Transcription
WHITE PAPERIHI Psychology of ChangeFrameworkto Advance and Sustain Improvement[Grab your reader’s attention with a greatquote from the document or use this space toemphasize a key point. To place this text boxanywhere on the page, just drag it.]AN IHI RESOURCE53 State Street, 19th Floor, Boston, MA 02109 ihi.orgHow to Cite This Document: Hilton K, Anderson A. IHI Psychology of Change Framework to Advance and Sustain Improvement. IHIWhite Paper. Boston, Massachusetts: Institute for Healthcare Improvement; 2018. (Available at ihi.org)
AUTHORS:Kate Hilton, JD, MTS: Faculty, IHIAlex Anderson: Research Associate, IHIAcknowledgments:The authors are grateful to Helen Bevan, Becky Margiotta, Kedar Mate, Kara McElvaine, Frances Olajide, Kathryn Perera,Jessica Perlo, and Hanna Sherman for refining the theory; to Neil Baker, Karen Baldoza, Mike Briddon, Pedro Delgado,Becka DeSmidt, Christina Gunther-Murphy, Paul Howard, Teaka Isaac, Niñon Lewis, Allison Luke, Marianne McPherson,Santiago Narino, Linson Naval, Leslie Pelton, Kathryn Perera, Amy Reid, Cory Sevin, Hanna Sherman, Valerie Spaulding,and Trissa Torres for testing the model; to Barbara Balik, Donald Berwick, Maureen Bisognano, Marshall Ganz, DonGoldmann, Bob Klaber, Becky Margiotta, Kedar Mate, Joe McCannon, Santiago Narino, Tyler Norris, Carlos Pelligrini,Kathryn Perera, Jessica Perlo, Michael Rose, Jonathan Scaccia, Hanna Sherman, Matthew Stiefel, Nana Twum-Danso, andDavid Williams for reviewing the white paper; and to Jane Roessner and Val Weber for editing the white paper. We are alsograteful to those interviewed and not already mentioned, including Nisreen Haj Ahmad, David Fleisher, Hahrie Han, DanHeath, Hunter Guhlbach, Christopher Lawrence-Pietroni, Ziva Mann, Katy Milkman, Michelle Molitor, Tom Nolan,Kathryn Segovia, Rebecca Steinfeld, and Robert Sutton.The Institute for Healthcare Improvement (IHI) is a leading innovator in health and health care improvement worldwide. For more than 25 years, we havepartnered with visionaries, leaders, and frontline practitioners around the globe to spark bold, inventive ways to improve the health of individuals andpopulations. Recognized as an innovator, convener, trustworthy partner, and driver of results, we are the first place to turn for expertise, help, andencouragement for anyone, anywhere who wants to change health and health care profoundly for the better. The ideas and findings in these whitepapers represent innovative work by IHI and organizations with whom we collaborate. Our white papers are designed to share the problems IHI isworking to address, the ideas we are developing and testing to help organizations make breakthrough improvements, and early results where they exist.Copyright 2018 Institute for Healthcare Improvement. All rights reserved. Individuals may photocopy these materials for educational, not-for-profit uses, provided that thecontents are not altered in any way and that proper attribution is given to IHI as the source of the content. These materials may not be reproduced for commercial, for-profit use inany form or by any means, or republished under any circumstances, without the written permission of the Institute for Healthcare Improvement.
