Transcription
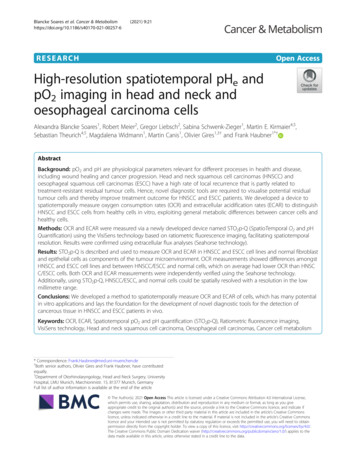
Principles of tumour immunologyMichele TengNov 20th 2017, SingaporeCancer Immunoregulation andImmunotherapy LaboratoryQIMR Berghofer MRIBrisbane, Australiamichele.teng@qimrberghofer.edu.au
Disclosure Slide I have received speakers bureau honoria fromMerck Sharp & Dohme.
Talk Outline1. Hallmarks of Cancer2. Cells of the Immune system3. The Cancer Immunity Cycle- Tumor-associated antigens (TAA), Cellular and Humoral responses toTAA4. Conceptual developments in the field of tumourimmunology- Immunosurveillance and role of innate immunity, immune balanceagainst cancer
Sources of slide Charles Janeway’s Immunobiology text book Peer-reviewed articles (Pubmed) Online slides ( URL listed)
Cancer
Hallmarks of Cancer (2000)Hanahan and Weinberg, Cell 2000
Emerging Hallmarks and Enabling CharacteristicsHanahan and Weinberg, Cell 2011
Hallmarks of Cancer (2017)In Vitrogen
Immunology(Study of the immune system)
Cells of the immune systemILCs –innate lymphoid cellsMAITs –Mucosal associatedinvariant T cellsgd T cells – gamma delta T cells(ILCs)(gd, MAIT)
Cancer Immunology(Study of the response of the immune systemto cancer)
The Cancer-Immunity Cycle – Steps to generate aneffective anti-tumour responseChen and Mellman Immunity 2013
Not all cell deaths are equal(at priming an immune response)
Cells can die in different waysDAMPs Tumour fragmentsImmunogenic Cell Death (ICD)(Adjuvanticity, Antigenicity)DAMPs – Damageassociated molecularpatterns
Differential requirements for theimmunogenicity of cell deathTLR4Nat Rev Immunol. 2017 Feb;17(2):97-111. doi: 10.1038/nri.2016.107.
The Cancer-Immunity CycleImmunity. 2013 Jul 25;39(1):1-10. doi: 10.1016/j.immuni.2013.07.012.
Types of professional AntigenPresenting Cells (APCs)Nat Rev Immunol. 2014 Nov;14(11):719-30. doi: 10.1038/nri3754.
Activation of tumour-specific T cells by APCsTCR with the right specificity
Tumor-specific and tumor-associated antigens(Neoantigens) QIMR Berghofer Medical Research Institute 19
TAA – therapeutic targets?
Cell-mediated and humoral immuneresponses to tumour
Requirements for effective priming of T cellsFront. Oncol., 10 April 2014 https://doi.org/10.3389/fonc.2014.00077
The many flavours of CD4 T cellsTh22
Cell-mediated and humoral immuneresponses to tumour
T cell-independent and T cell-dependentB cell activation
Antibody mechanism of actionIgG1FcgRIIIa-activating receptorNK cells
Antibody mechanism of actionActivate cellulareffector functionAntibody-DependentCell-Mediated CytotoxicityAntibody-DependentCellular PhagocytosisBiolegend
ADCC - the underlying mechanism for the clinical efficacyof therapeutic anti-cancer antibodies.Biolegend
Effector responses of NK cells are regulated byinhibitory and activatory receptorsRelease ofCytokinesCytolysisTrends in Immunology 2011 32, 364-372DOI: (10.1016/j.it.2011.06.001)
Major inhibitory and activating receptors on NKcells and their cognate ligands on targetsNKp30 isoforms predictclinical outcome of GIST,neuroblastomaChan et al., 2014 Cell Death Differentiation
The Cancer-Immunity CycleImmunity. 2013 Jul 25;39(1):1-10. doi: 10.1016/j.immuni.2013.07.012.
