Transcription
CHAPTER 15F425 - PHARMACY SERVICESTHE MEDICATION AUDIT TRAIL(ORDERING, RECEIVING ANDDISPOSITION OF MEDICATION)15.1
NURSING HOMETHE PRESCRIPTION AUDIT TRAILI. Regulatory OverviewSTATE59A-4.112 Florida Nursing Home Regulations involving Pharmacy Services1) The facility shall adopt procedures that assure the accurate acquiring, receiving, dispensing,and administering of all drugs and biologicals, to meet the needs of each resident.2) The consultant pharmacist shall establish a system to accurately record the receipt anddisposition of all controlled drugs in sufficient detail to enable an accurate reconciliation.3) The pharmacist shall determine that drug records are in order and that an account of allcontrolled drugs is maintained and periodically reconciled.4) All controlled substances shall be disposed of in accordance with State and federal laws.All non-controlled substances may be destroyed in accordance with the facility’s policiesand procedures. Records of the disposition of all substances shall be maintained insufficient detail to enable an accurate reconciliation.FEDERALF425 (Rev. 9/20/2006)§483.60 Pharmacy Services (Complete regulation available in Section II of this manual)The facility must provide routine and emergency drugs and biologicals to its residents, or obtainthem under an agreement described in §483.75(h) of this part. permits, but only under the generalsupervision of a licensed nurse.(a) Procedures. A facility must provide pharmaceutical services (including procedures thatassure the accurate acquiring, receiving, dispensing, and administering of all drugs andbiologicals) to meet the needs of each resident.(b) Service Consultation. The facility must employ or obtain the services of a licensed pharmacistwho-(1)Provides consultation on all aspects of the provision of pharmacy services inthe facility;(2) Establishes a system of records of receipt and disposition of all controlleddrugs in sufficient detail to enable an accurate reconciliation; and(3) Determines that drug records are in order and that an account of allcontrolled drugs is maintained and periodically reconciled.15.2
NURSING HOMEII. THE AUDIT TRAIL CONSISTS OF:1) Records that show when medications were ordered.a. Telephone Ordersb. Physician Orders (ex RX from outside prescriber)c. Refill order sheetsd. copies of faxes at the Pharmacye. Record Retention Requirements (BOP 64B16.28.140) has recently changed from2 years to 4 years (see page 15.11)2) Delivery of Medicationa. documentation should show which nurse received the medicationb. copies of delivery documents (i.e. delivery logs or delivery manifests) should beretained by the facility and the vendor Pharmacy3) Administration of MedicationDoses administered are recorded on the facility’s medical records forms including:a. the MAR (Medication Administration Record)b. the PRN Sheetc. the Treatment Sheet4) Disposition of Medicationa. Documentation showing drug was destroyed in the facility (non-controls can bedestroyed on the nursing unit)b. Documentation of controlled substances destruction showing disposition by theConsultant Pharmacist, the D.O.N. and the Administrator or their designeec. Documentation of medications released with a patient when they are dischargedd. Documentation of medications returned to the Pharmacy for credit.III. THE GOAL OF THE AUDIT TRAILThe audit trail should allow the Consultant Pharmacist to track a medication throughout theFacility.EX. 30 doses of Percocet ordered and delivered on 4/1/2012 by vendor pharmacyReceived by Nurse L. Smith LPN on 4/1/2012 3pmMAR indicates 15 doses were administered between 4/1/2012 and 4/20/2012 (perMAR)15 doses sent to the DON for destruction on 4/20/201215 doses actually destroyed by the Consultant Pharmacist on 5/30/2012audit shows all doses are accounted for15.3
NURSING HOMEMedication Orders in the Nursing Home1.Who can prescribe in the nursing home?Anyone who can prescribe in Florida can also prescribe in the nursing home2.Identify prescribers who are problematic in the nursing home?(1) Physician Assistants – Consultant must look at how P.A. orders are approved bytheir Physician(2) ARNP’s – prescribing or altering doses of controlled substance15.4
NURSING HOME3. What is the process for ordering medications for a new admission?a. Hospital transferb. Transfer from another facilityc. Transfer from resident’s home4. The use of Telephone Orders vs In-house Orders5. What is the process for transferring orders from Nursing to Pharmacy personnel?a. via phoneb. via fax6. Compare the new order process in the Nursing Home vs an ALF7. What makes an order “legal” in the nursing home?a. Specific Frequency (1 tab q4h)b. Route of administrationc. Duration of therapyd. PRN orders must have reason for use8. The standard of practice requires the primary physician for each resident to renew ordersevery 30 days.a. Physician Order Sheet – signed and dated every 30 days.Federal Indicators and state regulations do not require this process.9. No medications can be administered without an order15.5
