Transcription
Chemical Pathology Lecture Notes2013University of Cape TownPrefaceThis manuscript constitutes a series of lecture notes prepared and updated by members of theDivision of Chemical Pathology at UCT. These notes are intended to provide a clear and concisereference of the basic biochemical principles and clinical application of the field of ChemicalPathology/Clinical Biochemistry. These lectures have been developed specifically for undergraduatemedical student teaching.Included in lectures 1 -11, 14, 18, 20, 22- 25 and 27 are a series of related questions and answersthat can be used as an excellent tool to test knowledge and provide insight into a wide range of clinicalproblems. In this the 2012 edition, lectures 1, 3, 10, 16, 26 and 29 have been completely revised inkeeping with continouous developments in the fieldThese lectures are published under Creative Commons Copyright(Attribution-Non Commercial-Share alike -2.5-South Africa) and may be reproduced for teaching purposes in this exact formatprovided they are not distributed for profit and that all original authors are acknowledgedExperts in the field who may find this resource useful are invited to contribute corrections, submitrevisions of lectures or submit new lectures on relevant topics. In this way it is hoped that this work willimprove and remain current as teaching tool.George van der WattDivision of Chemical PathologyUniversity of Cape Town.Contact:e-mail: George.vanderwatt@uct.ac.za
Table of ContentsTable of Contents .1Lecture 1: Introductory Lecture And Basic Statistics. .3Lecture 2: Acid-Base Balance .16Lecture 3: Disorders Of Renal Function .42Lecture 4: Disorders Of Water And Sodium Balance .59Lecture 5: Disorders Of Potassium Metabolism .72Lecture 6: Carbohydrate Metabolsim And Diabetes .82Lecture 7: Calcium, Magnesium And Phosphate Metabolism.112Lecture 8: Iron Metabolism .133Lecture 9: Lipid And Lipoprotein Metabolism And Dyslipidaemias .150Lecture 10: Obesity .175Lecture 11: Biochemistry Of Alcohol Abuse .185Lecture 12: Disorders Of Protein Metabolism .194Lecture 13: Cerebrospinal Fluid .217Lecture 14: Chemical Pathology Of Liver Disease .223Lecture 15: Enzymology.247Lecture 16: Chemical Pathology Of The Gastro-Intestinal Tract .256Lecture 17: Endocrinology 1: Pituitary And Hypothalamus .269Lecture 18: Endocrinology 2: Pituitary Diseases .273Lecture 19: Endocrinology 3: Adrenal Diseases .284Lecture 20: Endocrinology 4: Adrenal Dysfunction: Hypercortisolism And Hyperaldosteronism .291Lecture 21: Endocrinology 5: Hypoadrenalsim And Congenital Adrenal Hyperplasia .300Lecture 22: Endocrinology 6: Thyroid .306Lecture 23: Endocrinology 7: Disorders Of Gonadal Function .314Lecture 24: Vitamins .324Lecture 25: Uric Acid And Gout .340Lecture 26: Inherited Metabolic Diseases .349Lecture 27- Disorders Of Porphyrin Metabolism .367Lecture 28: Tumour Markers .379Lecture 29: Pregnancy And Parental Screening .3912
Lecture 1: Introductory Lecture And Basic StatisticsPROF E HARLEY, UPDATED Dr D HAARBURGER 2011WHAT IS CHEMICAL PATHOLOGY?Pathology is the scientific study of the cause, origin, and nature of disease, including the changes occurringas a result of disease. Chemical Pathology (also known as Clinical Biochemistry or Clinical Chemistry) is thebranch of pathology concerned with the biochemical basis of disease, and the application of biochemical andmolecular techniques in diagnosis. An allied subspecialty of Chemical Pathology is Metabolic Medicine whichdeals with metabolic disease in all its manifestations. The Division of Chemical Pathology at the University ofCape Town is involved in teaching at undergraduate and postgraduate levels and provides diagnosticlaboratory services for Groote Schuur Hospital.An understanding of the biochemical mechanisms of disease states has provided modern medicine with arational basis for diagnosis and therapy. The course will equip you with the