When the Cancer Immunity Cycle issuccessfully completed
Cancer Immunology (pre 2000)Reason for failuresCancer Immunology (2000-2017)- What went right.
Conceptual Developments in Cancer mbination3ImmunemAb-based therapyReaction5Tumourinduced Immunesuppression
13EsKILLBATTLELOSESmyth et al. JEM 2000, Shankaran et al. Nature 2001Swann et al. J. Clin. Invest. 2007, Koebel et al. Nature 2007Teng et al., JLB 2008; Schreiber.Smyth. Science 2011 ResQIMR 2012,BerghoferMedicalResearchInstitute 36Teng et al., CancerTenget al.,JCI 2015
2Mutationalload correlates with frequency oftumour neoantigens. & responseEstimate of the neoantigen repertoire in human cancerSynder A et al., NEJM 2014van Allen et al., Science , 2015, Hugo W et al., Cell 2016Ton N. Schumacher, and Robert D. SchreiberScience 2015;348:69-74MHCQuality
3Immune contexture correlates with clinical outcomeNKTStromaImmune contextureassociated with goodprognosis in CRCChemokine CXCL9 CX3CL1 CXCL10 CCL2 CXCL13 CCL5Adhesion MADCAM1 ICAM1 VCAM1NeutrophilNKTH1 IL-12 IFN-γ IL-15TFH IL21BcellsTumor margin CD3 , CD8 ,CD45RO T cellsLocation, density, functionalorientation of toxic Granzymes Perforin GranulysinTH1 T-bet IRF1 STAT1BloodvesselEosinophilImmatureDCB cellsMast elial/smoothmuscle layerImmunoscoreTLSGalon et al., 2006 Science, Pages et al., 2005 NEJM,Fridman et al., 2012 NRC, Bindea el al., 2013 Immunity
Mechanism of Treg mediated immunosuppressionWorman C et al., Cell Mol Life Sci 2009
Mechanism of MDSC mediated immunosuppressionDmitry I. Gabrilovich Cancer Immunol Res 2017;5:3-8
4(trimAb)trimAbanti-DR5 (immunogenic cell death)anti-CD40 (activate APC)anti-CD137 (enhance effector T cell function and survival)MCA induced fibrosarcoma modelMCA50-180 dWT or KO mouseDetect sarcomaMeasure growthCommence treatment
Rejection of carcinogen-induced establishedtumors by trimAbUno et al. Nature Medicine, 2006
4 The four nodes to target for inducing maximal anti-tumour immunitySmyth et al., NRCO 2016
5Engagement of checkpoint receptors represents a majormechanism of tumour-induced immunosuppressionCheckpoint receptors:Brakes to limitoverzealousT cell activationAbout 20 interactionsregulate T cell immuneresponseAPC/TumourT cellMelero I et al.Nat Rev Cancer 2015
Checkpoint blockade can unleashendogenous anti-tumour responseORR – 10%2010ORR – 31%2012ORR – 53%2013ORR – 61%2015
Anti-PD-1 to be used as standard of care and incombination immunotherapiesORR –33.7% vs 11.9%2015ORR –31.7% vs 10.6%2015ORR –20% vs 9%2015ORR –44.8% vs 27.8%2016
Cancer immunotherapy-based combination studies underway in 2016Chen & MellmanNature 2017
Tumour microenvironment can be stratified into 4 types based onTILs and PD-L1 expression in tumoursTeng et al., 2015 Cancer Res
Summary Anti-PD-1/PD-L1 - will become the immunotherapeuticbackbone of future cancer treatments Cancers can be divided into four type– absence or presence of TILs and PD-L1 expression Efficient anti-tumour strategies must focus on hittingdifferent targets concurrently Key nodes to target in combination treatment––––abrogating immune suppressioninducing immunogenic cancer-cell death,enhancing antigen presentation/adjuvanticityinducing activation and survival of immune-effector cells
Summary Exome-sequencing data can be mined to– identify unique neoantigen profile of tumours– guide future personalized vaccine design for use in combinationtreatments A large proportion of patients have ‘immune ignorant’(cold) tumours,– predicted to have a poor prognosis regardless of any currentintervention– novel therapies have to be developed (Oncolytic virus, STINGagonist, CAR-T).
