Transcription
Healthy People 2020:Who’s Leading theLeading HealthIndicators?
Carter BlakeyDeputy DirectorOffice of Disease Prevention and Health PromotionU.S. Department of Health and Human Services
Who’s Leading the LeadingHealth Indicators? Leading Health Indicators are:o Critical health issues that, if addressedappropriately, will dramatically reduce theleading causes of preventable deaths andillnesseso Linked to specific Healthy People objectiveso Intended to motivate action to improve thehealth of the entire population 1200 Healthy People objectivesLHIs are a subset ofHealthy Peopleobjectives3
Who’s Leading the LeadingHealth Indicators?Featured Speakers: Don Wright, MD, MPH – Director, Office of Disease Preventionand Health Promotion, U.S. Department of Health and HumanServicesRichard McKeon, PhD – Suicide Prevention Branch Chief,Division of Prevention, Traumatic Stress, and Special Programs,Center for Mental Health Services, Substance Abuse and MentalHealth Services AdministrationJulie Goldstein Grumet, PhD – Director of Health andBehavioral Health Initiatives, Suicide Prevention ResourceCenter, Director, Zero Suicide Institute, Education DevelopmentCenterBrian Ahmedani, PhD, LMSW – Director, Center for HealthPolicy and Health Services Research, Director of Research,Behavioral Health Services, Henry Ford Health System4
Don Wright, MD, MPHDeputy Assistant Secretary for HealthDirectorOffice of Disease Prevention and Health PromotionU.S. Department of Health and Human Services
Mental HealthMental HealthMental Health Disorders State of well-being Health conditions characterized byalterations in thoughts, mood, and/orbehaviors Individuals can:- Realize their own abilities- Cope with normal stresses of life- Work productively and fruitfully- Contribute to their own community Can have harmful and long-lastingeffects- High psychosocial and economic costs May impact their family, relationships,and ability to be productive Association between mental healthdisorders and physical health6
Risk Factors Related to Mental Health Indicators of mental health Emotional well-beingPsychological well-beingSocial well-beingRisk factors linked to mental health Race/ethnicitySexGenderAgeIncomeEducationSexual orientationGeographic location7
Mental Health – Across the Lifespan Children and Adolescents Nearly 20% experience a mental health disorder Onset can be as early as 6 years old Early treatment and diagnosis of mental health disorders mayhelp lower the risk for unhealthy and unsafe behaviors Adults About 19% live with a mental health disorder Mental health disorders affect young adults (18 to 25 years) morethan other adult age groups Preventing mental health disorders and promoting good mentalhealth can create supportive living environments for people to adoptand maintain healthy lifestyles8