NURSING HOMEFEDERAL PHYSICIAN REQUIREMENTSF333 – Prescriber’s Orders –The latest recapitulation of drug orders is sufficient for determining whether a validorder exists provided the prescriber has signed the “recap” The signed “recap”, if the facilityuses the “recap” system, and subsequent orders constitute a legal authorization to administerthe drug.F386 – Physician’s visits – The Physician must:1) review the resident’s total program of care, including medications and treatments,at each visit required by paragraph of this section;2) write, sign and date progress notes at each visit and3) sign and date all ordersUnder Guidance to surveyor: “There is no requirement for physician renewal oforders”F387 - Frequency of Physician visits1) The resident must be seen by a physician at least once every 30 days for the first 90 days afteradmission, and at least once every 60 days thereafter2) A physician visit is considered timely if it occurs not later than 10 days after the date the visitwas requiredF388 – At the option of the physician, required visits in SNF’s, after the initial visit, may alternatebetween personal visits by the physician and visits by a physician assistant, nurse practitioner orclinical nurse specialist in accordance with paragraph (e) of this section15.6
REVISED FLORIDA PHARMACY REGULATIONS64B16-27.1003 Transmission of Prescription Orders. Prescriptions may be transmitted from prescriber to dispenserin written form or by any means of communication. Prescriptions may be transmitted by facsimile systems as providedin Section 465.035, F.S., and federal law. Any direct transmission of prescriptions, including verbal, facsimile,telephonic or electronic data transmission, shall only be with the approval of the patient or patient’s agent. Thepharmacist receiving any such transmitted prescription shall not participate in any system that the pharmacist knows orshould have reason to know restricts the patient’s choice of pharmacy. The pharmacist shall take such measuresnecessary to ensure the validity of all prescriptions received. Specific Authority 465.005, 465.0155, 465.022 FS. LawImplemented 465.022, 465.026, 893.07 FS. History–New 11-18-07.64B16-27.103 Oral Prescriptions and Copies.(1) Only a pharmacist or registered pharmacy intern acting under the supervision of a pharmacist may, in the State ofFlorida, accept an oral prescription of any nature.(2) Only a pharmacist or registered pharmacy intern acting under the supervision of a pharmacist may, in the State ofFlorida, prepare a copy of a prescription or read a prescription to any person for purposes of providing referenceconcerning treatment of the person or animal for whom the prescription was written, and when said copy is given anotation shall be made upon the prescription that a copy has been given, the date given, and to whom given.Specific Authority 465.005, 465.0155, 465.014, 465.022 FS. Law Implemented 465.003(13), 465.014, 465.022, 893.07(1)(b) FS.History–Amended 5-19-72, Repromulgated 12-18-74, Formerly 21S-1.18, 21S-1.018, 21S-27.103, 61F10-27.103, Amended 9-19-94,Formerly 59X-27.103, Amended 10-15-01, 11-18-07.Podiatric Residents461.014(1)(f), Florida Statutes - Residency(f) A person registered as a resident podiatric physician under this section may, in the normal course of hisor her employment, prescribe medicinal drugs described in schedules set forth in chapter 893 andpursuant to s. 461.003(5) if:The person prescribes such medicinal drugs through use of a Drug Enforcement Administration numberissued to the hospital or teaching hospital by which the person is employed or at which the person'sservices are used;1. The person is identified by a discrete suffix to the identification number issued to such hospital;and2. The use of the institutional identification number and individual suffixes conforms to therequirements of the federal Drug Enforcement Administration.15.7
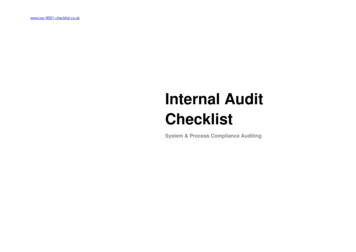
NURSING HOMEReceiving Medications in the Nursing Home1.Records of receiving a medication:a.Who and when ordered?b.Who and when received?2.Record of source:a.From the pharmacy?b.From home?c.Other?3.Records of medication delivery (delivery log or delivery manifest) should be maintainedby the facility and vendor Pharmacy for at least 2 years.These may be used during an AHCA investigation, a DEA investigation or a MedicaidAuditSAMPLE OF A DELIVERY LOGQuality Care Pharmacy6499 38th Ave NSt.Petersburg Fl 33710Shady Rest Nursing Home11440 49th Street NClearwater Florida8/1/20128/1/20128/1/20128/1/20128/1/2012Rx 711000 Mary SmithRx 711001 Mary SmithRx 711002 Mary SmithRx 683722 Tom JensenRx 711009 Gus Adams8/1/2012Furosemide 40mg #30Ibuprofen 400mg #30Slow K 8meq #30Isosorbide Mononitrate ER 60mg #30Phenytoin ER 100mg #30Nurse SignatureDate15.8