Moving Forward
Key issues in cancer immunotherapy1) Identifying biomarkers to predict what cancers and ptswill respond to anti-PD-1/PD-L12) How do we increase the proportion of patients whorespond to anti-PD-1/PD-L1?3) What therapies do we use to treat cancers withmicroenvironments that are resistant to anti-PD-1/PDL1 monotherapy?4) What do we do for patients who develop acquiredresistance to anti-PD-1 therapies?5) What is the optimal scheduling for administration ofcombination immunotherapy?6) How to assess the therapeutic index (anti-tumourefficacy/irAEs) of combination immunotherapies?
Overall SurvivalImproving the tail of the curve.Time
Thank Youwww.qimrberghofer.edu.au
Identifying biomarkers to predictpatients who will respond toanti-PD-1/PD-L1
Tumour microenvironment can be stratified into 4 typesbased on TILs and PD-L1 expression in tumoursTIL PD-L1 (38%)Type ITILPD-L1(41%)Type IIMelanomaType IVTIL PD-L1(20%)Type IIITILPD-L1 (1%)Taube et al. Sci Transl Med 2012, CCR 2014
Association of anti-PD-L1 response and tumour-infiltratingimmune cell PD-L1 expressionNature, 2014
Cancers with type I TME containing CD8 T cells and PD-L1most likely to respond to anti-PD-1/PD-L1Level of PD-1 expressionNgiow et al., Cancer Res 2015PDL2 expression?Tumeh et al. Nature (2014)
QIMR Berghofer Medical Research Institute 59
Factors that influence the cancer–immune set point
Biomarkers of response to PD-1/PDL1 blockadeAngiogenesisDensity, LocationPD-1 expression levelOther checkpointreceptorsEpigeneticsOther immune cellsCD8 T cellMMR-deficient/MSI-HSomatic vs Drivermutations(e.g mor/ImmunecellsIFN gene signature(early on txt)Tumor loadTimeDurability of ResponseMicrobiomeAgeExternal factorsPrior therapy
From bed-sideTo bed-sideClinical researchEx vivo/In vitro researchTo benchExperimentalMouse researchFrom bench QIMR Berghofer Medical Research Institute 62
Immunotherapy and GI cancerMelero I et al., Abstract presented at: 2017 Gastrointestinal Cancers Symposium;January 19-21, 2017; San Francisco, CA.
Atezolizumab (anti-PD-L1) – Tecentriq, approved for treatment of bladder cancer
Adaptive immune gene signature in early-ontreatment samples best predict respondersChen, P, Cancer Discov, 2016 EDT – median 1.4 months(0.7-26 months) Vilain et al EJC 2015; EDT(within 2 months of treatment)increase in intratumoral CD3 ,CD8 , CD68 in responders Non-responders – increasedVEGFACheckpoint immunotherapy: picking a winner Teng et al., Cancer Discovery 2016 in press
How do we increase the proportion ofpatients who respond to anti-PD-1/PD-L1?
Can we improve above the 50% ORR induced byanti-CTLA-4 & anti-PD-1?**Without the toxicity
Combination of anti-PD-1 or anti-CTLA-4 with IDOinhibitors (Indoximod) in melanomaAbstract #3075 ASCO 2016, Yousef Zakharia. Mhd Milhem
IDO - Indoleamine 2,3-dioxygenase, animmune suppressorAbstract #3075 ASCO 2016, Yousef Zakharia. Mhd Milhem
ORR 53%No increase in toxicityPhase II trial ongoing – 64ptsQuestions1) PFS?2) Durability3) Other cancers?
What therapies do we use to treat cancers withTME that are resistant to anti-PD-1/PD-L1monotherapy?
T-VEC anti-CTLA-4 Chemotherapy or targeted therapy anti-PD-1 Radiotherapy anti-CTLA-4 anti PD-1(Twyman-Saint Victor et al., Nature 2015) Type I IFN (poly-ic) anti-PD-1 (Bald et al. Cancer Discovery 2014)Microbiota (Zitvogel L et al, Gajewski T el,Science 2015) Engineering FcR engaging variants ofIgG (Ravetch Cancer Cell 2016) Scheduling (Neoadjuvant/adjuvant) CAR-T anti-PD-1anti-CD40 anti-IL-23anti-CD40 anti-CSFR1
What other cancers should we treatwith anti-PD-1/PD-L1?