Mental HealthLeading Health Indicators Reduce the suicide rate(MHMD-1) Adolescents with amajor depressiveepisode (MHMD-4.1)9
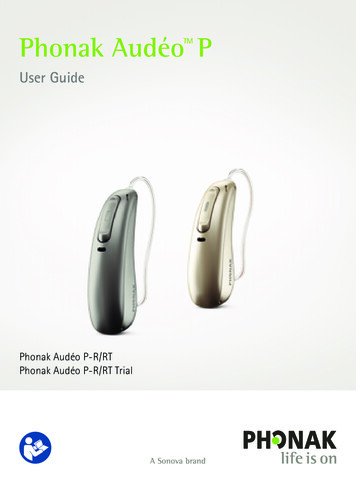
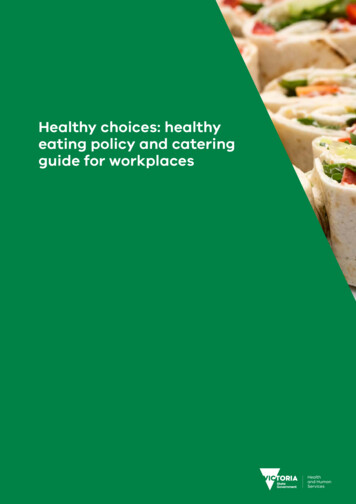
Suicide Rate by Race/Ethnicity, 2017NOTE: Data are for ICD-10 codes *U03, X60-X84, Y87.0 reported as underlying cause of death. American Indian includesAlaska Native. Asian includes Pacific Islander. The categories black and white exclude persons of Hispanic origin.Persons of Hispanic origin may be any race. Data are age-adjusted to the 2000 standard population.SOURCE: National Vital Statistics System–Mortality (NVSS–M), CDC/NCHS; Bridged–race Population Estimates, CDC/NCHSand Census.Obj. MHMD-1Decrease desired
Suicide Rate by Age, 2017INOTE: 95% confidence interval. Data are for ICD-10 codes *U03, X60-X84, Y87.0 reported as underlyingcause of death. Data for the total population are age adjusted to the 2000 standard population.SOURCE: National Vital Statistics System–Mortality (NVSS–M), CDC/NCHS; and Bridged–race PopulationEstimates, CDC/NCHS and Census.Obj. MHMD-1
Suicide and Major Depressive Episode(MDE) among Adolescents by Sex, 2017NOTE: Data are for adolescents aged 12-17 who died by suicide or reported having a Major Depressive Episode (MDE) in thepast 12 months. Suicide data are for ICD-10 codes *U03, X60-X84, Y87.0 reported as underlying cause of death.SOURCES: National Vital Statistics System–Mortality (NVSS–M), CDC/NCHS; Bridged–race Population Estimates, CDC/NCHSand Census. National Survey on Drug Use and Health (NSDUH), SAMHSA.Related Obj. MHMD-1;Obj. MHMD-4.1,Decrease desired
Major Depressive Episode (MDE) among Adolescents, 2017INOTE: 95% confidence interval. *2008 Total HP2020 baseline. Data are for adolescents aged 12-17 years whoreported having a Major Depressive Episode (MDE) in the past 12 months. American Indian includes Alaska Native. NativeHawaiian includes other Pacific Islander. The categories black and white exclude persons of Hispanic origin. Persons of Hispanicorigin may be any race.Obj. MHMD-4.1SOURCE: National Survey on Drug Use and Health (NSDUH), SAMHSA.
SAMHSA SUICIDE PREVENTION EFFORTSRichard McKeon, Ph.D.Chief Suicide Prevention BranchCMHS, SAMHSAHealthy People 2020Leading Health Indicators7/18/19
DisclaimerThe views, opinions, and content expressed inthis publication do not necessarily reflect theviews, opinions, or policies of the Center forMental Health Services (CMHS), the SubstanceAbuse and Mental Health ServicesAdministration (SAMHSA), or the U.S.Department of Health and Human Services(HHS).15
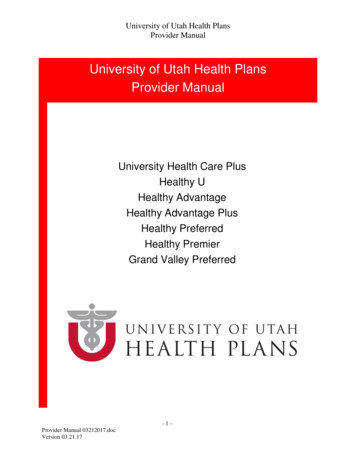
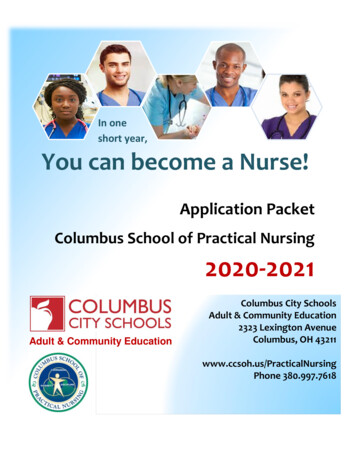
PROBLEMSUICIDE RATES INCREASEDIN ALMOST EVERY STATE.Suicide rates rose across the USfrom 1999 to 2016.Increase 38 - 58%Increase 31 - 37%Increase 19 - 30%Increase 6 - 18%Decrease 1%SOURCE: CDC’s National Vital Statistics System;CDC Vital Signs, June 2018.