conceptual tools you will require tounderstand the meaning and interpretation of diagnostic tests, as well as introducing new advances inmolecular aspects of medicine. Chemical Pathology is a logical, scientific subject, and is at the interfacebetween the practice of medicine and cutting-edge scientific developments. NB: More than 75% of medicaldiagnoses require the services of the laboratory.WHAT IS THE ROLE OF CHEMICAL PATHOLOGY IN HEALTH CARE?Chemical Pathology is the branch of pathology dealing with the biochemical basis of disease and the use ofbiochemical tests for diagnosis and management. Doctors in the specialty have dual responsibilities. Firstthere is the provision of a reliable analytical service, for example measuring serum electrolytes, indices ofliver function, hormones, drugs and tumour markers in hundreds of patient samples every day. Many of theseanalyses are performed on automated analysers, usually operated by technologists, but the management ofthe process (and the staff), assurance of quality and provision of guidance on the selection of tests andassessment of the significance of the results (particularly with some of the less generally familiar tests) arethe province of the chemical pathologist.Secondly, Chemical Pathologists have an important clinical role, not only advising on the management ofpatients with metabolic disturbances but in several countries now, they are increasingly having directresponsibility for such patients in out-patient clinics and on the wards.Chemical Pathology not only brings together science and medicine, it relates to all the medical specialities.Chemical Pathologists are frequently consulted about further investigation or management of patients foundto have biochemical abnormalities on 'routine' testing. They frequently have to deal with investigating patientswith dyslipidaemias, diabetes and hypertension, review ward patients receiving artificial nutrition, discuss theintroduction of a new diagnostic test with consultant colleagues, review the quality of the laboratory'sanalytical service and manage research projects of trainees. (Adapted from Dr William Marshall.)Under application of biochemical techniques can be listed the following: Diagnosis: tests can be used to help differentiate between various possibilities in the differentialdiagnosis based on the initial history and examination when the patient first presents. Screening: detection of disease before it is clinically evident, e.g. testing all infants at birth for aspecific inherited disease (phenylketonuria, thyroid deficiency) Monitoring: following the progression of disease processes, checking against adverse drug effects(e.g. hypokalaemia with diuretic therapy), or response to therapy (glucose levels in diabetes mellitus). Prognosis: providing information on disease susceptibility, e.g. cholesterol to predict heart disease.MEASUREMENTS IN CHEMICAL PATHOLOGY: concentration of a substanceThere are 2 types of units of concentration, molar units, and mass units. The former is preferable, since it isa better comparative descriptor of the concentration of a substance, but unfortunately many countries stillcling to the older mass units, usually grams/100 ml, and it is often necessary to convert.One mole of a compound corresponds to a mass (in grams) equal to the molecular weight of that compound,3