WHITE PAPER : IHI Psychology of Change Framework to Advance and Sustain ImprovementContentsExecutive Summary4The Human Side of Change5What Is the Psychology of Change?6Methodology6IHI Psychology of Change Framework: Activating People’s Agency7Power: The Ability to Act with Purpose7Courage: The Emotional Resources to Choose to Act in the Face of Challenge81. Unleash Intrinsic Motivation92. Co-Design People-Driven Change123. Co-Produce in Authentic Relationship154. Distribute Power195. Adapt in tute for Healthcare Improvement ihi.org3
WHITE PAPER : IHI Psychology of Change Framework to Advance and Sustain ImprovementExecutive SummaryThis white paper is a guide for all leaders interested in understanding the underlying psychology ofchange and leveraging its power to impact quality improvement efforts: to achieve breakthroughresults, sustainably, at scale. Improvement science has given health care improvers a theoreticalframework and the applied technical skills to understand variation, study systems, build learning,and determine the best evidence-based interventions (“what”) and implementation strategies(“how”) to achieve the desired outcomes. Yet, health care improvers worldwide still struggle withthe adaptive side of change, which relates to unleashing the power of people (“who”) and theirmotivations (“why”) to advance and sustain improvement — two commonly cited reasons for thefailure of improvement initiatives.The paper presents a framework and set of methods for the psychology of change — fiveinterrelated domains of practice that organizations can use to advance and sustain improvement: Unleash Intrinsic Motivation; Co-Design People-Driven Change; Co-Produce in Authentic Relationship; Distribute Power; and Adapt in Action.Building on the legacies of W. Edwards Deming, Everett Rogers, and many others, a renewed focuson the human side of change increases the likelihood that efforts to improve health and health carewill succeed in the short term and be scaled and sustained over time.Institute for Healthcare Improvement ihi.org4
WHITE PAPER : IHI Psychology of Change Framework to Advance and Sustain ImprovementThe Human Side of ChangeAlthough there are impressive examples of successful improvements and remarkable outcomes inhealth care systems all over the world, the challenge of achieving results in our health systems andcommunities, let alone at scale, remains persistent. There is a substantial gulf between what weknow and what we do in practice. Countless evidence-based improvements and innovations acrosshealth disciplines take years to be adopted, or do not become common practice due to low rates ofadoption and sustainability.1The rate at whichimprovementsspread relies atleast in part onpeople.The rate at which improvements spread relies at least in part on the people who are implementing,spreading, and communicating about the change in practice. In his book, Diffusion of Innovations,Everett Rogers posited that an innovation must be widely adopted in order to become selfsustaining. Within the rate of adoption, there is a point at which an innovation reaches criticalmass. Rogers defines five categories of adopters: innovators, early adopters, early majority, latemajority, and laggards (recently called “traditionalists”).2 Diffusion manifests itself in differentways and is highly subject to the type of adopters and their process for engaging others to adopt theinnovation.Improvement thought leader W. Edwards Deming addressed this by stressing the importance ofpsychology — the adaptive, human side of change — in his System of Profound Knowledge, inwhich he distilled the body of information and skills that can be brought to bear on anyimprovement into four interrelated areas: appreciation for a system, knowledge of variation,theory of knowledge, and psychology.3 Psychology, in Deming’s definition, is the way people thinkand feel, what motivates them, what demotivates them, the problematic effects of incentives, andhow they behave — including when they encounter change. Dr. Deming acknowledged that allimprovement occurs in human systems, in which people interact with each other. Herecommended that for improvement to succeed, leaders need to understand and master the broadarea of psychology and interpersonal relationships. He understood that people are thefundamental source of value, and that it takes work and expertise to create a culture that respectsand motivates them.Most quality improvement projects require people to take new approaches to both technical andadaptive challenges. Technical challenges are clearly defined, can be solved by experts orcompliance to authorities, and can achieve gains in short time frames. Adaptive challenges areharder to identify, must be solved by the people affected by the problem, and require more time toachieve outcomes.4 For example, administering medication to lower blood pressure is