Percentage increases in state suicide ratesTop 10
SAMHSA Programs, Efforts, Initiatives Garrett Lee Smith (GLS) State/Tribal Youth Suicide Prevention andIntervention Program– *Evaluations show program lowers rates of suicide and suicide attempts withincreased longevity and robustness when duration of grant is increased GLS Campus Suicide Prevention Grant ProgramZero Suicide in Health SystemsSuicide Prevention Resource CenterNational Strategy for Suicide Prevention grantsNative Connections (Tribal Behavioral Health)National Suicide Prevention LifelineCrisis Center Follow-up grantsSMVF TA- Mayor’s and Governor’s ChallengeFamily Toolkit18
National Strategy for Suicide Prevention19
Saving Lives:Impact of the 2012 National Strategyfor Suicide PreventionAmerican Association of Suicidology2015 Annual Meeting
The Garrett Lee Smith (GLS) Suicide Prevention National Outcomes Evaluation is supported through contract no. HHSS283201200007I/HHSS28342002T (reference no. 283-12-0702) awarded to ICF Internationalby the Center for Mental Health Services (CMHS), Substance Abuse and Mental Health Services Administration (SAMHSA), US Department of Health and Human Services (HHS).THE IMPACT OF GLS SUICIDE PREVENTIONPROGRAM ON YOUTH SUICIDAL BEHAVIORLucas Godoy Garraza (ICF International); Christine Walrath (ICFInternational); David Goldston (Duke CSSPI); Hailey Reid (ICFInternational), Richard McKeon (SAMHSA)
Proxy for GLS Program Implementation 39,000 TrainingEvents 1.4M TraineesMore than 96% of State and Tribal grantees conduct Gatekeeper Trainings*data through July 201822
Improving Post Discharge Safety ED SAFE demonstrated reduction in suicidalbehavior for suicidal people discharged fromED’s doing telephonic follow up. SafeVetreplicated this finding. White Mountain Apache/JHU Center forAmerican Indian Health almost 40% reductionin suicides from 2006-2012-centerpiece istribally mandated reporting and follow up.
“Celebrating Life”&“Empowering Our Spirits”Preventing Suicide in White MountainApache Youth
Longer-term Impact on Youth Suicide MortalitySustained impact after consecutive years of GLS programming25
Longer-term Impact on Youth Suicide MortalityGreater impact seen in rural areas 2.4 fewer deaths per 100,000 youth2 years after GLS implementation 20% stronger effect in rural countiesthan in non-rural counties or 1 fewerdeath per 244,000 youthThe decrease in youth suicide mortality appears to be stronger in ruralcommunities26
24 Cities Participating in Mayor’s ChallengeAlbuquerque, NMAtlanta, GAAustin, TXBillings, MTClarksville, TNColumbus, OHDetroit, MIHelena, MTHillsborough County, FLHouston, TXJacksonville, FLKansas City, MOLas Vegas, NVLos Angeles, CAManchester, NHMecklenburg County, NCOklahoma City, OKPhoenix, AZReno, NVRichmond, VASuffolk County, NYTopeka, KSTulsa, OKWarwick, RI27
Mayors Challenge and Crisis Intercept Mapping Sites (2018-2019)Mayors Challenge SitesAlbuquerque, NMAtlanta, GAAustin, TXBillings, MTClarksville, TNColumbus, OHDetroit, MIHelena, MTHillsborough County, FLJacksonville, FLKansas City, MOLas Vegas, NVLos Angeles, CAManchester, NHMecklenburg County, NCOklahoma City, OKPhoenix, AZReno, NVRichmond, VASuffolk County, NYTopeka, KSTulsa, OKWarwick, RICrisis Intercept Mapping SitesAlbuquerque, NMAtlanta, GAClarksville, TNKansas City, MOHelena, MTHouston, TXLas Vegas, NVLos Angeles, CAManchester, NHMecklenburg County, NCRichmond, VATruckee Meadows, NV28
Rural Primary Care Toolkit29
To Live to See the Great Day that Dawns30
National Suicide Hotline Improvement Act:SAMHSA Report to FCCRichard McKeon, Ph.D.Suicide Prevention Branch ChiefSubstance Abuse and Mental Health Services AdministrationU.S. Department of Health and Human ServicesFCC 3.28.2019
33
Potential Impact of N11 Based on SAMHSA’s experience with national and statecrisis intervention efforts over the past 18 years, andinformed by a meeting of experts and stakeholders inmental health, crisis intervention, emergency servicesand suicide prevention that SAMHSA convenedNovember 29 to 30, 2018, our judgment is that an N11national suicide prevention number has the potentialto play a key role in improving national crisisintervention and suicide prevention efforts; if thelaunch of a new number is accompanied by efforts todevelop a more coordinated crisis system with greatercapacity and access to sophisticated data andtechnology systems, and an ongoing commitment todata driven quality improvement.34
Ubiquitous and inexpensive technology ischanging nearly every other industry.