NURSING HOMEThe Disposition of Medication in the Nursing Home1. Methods of dispositiona.b.c.d.e.f.Proof of use (administered to resident as documented on the MAR)Transfer of control drugs to the D.O.N. for DestructionWaste (dropped doses or refused doses)Returned to family or residentReturned to the pharmacy for creditPilferage (will your audit trail catch missing meds?)2. Discontinued Medicationsa. When a drug order is discontinued the drug must be removed from the normal drugstorage area (i.e. drug cart) and placed in an area clearly marked for discontinuedmedicationsb. The facility policy will indicate whether the medication can be returned to pharmacyfor credit, destroyed in-house by nursing or if a controlled substance transferred tothe D.O.N. for destructionc. The facility should have a standard format for logging in these discontinuedmedications and identifying what happened to the remaining doses. (see sampleform)d. The disposition records becomes part of the patient’s permanent chart3. Discharge Medications in the Nursing Homea. All medications of discharged residents must be removed from the nursingdrug cart in a “timely manner”.b. Upon discharge, all medications may be sent home with the resident if soordered by the physician.c. Under certain per diem contracts the meds may need to be returned toPharmacy unless the family or facility wishes to pay for the remainingdoses.d. The disposition records becomes part of the patient’s permanent chart15.9
Federal Register/Vol. 75, No. 173/Wednesday, September 8, 2010/Notices54627ENVIRONMENTAL PROTECTION AGENCY[Frl-9197-7]Best management practices for unused pharmaceuticals at health care facilitiesAGENCY: ENVIRONMENTAL PROTECTION AGENCY (EPA).Action:notice.Summary: EPA is requesting public comments on a draft guidance document entitled,best management practices for unused pharmaceuticals at health carefacilities. The guidance is targeted at hospitals, medical clinics, doctors’offices, long-term care facilities and veterinary facilities. EPA expects that thisdocument will help reduce the amount of pharmaceuticals that are dischargedto water bodies.Dates: EPA requests comments on or before November 8, 2010. Comments received afterthis date may not be Incorporated into the final guidance document.Addresses: EPA prefers receiving comments by e-mail. Please send e-mail comments tounusedpharms@epa.gov and include your name and Organizational affiliation,if any. You may also send comments by postal mail to Meghan Hessenauer,engineering and analysis division (4303t), U.S. Environmental ProtectionAgency, 1200 Pennsylvania Avenue, NW., Washington, dc 20460.For further information contact: Meghan Hessenauer, engineering and analysis division,telephone: 202-566-1040; e-mail: Hessenauer.meghan@epa.gov.Supplementary information: Pharmaceuticals are being discovered in our nation’s watersat very low concentrations. EPA has been studying unused pharmaceutical disposalpractices at health care facilities, prompted by the concern that large amounts ofpharmaceuticals are being flushed or disposed of down the drain, ultimately ending upin rivers, streams and coastal waters.The agency has drafted a guidance document for health care facilities, which describes:1. Techniques for reducing or Avoiding pharmaceutical waste;2. Practices for identifying and managing types of unused pharmaceuticals; andapplicable disposal regulations. The guidance is targeted at hospitals, medical clinics,doctors’ offices, long-term care facilities and veterinary facilities.3. EPA expects that this document will help reduce the amount of pharmaceuticals thataredischarged to water bodies. The document is available on EPA’s Web nusedpharms index.cfm.EPA has visited many facilities and consulted with organizations in the health care industry, aswell as federal, state and local government agencies. EPA continues to solicitrecommendations from a wide range of stakeholders and welcomes comments on thedraft document. We plan to publish a final version of the document in late 2010.Dated: September 1, 2010.Ephraim S. King, Director, Office of Science and Technology.[FR Doc. 2010-22325 Filed 9-7-10; 8:45 am]15.10
64B16-28.140 Record Maintenance Systems for All Pharmacy Permits.(1) Requirements for records maintained in a data processing system.(a) The pharmacy must comply with the provisions of 21 C.F.R. Section 1304.04 (a regulation of the Federal DrugEnforcement Administration), which is hereby incorporated by reference as of March 1, 1998, when such is applicableto operate such a data processing system if any controlled substances (as that term is used in Ch. 893, F.S.) aredispensed from the pharmacy.(b) Any pharmacy using a data processing system must meet the requirements of 21 C.F.R. Section 1306.22, whichis hereby incorporated by reference as of March 1, 1998.(c) If a pharmacy’s data processing system is not in compliance with this subsection, the pharmacy must maintain amanual recordkeeping system as specified in Rule 64B16-27.800, F.A.C., and Section 893.07, F.S.