e.g. 1 mole of NaCl (23 35) 58 grams of the saltor, 1mole/liter (mol/l) of NaCl 58 g/l or 5.8 g/100mlAbbreviations:1 mol/l 1 M 1 molar-31 mmol/l 1 mM 1 millimolar 10 M1 µmol/l 1 µM 1 micromolar 10 M-6-91 nM 1 nanomolar 10 M1 pM 1 picomolar 10-12MConcentrations of some analytes (to demonstrate the range of concentrations in clinical chemistry) 140 mMserum glucose8 mM2 1 mMserum albumin0.6 mM3 20 µMserum cortisol500 nM 40 nMplasma ACTH50 pMserum Naserum Mgserum Feserum [H ]METHODS USED IN THE CHEMICAL PATHOLOGY LABORATORY Colorimetric methods:Analyte reacts with a dye, changing its absorption spectrum (colour).Measured with a spectrophotometer. Rapid & easily automated. Cheap. Concentration range:2 mM to µM. Examples: urea, creatinine, phosphate, albumin, total Ca Ion-selective electrodes:Membrane selectively permeable to an ion generates a membranepotential proportional to concentration of free ion. Rapid & easily automated. Cheap.Concentration range: mM to nM 2 Examples: Na , H (pH meter), free Ca Enzymatic:Example: lactate dehydrogenase (LDH) catalyses the reaction lactate NADpyruvate NADH HThe concentration of NADH is easily measurable by its UV absorbance, allowing the rate of thereaction to be measured. An end-point method can be used to measure the concentration of asubstrate (e.g. the amount of NADH formed will be equal to the initial lactate concentration) or arate method can measure the amount of enzyme. Immunoassays and related techniques:In the competitive immunoassay, the analyte orantigen (Ag) in the sample competes with a labelled analyte (Ag*) for binding to a limiting numberof antibody sites (Ab) in the test tube:Ag* Ab Ag* - Ab(we measure THIS by means of the radio-label) Ag (unknown amount in patient's plasma.)(the more of this, the less Ag*-Ab is formed) Ag-AbThe antigen-antibody complex (Ag*–Ab) can be easily separated from the free Ag*, and theamount of labelled Ag* bound is measured. The more unlabelled Ag in the specimen, the less4
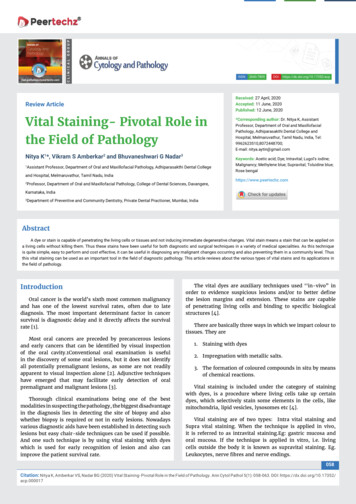
Ag* will be bound . The technique has high sensitivity i.e. is able to measure low concentrationsof Ag ( nM to pM range). Automation has been achieved with some but not all immunoassays incurrent use, so it can be a time-consuming method.Immunoassays can be characterised according to their label. Common types of immunoassaysare radioassays (using radio-labels), enzyme-assays (where enzyme activity is measured) andchemiluminescent assays (where light is measured). Chromatographic methodsElectrophoresis and other chromatographic methods can be used to separate compoundsbased on their physical and chemical properties, e.g.- serum proteins (electrophoresis)- amino acids (ion exchange chromatography)- organic acids (gas chromatography, mass spectrometry)- isoenzymes (electrophoresis) DNA techniquesAnalysis of patient’s DNA for specific mutations, or linked polymorphisms, by molecularbiological techniques, usually involving use of the versatile polymerase chain reaction (PCR)BASIC STATISTICSStatistics is the science of collecting and analysing data. This collected data can then be used to makepredications about the population from where the data came. Various parameters can be used to describethe data:Mean: Also called average is a measure of central tendency of the data. The mean is defined as the sum ofall the observations dived by the number of observation.Variance: This is a measure of the dispersion of the data. A small variance implies all the data is close tothe mean, whereas a large variation implies the opposite. To calculate the variance, each observation issubtracted from the mean and then squared. The average of these squares is the variance.Standard deviation: This is the square root of the variance. The standard deviation has the advantage ofhaving the same units as the original data.Coefficient of variation (CV): This is the standard deviation divided by the mean, usually expressed as apercentage. The CV is a dimensionless (unitless) number which is useful for comparing differentpopulations.PRECISION AND ACCURACY IN BIOCHEMICAL TESTSPrecision: The amount of variation in results after measuring the same sample repeatedly.Accuracy: How close the result is to the "true" value as determined by a reference method.Figure 1.In figure 1 above, both graphs show the distribution of results for repeated analysis of the same sample bydifferent methods. Methods A and B on the left are equally accurate (mean value is the same) but the lesser5
