Transcription
Medicare Risk AdjustmentRAF 101Presenter:Renee White, LPN, CCS, CPC, CPCI, CPMA, CRC1
DisclaimerThe information presented herein is for information purposesonly. HIMS BMG/BUMG Documentation and Coding EducationTeam has prepared this education using Banner Health Ethicsand Compliance approved regulatory and industry authoritativeresources. It is designed to provide accurate and authoritativeinformation on the subject matter. Every reasonable effort hasbeen made to ensure its accuracy. Nevertheless, the ultimateresponsibility for correct use of the coding system and thepublication lies with the user. Any codes are to be used for easyreference; however, the CPT code book and ICD-10-CM codebooks and the Official Guidelines for Coding and Reporting arethe authoritative references for accurate and complete coding.HIMS BMG/BUMG warrants that the information containedherein is accurate and up to date according to the approvedauthoritative resources, but may not be free from defects.2
Abbreviations RAF: Risk Adjustment Factor MRA: Medicare Risk Adjustment CMS: Centers for Medicare & MedicaidServices RA: Risk Adjustment MA: Medicare Advantage HCC: Hierarchical Condition Categories MEAT: Monitor, Evaluate, Address, Treatment3
ObjectivesProvide Overview of Medicare RiskAdjustment (MRA)Identify the role of Health Care Providers inthe Medicare Risk Adjustment processProvide medical record documentationguidelines4
Purpose MRA is intended to redirect money away fromMAO that would cherry-pick the healthierenrollees MRA is a way to provide MAO that care for thesickest patients the resources to do so5
Reimbursement Model RAF-HCC RAF-HCC is a predictive model CMS usesdiagnosis data submitted from the previousyear to establish capitation payments to theMA plan6
HCC’s are disease categories which are mappedto certain Diagnosis Codes for chronic conditions: 79 HCC’s and over 8830 ICD-10-CM diagnosiscodes out of 70,0007
8
I’m CuredCMS wipes the slateclean every January 1,so MA plans mustrecapture all chronicconditions in order toreceive reimbursement9
How it WorksThe average CMS FFS patient has the score of 1.00 RAF is a numeric value assigned by CMS toidentify the health status of a patient RAF scores are made up of the following criteriafor each member:Demographic information e.g. age and sexMedicaid status and Medicare eligibility dueto a disabilityChronic conditions and disease interactions10
How it Works2 RAF-HCC is a predictive model using diagnosissubmitted from the previous year to establishcapitation payments to the MA plan Each diagnostic code falls into one DiagnosisGroup and codes are grouped into ConditionCategories11
Disease Interaction DM and CHF DM and CVD CHF and COPD COPD, CVD and CAD RF and CHF RF, CHF and DM12
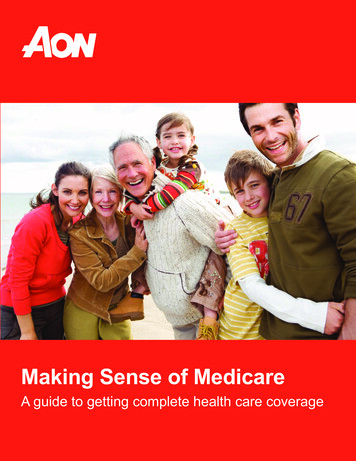
Low level of specificityHigh level of specificityModerate level of specificity76 year old female0.42676 year old female0.42676 year old female0.426Medicaid eligible(aged female 65 )0.202Medicaid eligible(aged female 65 )0.202Medicaid eligible(aged female 65 )0.202No Type 2 diabetescodedNo vascular diseasecodedChronic diastolic(congestive) heartfailure not codedNo Disease InteractionTotal RAFXXType 2Diabetes w/ocomplications E11.9 (HCC19)Vascular disease w/ocomplicationsPVD, unspecifiedI73.9(HCC 108)0.118Type 2 Diabetes with diabeticperipheral angiopathy w/o gangrene0.368E11.51 (HCC 18)0.299Vascular disease w/ Atherosclerosis ofnative arteries of left leg with ulcerationof ankle1.143I70.243(HCC 106)XChronic diastolic(congestive) heart failurenot codedXChronic diastolic (congestive) heartfailure I50.32 (HCC 85)0.368XNo Disease InteractionXDisease Interaction(DM CHF)0.1821.057Total RAF2.0891.963 8210.628Total RAFTotal RAF, With FFSNormalization1 &CodingIntensity Adj20.590Total RAF, With FFSNormalization1 & CodingIntensityAdj20.993Total RAF, With FFSNormalization1 & Coding IntensityAdj2Estimated AverageCounty Rate 821Estimated Average CountyRate 821Estimated Average County RateEstimated DollarsPMPM 484Estimated Dollars PMPM 815Estimated Dollars PM 1,611Estimated DollarsPMPY 5,812Estimated Dollars PMPY 9,782Estimated Dollars PMPY 19,33313
ICD-10-CM Official Guidelines forCoding & Reporting Code all documented conditions that coexist at thetime of the encounter/visit, and require or affectpatient care, treatment or management Do not code conditions that were previously treatedand no longer exist However, history codes (Z codes) may be used assecondary codes if the historical condition or familyhistory has an impact on current care or influencestreatment14