SAMHSA’s mission is to reduce the impact of substanceabuse and mental illness on America’s communities.Richard McKeonChief, Suicide Prevention .hhs.govwww.samhsa.gov1-877-SAMHSA-7 (1-877-726-4727) 1-800-487-4889 (TDD)36
Suicide Prevention:Resources for the CommunityJulie Goldstein Grumet, PhDDirector, Health and Behavioral Health InitiativesSuicide Prevention Resource CenterDirector, Zero Suicide InstituteJuly 18, 2019@SPRCTweetswww.sprc.org
SPRC Suicide Prevention Resource CenterFunding and DisclaimerThe Suicide Prevention Resource Center at EDC is supportedby a grant from the U.S. Department of Health and HumanServices (HHS), Substance Abuse and Mental Health ServicesAdministration (SAMHSA), Center for Mental Health Services(CMHS), under Grant No. 5U79SM062297.The views, opinions, and content expressed in this product donot necessarily reflect the views, opinions, or policies ofCMHS, SAMHSA, or HHS.Suicide Prevention: Resources for the Communitywww.sprc.org38
SPRC Suicide Prevention Resource CenterThe national Suicide PreventionResource Center (SPRC) is your onestop source for suicide prevention.We help you develop, deliver, andevaluate t/HCorlessedc.orgprevention programs.CONNECT WITH USWhat we offer Best practice modelsToolkitsOnline trainingsResearch summaries and more!@SPRCTweetswww.sprc.orgWho we serve g@SuicidePreventionResourceCenter@SPRCTweets
SPRC Suicide Prevention Resource CenterVisit SPRC.orgSign up for SPRC’s Weekly Sparknewsletter for the latest news,research, and announcements.Learn at your own pace with onlinecourses, learning labs, and briefvideos.Discover how to apply suicideprevention best practices with SPRC’sEffective Suicide Prevention Model.Access a wealth of resources,including toolkits, fact sheets, successstories, and more!Explore a library of suicideprevention programs with evidenceof effectiveness.Find information on suicideprevention efforts in your state.@SPRCTweetswww.sprc.org
SPRC Suicide Prevention Resource CenterEffective Preventionwww.sprc.orgSuicide Prevention: Resources for the Community41
SPRC Suicide Prevention Resource CenterA Comprehensive Approach to SuicidePreventionSuicide Prevention: Resources for the Communitywww.sprc.org42
SPRC Suicide Prevention Resource CenterGuiding Principleswww.sprc.orgSuicide Prevention: Resources for the Community43
SPRC Suicide Prevention Resource CenterStrategic Planningwww.sprc.orgSuicide Prevention: Resources for the Community44
SPRC Suicide Prevention Resource CenterEffective Prevention Effective prevention requires strategic planning. Suicide is multidimensional. No single approach will reduce suicide. Strategic planning offers you the time to learn about suicide in your community – use data todetermine where to focus your efforts. Successful endeavors incorporate: www.sprc.orgLived experiencePartnerships and collaborationSafe and effective messagingCulturally competent approachesEvidence-based preventionSuicide Prevention: Resources for the Community45
SPRC Suicide Prevention Resource CenterSuicide is a Complex, Multidimensional Problem Bundle of interventions Prevention and intervention efforts must be sustained Data driven decisions Continuous quality improvementwww.sprc.orgSuicide Prevention: Resources for the Community46
SPRC Suicide Prevention Resource CenterWhy Evaluation Is ImportantEvaluating your program will help you: Identify and solve problemsDetermine progress toward your goalsShow partners, stakeholders, policymakers, funders, and the community the value of suicidepreventionDecide on how to enhance or expand your suicide prevention effortsKey aspects of evaluating your program: Hire an evaluator (if you don’t have one on staff)Involve the agencies, organizations, and people who will be collecting or providing data for theevaluationResearch the suicide problem in your community, including risk and protective factorsDevelop a logic model that shows how your planned activities will lead to your long-term goalsMonitor progress and resultsAnalyze findings and use them to enhance your suicide prevention effortsGathering data can be challenging – Don’t let PERFECT be theenemy of GOODwww.sprc.orgSuicide Prevention: resources for the Community47
SPRC Suicide Prevention Resource veillancewww.sprc.orgSuicide Prevention: Resources for the Community48
SPRC Suicide Prevention Resource CenterResources and WebsitesSuicide Prevention Resource Center: sive-approach al-learning-lab http://www.sprc.org/states l-strategy-suicide-preventionZero Suicide: ZeroSuicide.com s-outcomes/outcome-stories udy ro-suicidewww.sprc.orgSuicide Prevention: Resources for the Community49
SPRC Suicide Prevention Resource CenterContact InformationJulie Goldstein Grumet, omwww.sprc.orgSuicide Prevention: Resources for the Community50
Henry Ford Health System’sZero Suicide InitiativeBrian K. Ahmedani, PhDDirector, Center for Health Policy & Health Services ResearchHenry Ford Health SystemJuly 2019
Details about Henry Ford Henry Ford Health System (HFHS)– Large health system serving southeast- and mid- Michigan,including the Detroit metropolitan area. 8 hospitals and 40 medical centers.– Full range of services: Primary care, outpatient medical specialties, inpatient, and emergency. Behavioral health services, including a stand-alone psychiatric hospital, achemical dependency treatment center, additional inpatient services,partial hospitalization, and outpatient care.– Serves 1 million patients per year.