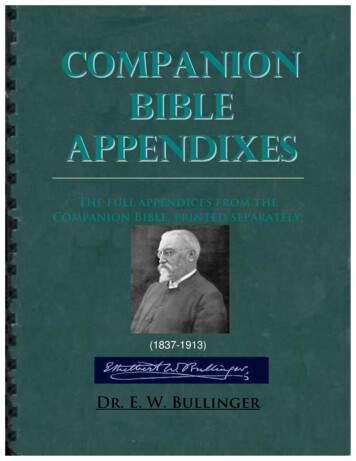
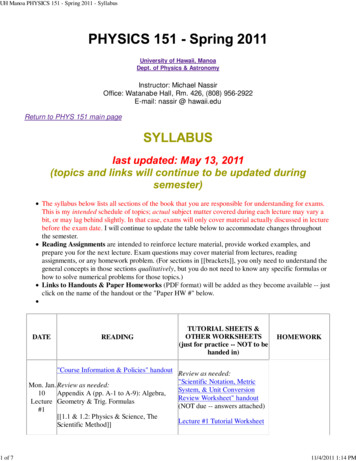
scatter in A makes it more precise. C and D on the right are equally precise, but in D the mean value differsfrom the true, so C is more accurate.MEANING OF NORMAL AND REFERENCE RANGESIf an analyte is measured in a large number of normal (healthy) individuals and the distribution of the testresults are plotted as in Fig 2, many substances show a Gaussian (or "normal") distribution, depicted here.The problem with such a distribution is that a few, clinically normal (note different usage of the word"normal"), individuals have values much higher or lower than the mean. So when can a result be taken ashaving clinical significance such that the clinician can suspect pathology? By convention it is when the resultis outside the range given by 95% of clinically normal individuals, which corresponds to 2 standard deviations(2SDs) away from the mean. Although not ideal, since by definition 5% of normal individuals have resultsoutside this range, it is the most practical solution to the dilemma, and this range is usually termed theReference range; (the term "Normal" range is often used interchangeably in a clinical context, but is notstrictly statistically accurate).Figure 2If we were now to compare the analyte levels in a healthy (H) population with a population having somedisease (D) causing elevated levels of the analyte, and which would therefore be diagnostically useful, wemight find distributions such as shown in Fig 3. Note the problematical area of overlap. A normal individualwho chances to have a value falling in the H3 region is in danger of being marked as having the disease(which can be a major practical problem in insurance examinations). This is termed a false positive (FP)result. Alternatively a person with the disease ( but perhaps not manifesting it obviously clinically yet) mightchance to have a value in the area shown by D2, in which case he or she could be misclassified as nothaving the disease (false negative result, FN). The H1 area corresponds to true negative (TN) and D1 to truepositive (TP).If one is particularly concerned about not missing genuine cases of the disease (as in screening new-bornsfor an inherited disease) then one could adjust the reference range to the left until all the D2 region isincluded. This increases the sensitivity of the test, but at the cost of increasing the number of normalindividuals (false positives) who would then appear to have the disease. This would decrease the specificityof the test, specificity being defined as the incidence of negative results in persons known to be free of thedisease. Alternatively if one is concerned more with not labelling individuals who are healthy as having thedisease (as from the patient's point of view in an insurance examination), then moving the upper end of thereference range to the right of the H3 region would seem appropriate. However, by thus increasing thespecificity (no false positives) more patients with the disease will now be missed (many false negatives). Itmay therefore be seen that a reference range right for some circumstances may not be appropriate foranother. It is unfortunately seldom that the two distributions (D & H) have no overlap, when there would be100% sensitivity and 100% specificity, and no problems would arise. The ideal test is accurate, precise,sensitive, specific, cheap, simple to perform, and gives results quickly. These ideals are seldom, if ever, fullymet by any test, and the decision as to which method to employ in a laboratory becomes a complex functionof these sometimes conflicting requirements.For reference, sensitivity (the ability of a test to detect a disease when it is present), and specificity (the abilityof a test to reflect the absence of the disease in those disease-free) can be calculated as follows:Sensitivity TN / (TN FP) 100%6