Why is complete documentationimportant? B19.20 Hepatitis C, unspecified (No HCC) B17.10 Hepatitis C, acute (No HCC) B18.2 Hepatitis C, chronic (HCC-29)15
Why is complete documentationimportant? If the patient is actively receiving medication forcancer treatment (AHA Coding Clinic 10/2008).Assign the following codes:Active cancer code e.g. breast cancer C50.919Long-term (current) use of medications Z79.81 History of code should only be assigned if thedrug is being used prophylactically.16
Where’s the M.E.A.TA diagnosis willnot pass a RADVaudit without theM.E.A.T17
The Road to Success Starts and Endswith M.E.A.T. A variety of downfalls beset Providers and MAplans when confronted with a RADV audit Simply listing a diagnosis in the medical recordwithout M.E.A.T. will not support a reportableHCC code and is unacceptable Remember when the Provider follows theM.E.A.T. guidelines the documentation isbasically audit-proof18
Definition of M.E.A.T. Monitor—signs, symptoms, diseaseprogression, disease regression Evaluate—test results, medicationeffectiveness, response to treatment Assess/Address—ordering tests, discussion,review records, counseling Treat—medications, therapies, othermodalities19
Example M.E.A.T. Monitor: B/P reading 120/80; HgbA1c 5.5; lastlipid panel was within normal limits Evaluate: stump well healed, ostomy site w/oinfection appears clean & dry Address: stable; controlled, worsening;unchanged, uncontrolled Treatment: taking Fosamax for osteoporosis;taking tamoxifen for breast cancer “treatment”,DM controlled on insulin20
Why Would You Fail a RADV Audit? Failure to ensure the diagnosis codes beingbilled and the medical record documentationmatch Failure to document according to the M.E.A.T.principles (i.e. monitor, evaluate, addressed,and/or treatment Failure to link the causal relationship formanifestation codes21
Key to Success At the end of the day, providing timely andaccurate documentation and submitting HCCcodes allows proper reimbursement Accurate documentation and coding allows theplans to provide better benefits to membersand improve premiums per member permonth (PMPM)22
ConclusionMRA supports achievement of “Triple Aim” Cost effective Care Quality Outcomes Patient Satisfaction23
Resources http://www.hcpro.com/content.cfm?content id 302031 https://www.cartoonstock.com/directory/c/cured ham.asp24
Evaluation & Management Services (E&M)Presenter:Thomasina L Young, CPC, CPCO, CPMA, CRC25
What are E & M Services A section of codes in the AMA CPT Manualthat are used to report the professional feeservices performed by physicians and otherqualified healthcare providers.The “bread andbutter” of manyprofessional feeservices
Why Is Documentation So Important? Supports the medical necessity of the service Reduces risk to audit exposure Supports billing services to payers Demonstrates the quality of care rendered Serves as a legal document in malpracticecases Provides continuity of care across disciplines
Outpatient E/M ServicesCPT CodeNewTimeHistoryExamMDM9920110Problem FocusedProblem FocusedStraightforward9920220ExpandedProblem FocusedExpanded 560ComprehensiveComprehensiveHighCPT CodeEstablishedTimeHistoryExamMDM9921210Problem FocusedProblem FocusedStraightforward9921315ExpandedProblem FocusedExpanded 21540ComprehensiveComprehensiveHigh
Inpatient Hospital E/M ServicesCPT CodeInitialTimeHistoryExamMDM9922130Detailed orComprehensiveDetailed ehensiveHigh9923115ProblemFocusedProblem equent29
Observation E/M ServicesCPT CodeInitialTimeHistoryExamMDM9921830Detailed orComprehensiveDetailed FocusedProblem blemFocusedModerate9922635DetailedDetailedHigh30
ConsultationsMedical Record Documentation requirements: Request for consultation Rendering of consultant’s opinion Report sent back to the requesting physicianExample: I saw this patient in consultation at the request of Dr.31
CMS Preventive VisitsThere are 3 types of “wellness visits/preventivevisits”, each has different reportingrequirements.Initial Preventive Physical Examination (IPPE)Initial Medicare Annual Wellness Visit (AWV)Subsequent AWV
Care Management Services99487: Complex chronic care management 60minutes of clinical staff time99489: Complex chronic care management EACHadditional 30 minutes of clinical staff time99490: Chronic care management service at least 20minutes of clinical staff time99495: Transitional care management (TCM)moderate complexity; face-to-face within 14 days99496: Transitional care management highcomplexity; face-to-face within 7 days33
Medical Necessity Medicare defines "medical necessity" asservices or items reasonable and necessaryfor the diagnosis or treatment of illness orinjury or to improve the functioning of amalformed body member Medical necessity of a service is theoverarching criterion for payment in additionto the individual requirements of a CPT code34