PD-1 & PD-L1 expression in various typesof solid tumours
PD-1 TILs expression correlates with increasing mutational loadLe et al., NEJM, 2015; Maby et al., Cancer Res, 2015
Gut bacteria affect immunotherapy effectivenessSivan A et al., Science 2015Vétizou M et al., Science 2015The composition of intestinal microbiotaaffects checkpoint blockade efficacy andcan be manipulated to improve responses.Alexandra Snyder et al. Science 2015;350:1031-1032
Neoantigen presentation in the tumour microenvironmentKhalil, D. N. et al. (2016) Nat. Rev. Clin. Oncol.
T-cell inflamed phenotype gene expression signaturesto predict clinical benefit from pembrolizumab across 5cancer types
Biomarkers and response to pembrolizumab(pembro) in recurrent/metastatic head and necksquamous cell carcinoma (R/M HNSCC)
What do we do for patients who developacquired resistance to anti-PD-1therapies?
Jesse Zaretsky. Antoni Ribas NEJM 2016Mean time to relapse 624 days (range, 419 to 888)
Mechanisms of resistance Whole-exome sequencing of biopsy samples fomrpaired baseline and relapsing lesions in 4 pts 2 pts; IFNgR associated JAK1/JAK2 mutations lossof ability to respond to IFNg 1 pt; b2m mutation loss of surface MHC Iexpression 1 pt; - no defined genetic alterations to explainacquired resistance (no PDL1 on tumors pre/post txt)
Genomic and Transcriptomic Features of Response to Anti-PD-1Therapy in Metastatic MelanomaHugo W, . Ribas A, Lo R Cell 2016
Association of PD-L2 expression in humantumors with atezolizumab activity. QIMR Berghofer Medical Research Institute 85
QIMR Berghofer Medical Research Institute 86
QIMR Berghofer Medical Research Institute 87
QIMR Berghofer Medical Research Institute 88
Evidence for immunoediting in human tumoursRooney et al., Cell 2015 Analysis of 18 TCGA tumour typesshows genomic correlates of immunecytolytic activity Multiple tumour types demonstratestrong link between mutation load andlocal immunity Number of predicted MHC Class Iassociated neoantigens correlated withcytolytic activity. Lower than expectedin colorectal and other tumours,suggesting immune-mediatedelimination Infiltrated tumours are enriched forprobable escape lesions affectingCASP8, HLA, B2M
Integrative Analyses of Colorectal Cancer ShowImmunoscore Is a Stronger Predictor of Patient SurvivalThan Microsatellite Instability MSI and a subgroup of MSSpatients have high intratumoraladaptive immune gene expression Functional effector anti-frameshiftmutation CTLs kill tumor cells inMSI patients Genetic evidence ofimmunoediting in human CRC, inparticular for MSI patients Immunoscore gives an indicatorof tumor recurrence and survivalbeyond MSI stagingMlecnik et al., Immunity 2016
QIMR Berghofer Medical Research Institute 91
Tumor associated antigens and tumor specific lasia-robbins-path-13540987
ecancer 8 441 / https://doi.org/10.3332/ecancer.2014.441
Activation of tumor specific T cells by AntigenPresenting Cells (APCs)
Antibody mechanism of action QIMR Berghofer Medical Research Institute 95
Targeting CTLA-4 and PD-1 to release thebrakes on T cellsLymph Node"inflammatory site” (tumor)Ribas A NEJM 2012
The Immune System Delves P and Roitt I, NEJM 2000
Targeting NK cells in cancer immunotherapyGuillerey C et al., Nat Immunol 2016
Charles Janeway’sImmunobiology text book . Trends in Immunology 2011 32, 364-372DOI: (10.1016/j.it.2011.06.001) Release of Cytokines Cytolysis. Major inhibitory and activating receptors on NK cells and their cognate ligand