Transcription
zHow to Conduct a Medical Record ReviewWHIT E PAPERSummary: This paper defines a recommended process for medical record review. This includesthe important first step of defining the “why” behind the review, and marrying the review outcometo organizational goals.F EAT UR E SAligning record reviews toorganizational goals. 2Principles of recordreview. 3ED/EMS notes. 5History and physical (H&P). 6Operative note or bedsideprocedures. 7Diagnostics and medications. 8Progress notes, consults, andnursing documentation. 9Initial vs. subsequentreviews. 9Documenting the review:capturing thought processesand critical thinking. 11Reconciliation with codeddata. 13Advanced techniques for matureCDI programs. 15The role of technology. 17Conclusion. 18References. 19Medical record review is perhaps the core responsibility of the CDI professional. Although the numbers vary by facility, CDI specialists review an average of16–24 patient charts daily, a task that compromises the bulk of their workday(ACDIS, 2016).1 During the review, CDI professionals comb the chart for incomplete, imprecise, illegible, conflicting, or absent documentation of diagnoses,procedures, and treatments, as well as supporting clinical indicators. Theirgoal is to cultivate a medical record that stands alone as an accurate story of apatient encounter, providing a full picture of the patient’s illness and record oftreatment. A complete record allows for continuity of care, reliable collection ofmortality and morbidity data, quality statistics, and accurate reimbursement.In their review of the medical record, CDI professionals aim to reconstruct thepatient story from admission to discharge by examining, understanding, andsynthesizing many puzzle pieces from disparate systems and people. Thisprocess requires considerable clinical acumen, critical thinking akin to detectivework, and knowledge of coding guidelines and quality measure requirements. In aworld with finite resources, it also requires an efficient, effective workflow.This paper defines a recommended process for medical record review. Thisincludes the important first step of defining the “why” behind the review, andmarrying the review outcome to organizational goals. The paper also describes arecommended step-by-step review process, starting with emergency departmentdocumentation and continuing to the history and physical, progress notes, andquery and follow-up. This paper defines and differentiates initial and subsequentreviews and offers suggestions for capturing not just physicians’ critical thinking,but that of the CDI specialists too. It also discusses reconciliation of coded data,advanced chart review techniques, and the present state of assistive technology.1. The majority (53%) of respondents to ACDIS’ 2016 CDI Productivity Survey indicated that they conduct6–10 new reviews each day, with 32% reporting that they conduct 11–15 new reviews each day. Surveyresults indicated an interesting split of daily re-reviews, with approximately one-third of respondentsconducting 6–10 re-reviews per day and one-third conducting 11–15 re-reviews per day.
How to Conduct a Medical Record ReviewAligning record reviews to organizational goalsToday, CDIhas evolved.It’s no longerfocused solelyon MS-DRGs,but takes aholistic viewof all aspectsof patientcomorbidities,including theimpact onreporting ofquality measuresand patientconditions.One of the greatest challenges to identifying an optimal, universal CDI recordreview process is contending with differing organizational CDI scopes of work.While this paper offers a standard review process, differing organizational endgoals may require different review emphases.Many CDI programs began with a goal of DRG optimization. Under this model,CDI specialists typically reviewed the record concurrent with the patient’s stay.Reviews terminated when the DRG was “optimized” with documentation of theappropriate principal diagnosis. Unfortunately, this approach could lead to busyclinicians missing or omitting comorbidities in the documentation, resulting in aninaccurate patient classification in the DRG system.Today, CDI has evolved. It’s no longer focused solely on MS-DRGs, but takesa holistic view of all aspects of patient comorbidities, including the impact onreporting of quality measures and patient conditions. In today’s model, CDIreviewers examine cases throughout an encounter and query for documentationof all comorbid conditions, regardless of whether the DRG has already beenoptimized. This model encourages providers to document all conditions beingmonitored and treated, thereby ensuring accurate reimbursement for MS-DRGpayers and helping prevent denials that stem from the removal of a sole CC/MCC. The model also allows for some risk adjustment that may impact APR-DRGpayers and specific quality reporting agency measures. CDI specialists operatingin APR-DRG environments typically review records and query for diagnoses thatimpact APR-DRG assignment and severity of illness (SOI) and risk of mortality(ROM) metrics, which drive payment and related quality measures. Programs thatreview Value-Based Purchasing quality measures focus on principal diagnosisassignment, and on diagnoses (primarily chronic conditions) that drive riskadjustment for these measures.Ultimately, CDI specialists should review all records, regardless of payer, toensure documentation integrity across all patient populations.CDI review processes may also focus on some combination of the followingobjectives:Patient Safety Indicators (PSI)Hospital-acquired conditions (HAC)Mortality risk: Observed vs. expected metricsSpecific populations (by payer, service line, primary diagnosis,mortalities)October 2018 2 2018 by HCPro an H3.Group brand, Any reproduction is strictly prohibited. For more information, call 877-233-8734 or visit www.acdis.org.