Components of Medical NecessityMedical necessity cannot be quantified using a points system.Determining the medically necessary LOS is multi-factorial and isnot the same from patient to patient and day to day. Medicalnecessity is determined through a culmination of factors, including,but not limited to: Clinical judgment Standards of practice Why patient needs to be seen (chief complaint) Any acute exacerbations/onsets of medical conditions orinjuries Stability/acuity of patient Multiple medical co-morbidities Management of patient for that specific DOS35
Medical Necessity Criteria Consistent with the symptoms and diagnoses ortreatment of the patient’s condition, illness,disease or injury In accordance with accepted professionalmedical standards Not primarily for the convenience of the patientor provider Furnished at the most appropriate level that canbe safely provided to the patient36
Evaluation & Management (E/M)E/M services recognize 7 components which areused in defining the levels of E/M servicesKey Components History Examination Medical Decision MakingContributory Components Counseling Coordination of care Nature of presenting problem Time37
Chief Complaint (CC) The CC is a concise statement describing thesymptom, problem, condition, diagnosis,physician recommended return, or other factorthat is the reason for the encounter Is required for every E&M service If there is no chief complaint, the service can bedeemed not billable.38
History of Present illness (HPI)A chronological description of the development of thepatient's present illness with elements of:39
Past Medical, Family, Social History Past Medical history (the patient's past experiences withillnesses, operations, injuries and treatments). ForInfants/newborns may include mother’s pregnancy andthe birth of the child Family history - a review of medical events in thepatient's family, including diseases which may behereditary or place the patient at risk) Social history - an age appropriate review of past andcurrent activities, i.e., Military Status, livingarrangements and education40
Review of Systems (ROS)14 Systems Are RecognizedThree types of ROS:1. Problem Pertinent – inquires about organsystem directly related to the presentingproblem2. Extended – inquires about 2-9 organ systems3. Complete – Requires documentation of at least10 organs systems individually OR somepertinent /- of some organs systems with astatement “all other systems were reviewedand are negative”41
Examination GuidelinesExam omprehensive1995 & 1997 92231995 BodyAreas/OrganSystemsAffected area2 – 4 bodyarea/organsystems5 - 7 bodyareas/organsystems8 organ systems19971 - 5 bulletsin 1 systems/areas6 - 11 bulletsin 1 system/areas12 bulletsin 2 systems/areas2 bulletsfor each of 9 systems/areas42
Medical Decision Making (MDM)There are 4 levels of MDM:1. Straightforward3. Moderate2. Low4. HighMDM is:A. The number of diagnoses or management optionsB. Amount and/or complexity of data to be reviewedC. Risk of complications and/or morbidity ormortality43
OBSERVATION SERVICES (OBS) There must be a physician’s order specifying “Placementfor Observation” or simply “Observation” including thereason and medical necessity for OBS care A physician order for observation services should NOTread “Admit to (or for) Observation” All OBS services must be ordered by a physician OBS starts at the documented time that observation careis initiated All other physicians who furnish evaluations or serviceswhile the patient is receiving OBS must bill theappropriate outpatient service codes44
Teaching Physician (TP) GuidelinesThe Teaching Physician must personally document:That they performed theservice or werephysically present duringthe critical or keyportions of the servicefurnished by theresident; andHis or her participationin the management ofthe patientDocumentation bythe resident of thepresence andparticipation ofthe TP is NOTsufficient45
Medical Students TP can only use the ROS and PFSH from a MedicalStudents documentation TP MUST re-document the HPI, Exam and MDM TP MUST be present during the entire encounter46
Medicare Administrative Contractors (MACs)Banner Health is located in seven states:Arizona – Corporate aNevada47
Variances EncounteredMAC’s Noridian Novitas WPSAreas Review of Systems Exam PFSH Medical decisionmaking (MDM)
Copy/Paste/Cloning/Carry ForwardThe documentation may be worded: Exactly the same as another DOS Similar to a previous DOS The same for all patientsCloned documentation methods include: Templates Handwritten EHR