The Henry Ford Story Institute of Medicine Report: “Crossing the Quality Chasm” RWJ Grant Opportunity Finalist– Application for ‘Perfect Depression Care’ in Behavioral HealthServices department at HFHS “Blues Busters” Team– Senior leadership, physicians, other clinical staff, and patientadvisors. Zero Suicides becomes the goal; Expanded to all conditions(not just depression). Expansion into primary care and other medical settings.
The Evolution of Zero Suicide Started at Henry Ford The research evolved throughout the 2000s. National Action Alliance formed to create a new National Strategy– Focus on Zero Suicide. Zero Suicide adopted by Substance Abuse and Mental HealthServices Administration (SAMHSA). Resources made available by Suicide Prevention Resource Center(SPRC). International Zero Suicide movement begins.
Care Redesign High Reliability (Airline industry, 100% hand washing, zero infections). Map out a “perfect” delivery of care model that fits within yourresources and staffing– Universal vs. Selective approaches. High intensity treatments matched to those at greatest risk, while low intensity approachesmatched to those at lowest risk.– Use creativity and plan for changes. Policies and procedures must support this model. The care model must be integrated into work flow. The care model must be integrated into your EMR.
The Care Pathway Screening, risk stratification. Suicide risk assessment and safety plan. Level of risk determines the treatment / intervention, via evidence-basedapproaches (CBT / DBT). Strong family involvement. Means reduction protocol reviewed at every visit. Train entire team on the model and clinical approaches. Focus on access and engagement. Rapid cycle quality improvement. Henry Ford Zero Suicide Clinical Guidelines available al-health/zero-suicide
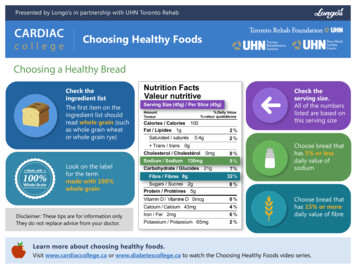
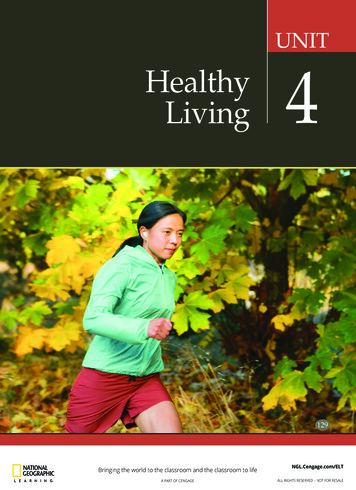
Suicide Rates at Henry Ford*Improvement in other outcomes as well.
Key Takeaways / Current Grant The program was associated with a significant reduction in suicidemortality among our patient population. Ongoing quality improvement is paramount.– E.g., expansion into primary care after recognizing many patients were neverreaching behavioral health. Our current research grant from the National Institutes of Health willallow us to examine which care pathways best prevent suicide andsuicide attempt across 6 large health systems and 9 millionpatients per year (Grant # U01MH114087).
RoundtableDiscussion59
Stay Connected Visit healthypeople.gov to learn more aboutthe Healthy People 2020 Leading HealthIndicators To receive the latest information about HealthyPeople 2020 and related events, visit ourwebsite to: Join the Healthy People 2020 Consortium Share how your organization is working toachieve Healthy People goalsFollow us on Twitter @gohealthypeople
Jul 18, 2019 · Center for Mental Health Services, Substance Abuse and Mental . Association between mental health disorders and physical health: 7: . Suffolk County, NY. Topeka, KS. Tulsa, OK. Warwick, RI. 2 8. Mayors Challenge and Crisis I