How to Conduct a Medical Record ReviewHierarchical Condition Categories (HCC)Readmissions and social determinants of healthLength of stay (LOS): Observed vs. expected metrics, which can also berisk-adjustedSetting a clear goal for CDI record review requires knowledge of reimbursement,quality measures, and other key targets. But it also requires understandingyour organization’s overall mission and goals. Without this concordance, aCDI program may find itself undervalued by hospital leadership or fail to meetorganizational needs. For example, initiating SOI/ROM-focused reviews whenhospital leadership is focused on Value-Based Purchasing metrics may result inoutcomes misaligned with institutional goals.A baseline CDIrecord reviewis a concurrentreview ofan inpatientmedical recordin which theCDI specialistattempts toabstract keyinformation forthe purposesof qualitymeasurement,compliantcoding, andappropriatereimbursement.Merging organizational goals with CDI workflows can be difficult, as it requiresaccess to leadership and negotiation with the competing interests of otherdepartments. As a result, programs often omit this essential step. However,successful alignment can ensure that the organization’s priorities are reflectedin the CDI program’s outcomes, granting the program and its work substantialadded value. Communication is key.Principles of record reviewA baseline CDI record review is a concurrent review of an inpatient medical recordin which the CDI specialist attempts to abstract key information for the purposesof quality measurement, compliant coding, and appropriate reimbursement.This process ensures that all conditions being monitored and treated during theencounter are appropriately identified in provider documentation.Quality measurement aspects of the review include capturingdocumentation that may need further clarification, require clinicalvalidation, or impact organizational quality measures, patient care andoutcomes, and public reporting.Compliant coding reviews identify diagnoses, conditions, and keyfindings that need further clarification for acuity (acute, subacute,chronic), specificity (type, degree, level), or clinical validation and/orsupport in order to be properly reported in coded data. This includespresent on admission (POA) status. During the review, CDI specialistsmust adhere to organizational bylaws, Uniform Hospital Discharge DataSet (UHDDS) guidelines, ICD-10-CM Official Guidelines for Coding andReporting, and internal documentation and coding policies.October 2018 3 2018 by HCPro an H3.Group brand, Any reproduction is strictly prohibited. For more information, call 877-233-8734 or visit www.acdis.org.
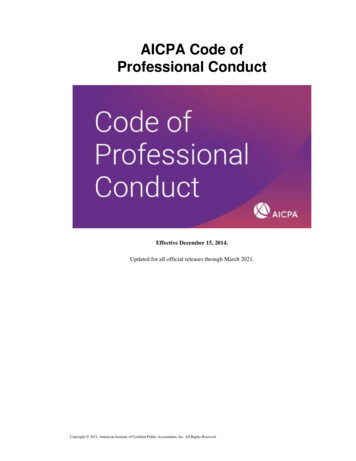
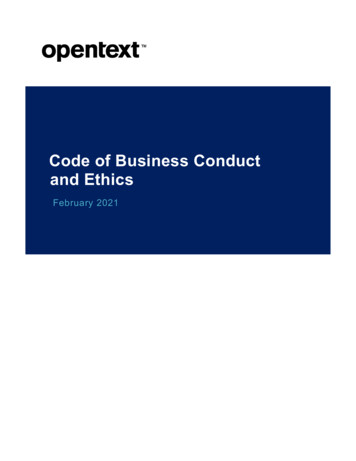
How to Conduct a Medical Record ReviewAppropriate reimbursement comes from the review’s capture ofseverity, clinical validation, coding accuracy, medical necessity, andquality outcomes.The record review should also track communication among CDI and codingprofessionals, if applicable, for efficiency, clarity, and understanding of the reviewand key findings (this topic is covered later in the paper).Concurrent CDI review captures the essence of the patient’s admission andarticulates the comorbid conditions being monitored and treated throughout theinpatient stay. During this process, the CDI specialist must clinically validate thestated conditions, querying for those conditions that are unstated but clinicallysupported, or stated but clinically unsupported.When should a record review begin? Typically, reviews begin 24–48 hours afteradmission and/or initial assessments are completed. A good rule of thumb isto review a record when there is enough information on which to base a query(e.g., after the history and physical is completed, and initial diagnostic testing isperformed).Following is an example of a chart review workflow:ED/EMSProgressNotesNursing/Ancillary NotesH&PDiagnostics/MedicationsQueryConsultsOR/ ProceduresFollow-up andFocusOctober 2018 4 2018 by HCPro an H3.Group brand, Any reproduction is strictly prohibited. For more information, call 877-233-8734 or visit www.acdis.org.