a technicalapproach, whereas inviting patients to change their lifestyles and diets is an adaptive one. Adaptivechange relies on people’s commitment to adopt new attitudes, competencies, beliefs, andbehaviors. Among other things, Ronald Heifetz, founder of the Center for Public Leadership at theHarvard Kennedy School, recommends that leaders dealing with adaptive change “pinpoint howvalue systems or methods of collaboration need to change,” “give work back to people, to defineand solve problems,” and “regulate the inevitable distress that adaptive work generates — sincepeople resist change.”5Improvement leaders frequently experience resistance. There are many good reasons why peopleresist change: fear of losing control, excess uncertainty, unease with surprise, and fear ofthreatening one’s way of doing things.6 Resistance is the judgment made by the brain that theproposal for change threatens what people are currently doing. Practically, resistance comes in theform of emotions or behaviors meant to impede being changed. People demonstrate it as apathy,hopelessness, complacency, self-doubt, outright rejection, and, most of all, fear. It can also takeInstitute for Healthcare Improvement ihi.org5
WHITE PAPER : IHI Psychology of Change Framework to Advance and Sustain Improvementmore subtle forms such as publicly acting in accordance while privately disagreeing, especially incompliance-based settings. And it can come from many sources, from senior leaders who resist theprovision of resources for improvement to occur, to frontline staff and patients who resistimprovements that require changes in behavior.What are the implications for health care leaders and improvers? As the health care workforceadjusts to growing workloads, changing technologies, and complex processes for delivering care,improvements in quality and safety are increasingly viewed as both necessary and burdensome.From managing the tension between the pace of improvement and the urgency of political pressureand financial stress, to engrained organizational culture that stops improvement in its tracks, toconnecting top-level leaders to those with lived experience at the point of care, to decreasingclinician burnout, to the co-production of health with patients and communities — the test ofeffective health system leadership is how many people are motivated to achieve and sustain betterresults at scale.7Fortunately, improvement leaders can learn and apply principles and tools from many disciplinesrelated to the psychology of change to do just that. Building on the legacies of Deming, Rogers, andmany others, a renewed focus on the human side of change increases the likelihood that efforts toimprove health and health care will succeed in the short term and be scaled and sustainedover time.What Is the Psychology of Change?Psychology ofchange: thescience and art ofhuman behavioras it relates totransformation.Psychology is defined as the science of the mind and human behavior, especially as a function ofawareness, feeling, or motivation. The definition of change is to cause to be different, or totransform. Put together, the psychology of change is the science and art of human behavior as itrelates to transformation.First and foremost, the IHI Psychology of Change Framework is an approach to advancing andsustaining improvement together with the people directly and indirectly affected by it — thoseworking in our health systems, patients and families, community members, policymakers, andothers. The framework emphasizes the inherent value of each person, regardless of his or heridentity or position in an organization. It also recognizes the importance of identifying the ways inwhich all persons affected by the improvement can meaningfully contribute to the solution. Theframework acknowledges that people act according to their unique identities, while, at the sametime, adhering to many predictable human behaviors.MethodologyIn 2017, IHI’s innovation team began exploring the psychology of change, and a research team setout to understand the potential use of adaptive tools from many related disciplines for increasingthe success and sustainability of improvement projects. The team reviewed the literature(including academic and professional journals as well as popular books and papers) and conductedinterviews with experts in a wide variety of relevant subjects. This information was synthesized in aseries of internal reports and eventually led to the development of the IHI Psychology of ChangeFramework.Institute for Healthcare Improvement ihi.org6