(d) Original prescriptions, including prescriptions received as provided for in Rule 64B16-28.1003, F.A.C.,Transmission of Prescription Orders, shall be reduced to a hard copy if not received in written form. All originalprescriptions shall be retained for a period of not less than four (4) years from date of last filling. To the extentauthorized by 21 C.F.R. Section 1304.04, a pharmacy may, in lieu of retaining the actual original prescriptions, use anelectronic imaging recordkeeping system, provided such system is capable of capturing, storing, and reproducing theexact image of the prescription, including the reverse side of the prescription if necessary, and that such image beretained for a period of no less than four (4) years from the date of last filling.(e) Original prescriptions shall be maintained in a two or three file system as specified in 21 C.F.R. 1304.04(h).(f) Requirements for back-up systems.1. The pharmacy shall maintain a back-up copy of information stored in the data processing system using disk, tapeor other electronic back-up system and update this back-up copy on a regular basis, at least weekly, to assure that data isnot lost due to system failure.2. Data processing systems shall have a workable (electronic) data retention system which can produce an audittrail of drug usage for the preceding four (4) years as specified in Rule 64B16-27.800, F.A.C.(g) Change or discontinuance of a data processing system.1. Records of dispensing. A pharmacy that changes or discontinues use of a data processing system must:a. Transfer the records of dispensing to the new data processing system; orb. Purge the records of dispensing to a printout which contains the same information required on the daily printoutas specified in paragraph (3)(b) of this section. The information on this hard-copy printout shall be sorted and printed byprescription number and list each dispensing for this prescription chronologically.2. Other records. A pharmacy that changes or discontinues use of a data processing system must:a. Transfer the records to the new data processing system; orb. Purge the records to a printout which contains all of the information required on the original document.3. Maintenance of purged records. Information purged from a data processing system must be maintained by thepharmacy for four (4) years from the date of initial entry into the data processing system.(h) Loss of Data. The prescription department manager shall report to the Board in writing any significant loss ofinformation from the data processing system within 10 days of discovery of the loss.(2) All transfers of prescriptions must be strictly in accordance with the provisions of Section 465.026, F.S., andRule 64B16-27.105, F.A.C.(3) Records of dispensing.(a) Each time a prescription drug order is filled or refilled, a record of such dispensing shall be entered into the dataprocessing system.15.11
(b) The data processing system shall have the capacity to produce a daily hard-copy printout of all originalprescriptions dispensed and refilled. This hard copy printout shall contain the following information:1. Unique identification number of the prescription;2. Date of dispensing;3. Patient name;4. Prescribing practitioner’s name;5. Name and strength of the drug product actually dispensed, if generic name, the brand name or manufacturer ofdrug dispensed;6. Quantity dispensed;7. Initials or an identification code of the dispensing pharmacist; and8. If not immediately retrievable via CRT display, the following shall also be included on the hard-copy printout:a. Patient’s address;b. Prescribing practitioner’s address;c. Practitioner’s DEA registration number, if the prescription drug order is for a controlled substance.d. Quantity prescribed, if different from the quantity dispensed;e. Date of issuance of the prescription drug order, if different from the date of dispensing; andf. Total number of refills dispensed to date for that prescription drug order.(c) The daily hard-copy printout shall be produced within 72 hours of the date on which the prescription drugorders were dispensed and shall be maintained in a separate file at the pharmacy. Records of controlled substances shallbe readily retrievable from records of non-controlled substances.(d) Each individual pharmacist who dispenses or refills a prescription drug order shall verify that the data indicatedon the daily hard-copy printout is correct, by dating and signing such document in the same manner as signing a checkor legal document (e.g., J.H. Smith, or John H. Smith) within seven days from the date of dispensing.(e) In lieu of producing the printout described in paragraphs (b) and (c) of this section, the pharmacy shall maintaina log book in which each individual pharmacist using the data processing system shall sign a statement each day,attesting to the fact that the information entered into the data processing system that day has been reviewed by him orher and is correct as entered. Such log book shall be maintained at the pharmacy employing such asystem for a period of four (4) years after the date of dispensing provided, however, that the dataprocessing system can produce the hard-copy printout on demand by an authorized agent of the Department of Health.If no printer is available on site, the hard-copy printout shall be available within 48 hours with a certification by theindividual providing the printout, which states that the printout is true and correct as of the date of entry and suchinformation has not been altered, amended or modified.