How to Conduct a Medical Record ReviewED/EMS notesThe process of record review begins with the emergency department (ED)notes, or notes from emergency medical services (EMS). Here, CDI specialistsencounter a great deal of clinical evidence for POA conditions, even if not initiallydocumented in the medical record. ED diagnoses may be final-coded, but like alldiagnoses, they must be clearly documented, be clinically supported, and meetthe UHDDS definition of a secondary diagnosis.Some of the elements that CDI specialists should consider in their review includethe following:Vitals—initial: Review the initial vital signs as these provide a baselineof medical necessity, clinical support and POA status for conditions, andevidence of disease processes (e.g., SIRS, sepsis, infections, respiratoryfailure). Compare initial and subsequent vital sign assessments forvariation. Note any therapeutic interventions that may impact the vitalsigns.Chief complaint: The chief complaint usually relates to the principaldiagnosis. Review for information from the patient or family thatmay indicate a potential disease or condition (e.g., encephalopathy,malnutrition, stroke). This information may shed light on confusion orbehavioral disturbances. Review nutrition status documentation forintake, fluid consumption, and any noted weight loss or gain over time. Inaddition, there may be documentation of a fall. If so, review to see howthe fall occurred, what the patient was doing prior, and where the falloccurred in order to capture coding specificity. Look for the underlyingcondition causing the fall, if appropriate. Seek to identify causative factorsand relationships among medical conditions that support identification ofthe principal diagnosis.Relevant physical findings: Obtain diagnosis validation via assessmentof the clinical findings that support the conditions being monitored andtreated. Common findings are for pressure injuries, respiratory failure,and malnutrition. Be vigilant for contradictory findings (e.g., diagnosis ofsepsis with a general description of “non-toxic”).Relevant past medical history: Capture appropriate chronic conditionsthat are relevant to this admission. Review the medications on admissionand verify the corresponding diagnosis. If the patient presented onantibiotics or another ongoing treatment, is there documentation ofa corresponding condition (e.g., urinary tract infection, pneumonia)?Review for recent surgeries, procedures, or complications that may haveOctober 2018 5 2018 by HCPro an H3.Group brand, Any reproduction is strictly prohibited. For more information, call 877-233-8734 or visit www.acdis.org.
How to Conduct a Medical Record Reviewcontributed to the admission. Identify if the patient has a DNR or palliativecare status.The H&Pprovides conciseinformationregardinga patient’shistory andexam findingsat the time ofadmission.In addition, itoutlines the planfor addressingthe issues thatprompted theadmission.POA status of devices or ostomies: Review for documentation ofthe presence and condition of all devices and ostomy sites. Are therepossible complications, a recent surgery, or conditions still being treated(cancer, infections, etc.)? Is there potential for a patient safety issue(PSI)?Confusion/altered mental status/skin ulcers: Are these conditionspresent, and is there a corresponding diagnosis?Assessment/medical decision-making: Read the chart and understandthe story. This may reveal differential diagnoses that require clarificationin the documentation.Diagnosis/impression: Review for medical necessity and accuracy ofdocumented diagnoses for appropriate capture in final coding. Do theconditions relate to the admission diagnosis?History and phys
Medical record review is perhaps the core responsibility of the CDI profession-al. Although the numbers vary by facility, CDI specialists review an average of 16–24 patient charts daily, a task that compromises the bulk of their workday 1 During the review, CDI professionals comb the chart for incom-plete, imprecise, illegible, conflicting, or absent documentation of diagnoses, procedures .