WHITE PAPER : IHI Psychology of Change Framework to Advance and Sustain ImprovementIHI’s framework results from a crosswalk of hundreds of tools and frameworks from manydisciplines and applied methodologies. Given its broad scope, the IHI Psychology of ChangeFramework is not exhaustive. The framework attempts to provide a useful summary of some of themany disciplines to advance improvement science and outcomes, such as psychology andsociology, as well as applied methodologies, such as change management, organizing, designthinking, adaptive leadership, scaling up, team building, and others. Many scholars andpractitioners have dedicated their careers to specific niches within these fields; readers areencouraged to explore them further to deepen practice and learning.The framework is grounded in a social theory of learning and recognizes that transformationrequires individual and interpersonal changes in thinking, feeling, and acting, along with systemlevel changes in structures, processes, and conditions. At its core, it invites people to engage theirhead, heart, and hands in its conceptual, motivational, and practical dimensions. It definesconcepts; offers examples; provides summaries of tools applied across social, self-authoring, andself-transforming stages of adult development; and recommends experiential practice, reflection,and discovery. The framework will evolve as research continues and feedback is received. IHIinvites improvement leaders to test and share learning in the continued development of the theory,tools, and measures.IHI Psychology of Change Framework:Activating People’s AgencyActivatingpeople’s agency Power (the abilityto act withpurpose) Courage (theemotionalresources tochoose to act inthe face ofdifficulty oruncertainty)Activating people’s agency is the central objective of the IHI Psychology of Change Framework.Activate means to make active or more active, or to convert from inactive to active. Agency isdefined as the ability of an individual or group to choose to act with purpose. Agency has two keycomponents: 1) power, or the ability to act with purpose; and 2) courage, or the emotionalresources to choose to act in the face of difficulty or uncertainty. Together, courage and power arethe primary drivers for activating people’s agency, or the ability of an individual or group to chooseto act with purpose.Imagine, for example, a hospital postoperative surgical unit that has a high rate of avoidablepatient falls. A unit staff nurse has ideas about how to prevent falls, but he is responsible for manyspecific tasks and has little time to change the standard work on the unit. He views his power — hisability to act to prevent falls — as limited; he does not believe that he has the requisite skills toinitiate an improvement project. Moreover, he fears punishment: he believes from previousexperience that working outside of the unit’s standard practices can result in disciplinary action.His willingness to choose to act to prevent falls is minimal; his courage is constrained by theorganization’s operational norms. To engage in meaningful improvement and advance a processfor change, leaders need to identify ways to activate the staff nurse’s agency — both his power andhis courage — to result in the mindful choice to act.Power: The Ability to Act with PurposePower is not a position or title that a person has within an organization; it’s not a thing, quality, ortrait. Power is relational; it is produced by a set of interdependent relationships that can beleveraged to achieve a specified aim. Power is generated as people bring to bear their skills,knowledge, experience, and capacity to act, individually and together, to achieve an aim.Institute for Healthcare Improvement ihi.org7
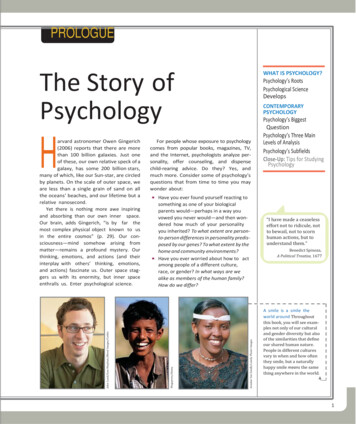
WHITE PAPER : IHI Psychology of Change Framework to Advance and Sustain ImprovementCourage: The Emotional Resources to Choose to Act in theFace of ChallengeEducator ParkerPalmer explainsthat the source ofcourage is inknowingourselves,creatingcircumstances inwhich others canbecome more selfaware and selfknowing, andbeing inrelationship withwhat is happeningaround us.The root of the word courage is “cor,” the Latin word for heart. Courage comes from people’semotional resources for mindful choice to act in the face of challenge.8 Educator Parker Palmerexplains that the source of courage is in knowing ourselves, creating circumstances in which otherscan become more self-aware and self-knowing, and being in relationship with what is happeningaround us.9The IHI Psychology of Change Framework is centered on activating agency at three levels: Self: An individual’s agency to make his or her own choices. People feel an increased sense ofagency when they exercise their power and courage to take action. 10 Interpersonal: The collective agency of people acting together. People feel an increasedsense of agency when they encounter positive experiences of other people exercising powerand courage.11 System: The structures, processes, and conditions that support the exercise of agency withinand across institutions and organizations. People feel an increased sense of agency when thestructures within which they operate enable them to exercise their power and courage. 12This is the objective in the IHI Psychology of Change Framework: to create the conditions thatenable individuals and groups across systems to exercise power and courage (i.e., to choose to actwith purpose) in order to advance and sustain improvements in health and health care. Toestablish these conditions, the framework is organized around five interrelated domains of practice(see Figure 1).Figure 1. IHI Psychology of Change FrameworkInstitute for Healthcare Improvement ihi.org8