Specificity TP / (TP FN) 100%There is one other statistic which can be useful in deciding either what test to use in a particular context(screening, confirmation etc), or what reference range to apply in such a context, and that is the predictivevalue (PV) of a test, which can be positive or negative. The PV for a positive result is dependent on theprevalence of the disease, and is the percentage of all positive results which are true positives, e.g.PV( ) TP/(TP FP) 100%If the test is less than 100% specific and the condition has a low prevalence (such as an inherited metabolicdisease), then many FPs will result. A high predictive value is important if the (unnecessary) treatment of afalse positive had significant dangerous consequences or side effects.The PV for a negative result is the percentage of negative results which are true negatives. This should bemaximised if one does not want to miss a patient who has the disease, it being the proportion of all negativeresults which are true negatives. It is given byPV(-) TN/(TN FN) 100%To maximise the PV(-) test should have a high sensitivity.SPECIMEN HANDLING IN CHEMICAL PATHOLOGYIf the physician is to have confidence that the laboratory result is correct and meaningful, he/she needs toensure that the specimen is taken in an appropriate way and that it gets to the laboratory in optimumcondition and in good time. As an old saying goes: "There is many a slip 'twixt the cup and the lip"Blood and additives:Anti-coagulated Blood (centrifuged)Clotted blood (centrifuged)otherwise same as plasma). cells plasma(cells clot) serum (lacks fibrinogen & some clotting factors,Anticoagulants:Heparin - inhibits clotting factor action2 Ca chelators: - EDTA, citrate, oxalate. Chelators bind to and remove free Caclotting factor activation.2 which is required forAll these anticoagulants are anions which are added as their Na , K or Li salts - these samples aretherefore NOT suitable for measurement of Na , K or Li , so serum should be used for these electrolytes.Fluoride tube is used for blood glucose measurement as it inhibits glycolysis. A blood sample taken withoutthis inhibitor will continue to metabolise the glucose giving a lower glucose level than it should (the samplewould also resemble one from a patient with lactate acidosis, red cells metabolising glucose to lactate)Urine additives: Random or 24-hour urine collections usually need a special bottle containing the correctadditive. Azide or toluene are often used to prevent bacterial growth. For urine Ca2 , Mg2 and phosphate(Pi) the bottle must contain acid (HCl) since Ca2 and Mg2 form an insoluble precipitate with Pi at alkalinepH. For urate, the urine needs to be alkalinised because URATE is much more soluble than URIC ACID.7
Contamination1. In the patient. Taking blood from a vein where the patient has a drip installed peripherally can give verystrange results ("drip arm").2. In the tube (wrong additive)Separation of red cells from serum/plasmaFor most tests delay of a few hours does not matter. After a 12 h delay the specimen is classified as a "non separated specimen" (NSS). NSS typically shows false high K , Pi and LDH (leakage from RBCs).Haemolysis - produces much the same changes as NSS and in addition haemoglobin is released. A clue tothis is where serum remains red after the blood is spun.Labile analytesSpecial precautions have to be taken when measuring labile constituents. EXAMPLES:Blood gases : blood has to be taken anaerobically and into a stoppered tube (to prevent CO2 escaping) andplaced on ice to prevent lactic acid production.Q: What acid/base disturbances would appear to result if these precautions are not followed?Peptide hormones are susceptible to protease degradation, and require addition of protease inhibitors.Plasma ammonia rapidly rises after sampling due to breakdown of glutamine.Other factors which can influence the value of