vermont, and North Dakota
Medicare-for-All Can Be Used to Mean a Variety ofCoverage Expansion Policies and ProposalsSingle Payer1 PublicProgram EmployerCoverage“Medicare”for AllWho Want ItNationalPublicOptionMost SweepingACA: Affordable Care Act; CHIP: Children’s Health Insurance Program. ESI: Employer-Sponsored InsuranceExpandMedicareEligibilityState PublicOptionStrengthenthe ACAMore Incremental
“Medicare-for-All” is Not MedicareOriginal MedicareEligibilityMedicare Advantage“Everyone in America” – eliminates Medicare,Medicaid, and private insuranceSeniors & people with disabilitiesPremiumMedicare-for-All* 144.60/month or higher based on incomeVaries, can be as low as 0NoneHospital: 1,408 deductible 352 or 704coinsurance after 60 daysProfessional: 198 deductible 20%coinsuranceNo cap on out of pocket costs. 81% ofbeneficiaries buy Medigap policies or use othersupplemental coverage to cover these costs1Varies but typically includes deductibles andcoinsurance. All plans must have an out-ofpocket max no higher than 6,700 in 2020NoneNetworkNoneMost plans have in-network providersNoneRx Drugs70% buy a Part D plan for 40 / month1Most plans include Part D Rx drug coverageYes, with some cost sharingDental, VisionNoneMany plans includeYesLong-Term CareNoneNoneYes33% of beneficiaries part of MSSP or NG ACOs2YesNoMedical Cost Sharing (2020)Managed Care / Risk Sharing*Based off Senator Sander’s Medicare for All proposal from the 2020 campaign.1)2)Source: Kaiser Family FoundationSource: CMS.gov
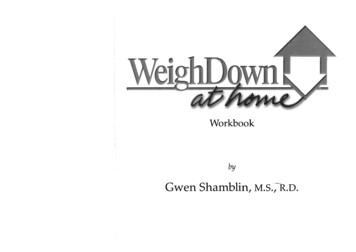
Support of a National Health Plan is Mixed, But HigherWhen Called “Medicare-for-All”Do you support a national health plan if it would Positive Reaction to Following Terms63%71%Guarantee health insurance as a right for all AmericansEliminate all health insurance premiums and reduce out-ofpocket health costs for most Americans63%59%49%46%27%67%37%Eliminate private health insurance companies58%37%Require most Americans to pay more in taxes50%32%Threaten the current Medicare programLead to delays in people getting some medical tests andtreatments60%26%Favor30%70%OpposeSource: Kaiser Family Foundation poll, January 20199%Of Medicare-for-AllSupporters UnderMedicare-for-All Source: Kaiser Family Foundation poll, April 2019Think would be able to keep their currenthealth insurance24%Think would not be able to keep theircurrent health insurance67%Not sureSource: Kaiser Family Foundation poll, January 2019
What is the single most important thingthat healthcare reform should do?1. Universal coverage / fewer uninsured2. Improve premium subsidies / mandate morecomprehensive benefits / less cost sharing3. Control costs / manage utilization / standardizerates paid to providers4. Better coordination between entities5. Enhanced flexibility in product design / VBIDPOLLING QUESTIONOPINION POLL
2020 Election Implications for“Medicare-for-All”
Proposals to Reform the Healthcare SystemRepresent a Wide Spectrum of ChangesMore IncrementalMost SweepingKey PoliciesRetains Public PayersSingle Payer1 PublicProgram ESI “Medicare”for AllWho Want It National PublicOption Medicare BuyIn State PublicOption Strengthen theACA Creates a New Public ProgramExpands Existing ProgramsErodes Commercial CoverageLikelihood Low Low Low Medium Medium Medium FFCRA: Families First Coronavirus Response Act; NIH: National Institutes of Health; FMAP: Federal Medical AssistancePercentage’ CARES: Coronavirus Aid, Relief, and Economic Security ActHigh
Scenario 1White House-RSenate-RHouse-DScenario 2White House-DSenate-RHouse-DScenario 3Election Outcomes Will Dictate Both the Policies andAvenues for ReformWhite House-DSenate- DHouse-DACA: Affordable Care Act; HAO: Healthy Adult Opportunity Program; CMMI: Center for Medicare and Medicaid Innovation*HAO waivers allow state Medicaid programs additional flexibilities, including the implementation of capped financing models, closed formularies, work requirements and various eligibility restrictions
TrumpThe Trump Administration Supports Overturningthe ACA, Which Could Significantly Decrease CoveragePresident Trump is supportive of the case against the ACA, California v. Texas, saying on May 7that his Administration will urge the Supreme Court to overturn the ACA.2018 Texas AG and 18 otherRepublican AGs file suitarguing that the ACA isunconstitutional, given thatthe Tax Cuts and Jobs Actzeroed out the individualmandate tax penalty2019 The 5th Circuit Court rules theACA individual mandate to beunconstitutional Since the mandate is“essential” to the ACA, theCourt concludes that theentire law is potentiallyunconstitutional and askslower court to re-examineACA: Affordable Care Act; AG: Attorney General; SCOTUS: Supreme Court of the United StatesLuthi, S. “Trump will urge Supreme Court to strike down Obamacare.” Politico. May 6, 2020. Available here.Supreme Court Docket. California v. Texas. Available here.2020 & Beyond SCOTUS has scheduled oralarguments of California v.Texas on November 10, a weekafter the elections. A ruling isnot expected until June 2021at the earliest Administration releases anexecutive order promising, butproviding little detail, toprotect pre-existing conditions