Medical Record Cloning Cloned documentation may be handwritten, but generallyoccurs when using a preprinted template or an ElectronicHealth Record (EHR). While these methods of documentingare acceptable, it would not be expected the same patient hadthe same exact problem, symptoms, and required the exactsame treatment or the same patient had the sameproblem/situation on every encounter Cloned documentation does not meet medical necessityrequirements for coverage of services. Identification of this type of documentation will lead to denialof services for lack of medical necessity and recoupment of alloverpayments made50
Common Errors Insufficient DocumentationIncorrect CodingMedical Necessity Not SupportedDocumentation Doesn’t Support Level BilledProlonged ServicesTime-based ServicesDuplicate submissionsOther Issues51
Documentation Doesn’t Support Level Billed Each encounter must tell a complete story Prior encounters cannot be considered unlessreferenced by date in the encounter being audited All three components (history, exam and medicaldecision making) must be present when billinginitial/new patient visits52
Documentation Doesn’t Support Level Billed Should be able to find a correlation between chiefcomplaint/HPI/exam findings and what isdocumented for medical decision making It would not be medically necessary or appropriate tobill a higher level E/M when a lower level of service iswarranted53
CERT Findings Improper Payments54
Key Points to Remember Professional fee service and facility fee servicesare reported differently but support the totalcare rendered to patients Providers should have ongoing CDI educationand taught how to “think in ink” Coders should have ongoing education and giventhe tools necessary to ensure their success
WHAT’S NEW FOR 201756
UPCOMING UPDATESGlobal periods: Instituting GXXX global period codes for data gathering; timebased 10 min; based on complexity of the visit; by settinginpt/outptNew Codes for Telehealth: Critical Care – G Codes; 1 per day;Complex Chronic Care Management Services 99497/99498 Payable 1/12017BHI CoCOM –Psychiatric Collaborative Care Model G codes for initial and subsequent; all are time based57
SPECIFICITYEach health care encounter shouldbe coded to the level of certaintyknown for that encounterNOTE: Check with commercial payers regarding reporting unspecifiedICD-10-CM58
The End of Grace PeriodOctober 1st, 2016 will mark the end of a 1-year graceperiod that Centers for Medicare and Medicaid Services(CMS) established for the ICD-10-CM diagnosis codes. CMSwill no longer accept unspecified ICD-10-CM codes onMedicare fee-for-service (FFS) claims when a specific one iswarranted by the medical record. Avoid unspecified ICD-10-CM codes wheneverdocumentation supports a more detailed code. Checkthe coding on each claim to make sure that it aligns withthe clinical documentation.59
Unspecified Codes Rheumatoid Arthritiso Juvenile, seronegative, seropositive, siteCrohn’s diseaseo Enteritis, regional: colon, duodenum, ileum, jejunum, largebowel, intestineUlcerative Colitiso Enterocolitis, ileocolitis, proctitis, pseudopolyposis,psychogenic, rectosigmoiditis, complicationsAsthmao Intermittent (mild)Exacerbation or status asthmaticuso Persistent: mild, moderate, severeExacerbation or status asthmaticus60
Unspecified Codes Osteoporosiso Age related, disuse, drug-induced, idiopathic, involutional ,localized, postmenopausal, post-traumatic, senile, etcOsteopeniao Site: ankle, foot, forearm, hand, leg, rib, shoulder, etcLung CAo Type: primary, secondary, benign, in-situ, malignant,o Laterality: right, left, bilateral, upper, lower, middle lobeBreast CAo Type: primary, secondary, benign, in-situ, malignant,o Laterality: right, left, bilateral, lower, upper, inner, outer61
ReferencesCMS Claims Processing Manual; Chapter 12; sec 30.6.1; pgs. 40-41CMS 1995 & 1997 Examination GuidelinesBH Pol 12411;Incident ToBH Position Statement: Review of Systems; Formal P&P upcomingBH Position Statement “Physician Practices/Clinics: Assistant at Surgery, Co-Surgery, Team Surgery.”BH Policy #678BMG Compliance Newsletter June 2012 “Cloning of Medical Notes”CMS IOM 100-04, Chp.12, Section ce/Guidance/Manuals/Downloads/clm104c12.pdfNovitas Web Article, “Split/Shared shared-em.htmlWPS Web Article, “Inpatient Split/Shared/E./M ment/medicalreview/20091116em.shtml AMA CPT Manual 2016 Federal ml?redirect s-what-end-icd-10-flexibilities-means62
COPD, CVD and CAD RF and CHF RF, CHF and DM 12. Low level of specificity Moderate level of specificity High level of specificity 76 year old female 0.426 76 year old female 0.426 76 year old female 0.426 Medicaid eligible (aged female 65 ) 0.202 Me