an analyte and may need to be taken into account inthe interpretation of results are the following:FactorExample AgeAlkaline phosphatase - elevated in growing children GenderLevels of sex hormones, also uric acid. PregnancyHormone levels, glucose. PostureAlbumin - probably the reason why most (recumbent) hospital patients have low albuminvalues ExerciseCreatine kinase FastingGlucose levels may be elevated if not fasting. Time of day Cortisol.REFERENCE RANGES OF ANALYTES WHICH ARE FREQUENTLY ENCOUNTERED AND THEREFOREUSEFUL TO MEMORIZEACID-BASEANALYTEREFERNCERANGEpH7,36 - 7,44pCO24,5 - 6.1kPaStd. Bicarbonate22mmol/lBase excess-2,5 to 2,5mmol/lpO210,0 - 16,0kPa8- 26UNIT
SODIUM135 - 145mmol/lPOTASSIUM3,5 - 5,0mmol/l97 - 107mmol/l2,1 - 2,6mmol/lUREA1-6mmol/lCREATININE5 - 115µmol/lSERUM OSMOLALITY275 - 297mol/kgGLUCOSE (fasting)3,9 - 6,1mmol/lCHLORIDECALCIUMRESULT VARIATIONIf you were to take a sample from a person now and measure a particular analyte, and then take a newsample from that same person some time later and re-measure that analyte, it would be highly unlikely thatyou would get the same result. In fact, every time you repeated this procedure, you would get a slightlydifferent result. For example, if you were to measure a person’s serum cholesterol weekly, you would not getone result, but a range of results. In fact, if you took enough results, the results would most likely form anormal distribution. The reason that you do not get the same result every time is because there are variousfactors which cause variation of the result. These include biological variation, pre- and post-analyticalvariation and analytical variation. Pre-analytical variation is variation that occurs between samples beforethe sample is analysed. Examples included differences in patient preparation, phlebotomy techniques,specimen storage and specimen transport. Analytical variation is the variation that occurs while measuringthe analyte. Examples include differences in pipetting volumes, differences in reagent concentrations anddifferences in calibration curves. Post-analytical variation is variation that occurs after the analyte has beenmeasured and comprises differences in reporting and interpretation of results. Biological variation is thebiggest source of variation in laboratory results. This variation is due to fluxes in homeostasis and isinfluenced by factors such as diet, activity level and time (of day, month or year).When interpreting serial results from a single patient, it is important to take all this variation into account. It iscrucial to know whether a change in two serial results represent a ‘real’ difference or merely expectedvariation.Example: If someone has a cholesterol level measured and the result 6.6 mmol/l and then has a levelmeasured 3 months later and the level is 5.82 mmol/l, has the level changed? How do we determine this?We need to examine all the possible causes of variation in these results. The (intraindividual) biological CVhas been determined for many analytes and are publicly available. For cholesterol, the published value (CVI)is 6.0%. The analytical variation (CVA) is also known. Typically, it will be 1.6% for cholesterol. Note that thiswill differ from laboratory to laboratory. We will assume that the pre- and post-analytical variations arenegligible. The total variation can be calculated as follows:If we want to be 95% confident of a change then we need 2 CVT 2 6.2% 12.4% 0.82 mmol/lThe difference is 0.78 mmol/l which is less than 0.82 mmol/lThis means that there has not been a significant change in the result!!!It is becoming increasingly important for laboratories to publish values for analytes derived from the CVs suchthat accurate decisions can be made by clinicians as to whether there has been a significant change in theresults.9