TrumpPresident Trump’s Coverage Reform Centers onIncreased Flexibility Across MarketsMedicaidMedicareCommercial and ExchangeMarkets The Trump Administration hassought to incentivize growth of MAand increase program flexibilities. President Trump has not expressedsupport for expanding Medicarecoverage beyond the currentlyeligible population.Through CMS 1332 waivers, theTrump Administration hassupported increased flexibility forstate marketplaces (e.g., flexibilityfor non-QHPs). The Trump Administration has alsosupported reinsurance efforts tohelp states subsidize medical costsof high-risk individuals to reducepremiums. Through CMS’s HAO block grants,states can implement cappedfinancing models and increasedflexibility for coverage requirements.CMS 1115 waivers allow states toseek limits to Medicaid coveragethrough work requirements.These policies are also reflected in a 2019 healthcare plan from the Republican Study Committee highlightingRepublican healthcare priorities in advance of the 2020 elections and are likely to remain priorities under a secondterm.CMS: Centers for Medicare and Medicaid Services; HAO: Healthy Adult Opportunity; MA: Medicare Advantage; FFS: Fee-for-Service; QHP: Qualified Health Plans;Source: The listed reforms have been indicated in past executive action, the President’s budget, and/or the RSC Health Care Plan (2019)
BidenVice President Biden’s Platform Combines “Moderate”Democratic Coverage ReformsWhile there have been discussions on more sweeping changes to coverage reform, Biden’splatform is more moderate, focusing on creating a public option and strengthening the ACA.SinglePayer1 PublicProgram EmployerCoverage“Medicare”for AllWho WantItNationalPublicOptionMost SweepingACA: Affordable Care Act; CHIP: Children’s Health Insurance Program. ESI: Employer-Sponsored InsuranceExpandMedicareEligibilityState PublicOptionStrengthenthe ACAMore Incremental
BidenVP Biden Proposes to Create a Public Insurance Option,Build on the ACA, and Improve Coverage AffordabilityPublic Option As proposed, Vice President Biden’s public option proposal would create a publiclyadministered, “Medicare-like” plan that is available on the exchanges as an alternative toprivate insurance coverage Individuals below 138% FPL in states without Medicaid expansion and not already eligiblefor public coverage would be eligible for premium-free access to the planACA SubsidiesAffordability Provisions Expansion of ACA advanced premium taxcredits (APTC) to families above 400%FPL Recalculation of premium tax creditamounts to help patients in all eligibleincome brackets to better afford moregenerous plansLower threshold of affordability forhouseholds with employer coverage (i.e.,limit total premium amount to 8.5% ofhousehold income, down from above9.86%) Limit “surprise billing”VP: Vice President; FPL: Federal Poverty Line; ACA: Affordable Care Act; OOP: Out-of-Pocket; APTCS: Advanced Premium Tax Credits;Biden for President: Healthcare. Link
BidenBudget Reconciliation Can Make It Easier to PassLegislation by Only Requiring a Simple MajorityHouse ActionJoint ActionSenate Action1.House passes budget resolutionwith reconciliation instructions,including targets & dates for certaincommitteesHouse & Senate reconcilerespective instructions and passjoint budget resolutionSenate passes budget resolutionwith reconciliation instructions,including targets & dates for certaincommittees2.House committees passreconciliation legislation3.House passes reconciliation bill withsimple majority vote4.5.Senate committees passreconciliation legislationHouse & Senate reconcile &pass identical reconciliationlegislationSenate passes reconciliation bill afterlimited debate (20 hours) & simplemajority votePresident signs or vetoes billHouse votes to override Presidentialveto with 2/3 voteNote: The reconciliation instructions are issued by the House and Senate Budget CommitteesSenate debate to overridePresidential veto with 2/3 vote islimited to 10 hours
Would any of the proposals outlined be asignificant improvement over the statusquo?1. Yes, they would alter things for the better2. Maybe, its unclear whether these changes wouldbe better than the status quo3. No, they are largely political talking points, part ofthe election, and ignore the realities abouthealthcare in AmericaPOLLING QUESTIONOPINION POLL
Would disrupting health insurance in theUS be a good thing?1. Disruption and elimination of private insuranceisn’t needed, smaller tweaks can solve many of thecurrent issues2. Insurance and risk sharing entities should continueto play a role in determining how healthcare isfinanced and delivered but with major changes3. I’m ready to go work in life or pensionPOLLING QUESTIONOPINION POLL
Final Thoughts“Medicare-for-All” will continue to be at the forefront of policy conversations about the future of the UShealthcare system. The 2022 midterms and 2024 Presidential race are likely to feature continued calls tomove towards some form of single payer system.In the meantime, any changes are likely to be incremental adjustments to current public programs. If VicePresident Biden wins, and democrats take the Senate, a combination of his policy proposals will likely leadto higher enrollment in public programs and a decrease in the number of uninsured patients.If President Trump wins, health insurance coverage in the United States will remain relatively stable, subjectto the Supreme Court’s ACA decision, and we are unlikely to see any large-scale expansions of publiccoverage for the next four years.
Q&A
You Weigh In: Medicare for All and the Latest Wave of Health Policy Proposals Andrew Loewer & Chris Sloan Moderator: Chiara Drago October 29, 2020. SOCIETY OF ACTUARIES Antitrust Compliance Guidelines Active participation in the Society of Actuaries is an important aspect of membership. While