(f) The prescription department manager and the permit holder are responsible for the proper maintenance of suchrecords and responsible that such data processing system can produce the records outlined in this section and that suchsystem is in compliance with this subsection.(g) Failure to provide the records set out in this section, either on site or within 48 hours for whatever reason,constitutes failure to keep and maintain records.(h) In the event that a pharmacy which uses a data processing system experiences system downtime, the followingis applicable;1. An auxiliary procedure shall ensure that refills are authorized by the original prescription drug order and that themaximum number of refills has not been exceeded or that authorization from the prescribing practitioner has beenobtained prior to dispensing a refill; and2. All of the appropriate data shall be retained for on-line data entry as soon as the system is available for use again.(4) Compounding records. A written record shall be maintained for each batch/sub-batch of a compounded productunder the provisions of Rule 64B16-27.700, F.A.C. This record shall include:(a) Date of compounding.15.12
(b) Control number for each batch/sub-batch of a compounded product. This may be the manufacture’s lot numberor new numbers assigned by the pharmacist. If the number is assigned by the pharmacist, the pharmacist shall alsorecord the original manufacture’s lot number and expiration dates. If the original numbers and expiration dates are notknown, the pharmacy shall record the source and acquisition date of the component.(c) A complete formula for the compounded product maintained in a readily retrievable form includingmethodology and necessary equipment.(d) A signature or initials of the pharmacist or pharmacy technician performing the compounding.(e) A signature or initials of the pharmacist responsible for supervising pharmacy technicians involved in thecompounding process.(f) The name(s) of the manufacturer(s) of the raw materials used.(g) The quantity in units of finished products or grams of raw materials.(h) The package size and number of units prepared.(i) The name of the patient who received the particular compounded product.(5) Authorization of additional refills. Practitioner authorization for additional refills of a prescription drug ordershall be noted as follows:(a) On the daily hard-copy printout; or(b) Via the CRT display.(6) Any other records, policy and procedure manuals, or reference materials which are not specifically required bystatute or rule to be kept in a hard copy may be kept in a readily retrievable data processing system which complies withthe provisions of subparagraph (1)(f)1.Rulemaking Authority 465.005, 465.022 FS. Law Implemented 465.003(14), 465.022, 465.026, 465.035, 893.07 FS. History–New 316-94, Formerly 61F10-28.140, Amended 3-12-97, 6-4-97, Formerly 59X-28.140, Amended 10-29-97, 6-15-98, 11-11-98, 10-15-01,3-24-14.15.13
NURSING HOMEExtracted from: Nursing Homes - Clarification of Guidancerelated to Medication Errors and Pharmacy Services - CMSNovember 2012B. Fentanyl PatchesTag F431- Service Consultation requires a licensed pharmacist, who isemployed by or provides services to a facility, to establish a system ofrecords of receipt and disposition of all controlled medications. Thesystem should enable periodic, accurate reconciliation and accountingof all controlled drugs. Fentanyl transdermal patches are a controlledsubstance commonly used in nursing homes for pain medication. Thesepatches present a unique situation given the multiple boxed warnings,the potential for abuse, misuse and diversion, and the substantialamount of fentanyl remaining in the patch after use. The facility’spolicies must address safe and secure storage, limited access andreconciliation of controlled substances in order to minimize loss ordiversion, and provide for safe handling, distribution and disposition ofthe medications.One benefit of the patch is the continuous delivery of fentanyl over 72hours. This slow-release of fentanyl from the transdermal reservoirallows for more consistent pain control in patients with chronic pain.This unique delivery system, however, is not impervious to diversion,even after the fentanyl patch has been used, removed and/or disposed.One study determined that even after three days of use, 28 to 84.4% ofthe original fentanyl dose was still present in the patch. The study notedthat the dose remaining in the patch was within the limits of a lethalfentanyl dose.7The remaining fentanyl in a used patch is a potential vehicle of abuseand accidental overdose and warrants implementation of adequatedisposal policies. Fentanyl products contain several boxed warningsrelated to potential abuse, misuse, and diversion, and specifically, thecontraindication of fentanyl transdermal patch use in individuals whoare not opioid tolerant.Staff should dispose of fentanyl patches in the same manner as wastingof any other controlled substances, particularly because the activeingredient is still accessible. Wasting must involve a secure and safemethod, so diversion and/or accidental exposure are minimized. TagF425 requires the facility’s procedures to address the disposition of allmedications. This includes but is not limited to:15.14