SMALL GROUP TEACHING. LECTURE 1- INTRODUCTION TO CHEMICAL PATHOLOGY: QUESTIONSCONVERSION OF UNITSIn order to interconvert between MOLAR and MASS units all that is needed is the molecular weight (MW) ofthe compound. Remember the essential relationship:1 mol of a compound has a mass of MW g therefore1 mol/l MW g/l and 1 mmol/l MW mg/l and 1 µmol/l MW µg/letc., etc.Abbreviations:1 mol/l 1 molar 1 M, 1 mmol/l 1 millimolar 1 mM, 1 µmol/l 1 micromolar 1 µM etc.The expression "g %" ("grams percent") means g per 100 ml.EXAMPLES:1. Convert a serum cortisol value of 500 nmol/l into µg/ml, given that MW of cortisol is 320500 nmol/l 500 x MW ng/l 500 x 320 ng/l 160000 ng/l 160 ng/ml 0.16 µg/ml2. Convert a plasma glucose level of 36 mg/dl to molar units. The MW of glucose is 180.36 mg/dl 360 mg/l 360/MW mmol/l 360/180 mmol/l 2 mmol/lEXERCISES:1. Convert a serum iron level of 112 µg/dl to µmol/l. The MW of iron is 56.2. The reference range for serum testosterone in adult males is 10 - 35 nmol/l. Convert this to ng/mlgiven that the MW of testoterone is 300.3. 3. A patient's urine has a Ca2 concentration of 80 mg/dl. What is this in mmoles/l, given that theMW of Ca2 is 40?.4. 4. An average "western" diet has a salt intake of about 150 mmol/day. How much NaCl is this ingrams? (MW of NaCl 58).BASIC STATISTCSMean:x ( x1 x2 . xn ) / Nwhere x1, x2 etc are the instances from N observationsStandard deviation (SD)For an analysis on a whole population :SD (x x)2iNFor an analysis on a sample of a population:SD (x x)i2( N 1)Standard error of the mean (SEM):SEM SD / N note: the SEM gets smaller if the number. of observations increases.10
Coefficient of variation (CV):CV (SD / x ) 100%i.e. the CV is simply the SD expressed as a % of the mean.If a parameter is normally distributed, then*approx. 95% of values fall within 2 SD of the mean*2.5% exceed the mean by more than 2SD*2.5% are less than the mean by more than 2SD*approx. 66% of values fall within 1 SD of the mean.EXERCISES:5. Two groups of people, group A (5 people) and group B (10 people), had blood taken for serum ironmeasurement. The results (in µmol/l) were as follows:A2015221927B22271920221515272019Calculate for each group (a) the mean serum iron level (b) the standard deviation (SD) (assumewhole population, i.e. use N, not N-1) and (c) the standard error of the mean (SEM). Then combinethe groups into a single group (A B), and recalculate the mean, SD and SEM.ABA BmeanSDSEM6. Given these results, comment on the difference between SD and SEM as statistical parameters:7. In a population of 1 million, serum growth hormone levels were "normally" distributed (i.e. Gaussiandistribution), with a mean of 4.5 ng/ml and a SD of 1.2 ng/ml. How many individuals had a growthhormone level less than 2.1 ng/ml?8. Are these people normal?PRECISION AND ACCURACYTwo methods for the measurement of serum urate were evaluated.Method A: The sample is treated with compound X which reacts with urate (and structurally relatedsubstances) to produce a blue coloured compound. The change in absorbance in the bluewavelength range is then measured.The test is performed on an automated analyser.Method B: The sample is teated with uricase enzyme which converts urate to allantoin. Urateabsorbs in the UV whereas allantoin does not. The decrease in UV absorbance is measured. Theuricase is highly specific for urate as substrate. The test is manually performed.A single sample of serum was measured repeatedly by each method, with the following results (inmM):Method A - 0.54, 0.55, 0.54, 0.56, 0.55, 0.55, 0.55, 0.54Method B 0.45, 0.41, 0.40, 0.42, 0.46, 0.43, 0.40, 0.4411
9. Calculate the precision of each method, expressed as the coefficient of variation (CV).The same sample had a urate level of 0.43 mM measured by the inte
Chemical Pathology (also known as Clinical Biochemistry or Clinical Chemistry) is the branch of pathology concerned with the biochemical basis of disease, and the application of biochemical and molecular techniques in diagnosis. An allied subsp