Timely identification and removal of medications from the currentsupply of medications for disposition; Identification of storage method for medications awaiting final disposition; Control and accountability of medications awaiting final disposition; Documentation of actual disposition for both full dose and anyother remaining partial dose; and A method of disposition consistent with applicable state andFederal requirements, local ordinances, and standards ofpractice.Survey Implications:If surveyors identify misuse or diversion of a controlled substance,they should consider and investigate these requirements: F309 - Quality of care, for evidence and/or potential outcomes,such as unrelieved pain. For example, evidence that on aparticular shift, or when a particular staff member isworking, that the resident’s pain symptoms are notrelieved to the extent possible but the pain symptoms aremet to the extent possible on other shifts; F425 - Pharmacy Services, for policies for safeguarding and access,monitoring, administration, documentation, reconciliation anddestruction of controlled substances; F431 - Pharmacy service consultation, for drug records andreconciliation of controlled drugs; F514 - Clinical Records, accuracy of medical record and forthe documentation of the administration of themedication and outcomes; or F520 - Quality assessment and assurance, for how the QAAcommittee monitors the administration, reconciliationand disposition of controlled substances in the facility.In addition, if the investigation identifies diversion of a resident’smedication, the surveyor must review for F224- Misappropriation ofResident’s Property. If it is determined that a resident’s medications werediverted for staff use, the State Agency must make referrals toappropriate agencies, such as local law enforcement; Drug EnforcementAdministration; State Board of Nursing; State Board of Pharmacy; andpossibly the State licensure Board for Nursing Home Administrators.15.15
NURSING HOMES4. Compliance issues to be reviewed by the Consultant Pharmacist Monthlya. Verbal orders not written in the chartb. New orders were never sent to Pharmacy for processingc. Discontinued orders still in used. Discontinued medications stored with active medicationse. Doctors signatures in place renewing orders in a timely manner (every 30 days)f. Evidence of primary doctor involved in P.A. prescriptions and controlledsubstances orders written by an ARNPg. All orders have complete directions as described aboveh. The audit trail from order (or reorder) to destruction is intact15.16
NURSING HOMETHE RETURN OF UNIT DOSE MEDICATION TO THE PHARMACYNote: This regulation does not address the type of facility that can return medications. Theboard has taken the position that only facilities with a Pharmacy license and aConsultant Pharmacist are allowed to return medications for credit.This would prohibit ALF’s (without a Special ALF license), Group homes, ADT’s, FACTprograms, Juvenile Detention Centers and Correctional facilities without an InstitutionalModified license from returning medication even if they are in unit dosed packaging andstored centrally.15.17
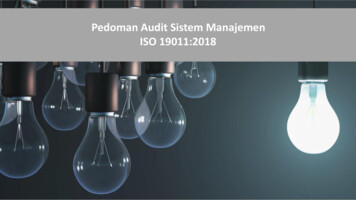
NURSING HOMESAMPLE FORMDischarge Drug List FormPatient Name Room #PhysicianI certify that the following drugs have been delivered to and received by:1.Signature of Charge NurseDateI acknowledge that these medications are not currently packed in child resistant packaging and thatI waive this special packaging requirement Yes ( )No ( )I request that these medications be repackaged by the Pharmacy in child resistant packaging prior tomy receipt of this medication.Yes ( )No ( )2.Signature of Patient or Responsible PartyDatePrescriptionNameQuantityDrugs reviewed and evaluated by pharmacist:3.Signature of PharmacistDate4.Disposition of Drugs:WMC-30815.18
NURSING HOMESAMPLE POLICY & METHODSMedications to Resident on DischargePOLICY:It is the policy of this facility to send home the resident’s medications upon discharge if thephysician orders it.METHODS:1.The physician must authoriz
3. Discharge Medications in the Nursing Home a. All medications of discharged residents must be removed from the nursing drug cart in a “timely manner”. b. Upon discharge, all medications may be sent home with the resident if so ordered by the physician. c. Under certa