WHITE PAPER : IHI Psychology of Change Framework to Advance and Sustain Improvement1.Unleash Intrinsic Motivation: Tapping into sources of intrinsic motivation galvanizespeople’s individual and collective commitment to act.2. Co-Design People-Driven Change: Those most affected by change have the greatestinterest in designing it in ways that are meaningful and workable to them.3. Co-Produce in Authentic Relationship: Change is co-produced when people inquire,listen, see, and commit to one another.4. Distribute Power: People can contribute their unique assets to bring about change whenpower is shared.5.Adapt in Action: Acting can be a motivational experience for people to learn and iterate tobe effective.These five domains are not meant to be sequential; rather, they are interrelated and can beengaged in many ways, in any order. The effective use of these practices to activate people’s agencycan and should be measured (see more in the Measurement section below).The five domains are described in more detail below, including summaries of high-leverage tools toapply the concepts in an improvement context. In practice, each tool relates to all five domains.1. Unleash Intrinsic MotivationWhat does it mean to unleash intrinsic motivation? Becky Margiotta and Joe McCannon, largescale change leaders who co-founded the Billions Institute, define unleashing as “orchestratingthe loss of control of people moving in the desired direction.”13 This involves an inherent tension offacilitating and guiding while losing control, as many people bring forward their energy andcreativity to advance a shared cause.Clinical and social psychologists Richard Ryan and Edward Deci define intrinsic motivation as“doing something for the inherent satisfaction that engaging in the activity provides.”14 (Incontrast, extrinsic motivation means doing something because it leads to a separate outcome likereward, recognition, or avoidance of punishment.) Put together, unleashing intrinsicmotivation means creating the conditions for many people to carry forward a shared cause on thebasis of the inherent value that one experiences in the activity.Deming likewise believed that improvers must move from systems driven by fear and extrinsicmotivation to those driven by intrinsic motivation.15 Influenced by Alfie Kohn, author of Punishedby Rewards, Deming rejected management by carrot-and-stick rewards, as well as other commonpractices such as quotas and merit ratings, which seek to affix blame and reward to individuals. Intheir place, Deming focused on motivations that arise from an environment of trust, relationships,interdependence, and pride in work.Deming understood what psychologists Deci and Ryan and social scientists Richard Hackman andGreg Oldham show: intrinsic motivation generates creativity, engagement, adaptive learning, andachievement. Hackman and Oldham demonstrate that tasks designed to draw on intrinsic sourcesof motivation produce greater commitment than those associated with extrinsic rewards. Theconditions for motivational task design include an experience of meaningfulness (the task isimportant to the overarching purpose), responsibility (how well the task gets done is up to me),and results (as I do the work, I can see whether or not I am doing it well).16 (All are premised onpsychological safety, discussed later in the white paper.) These intrinsic motivators are generativeand sustainable sources of commitment for advancing and sustaining improvement.Institute for Healthcare Improvement ihi.org9
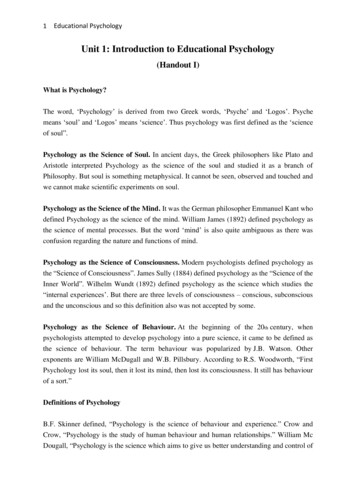
WHITE PAPER : IHI Psychology of Change Framework to Advance and Sustain ImprovementUnleash IntrinsicMotivation:Tapping intosources l andcollectivecommitmentto act.To unleash intrinsic motivation, it is important for improvers to understand what matters to otherpeople — individually, as related to the people they care about, and across society as a whole. Whenwhat matters to people is embraced and honored as part of the improvement work, it limits thefears associated with change because people are more likely to see and experience the fundamentalvalue of change. In a 2012 article, Michael Barry and Susan Edgman-Levitan introduced the idea ofasking patients, “What matters to you?” as well as, “What is the matter?” in the context ofimplementing shared decision making.17 Their ambition was to increase clinicians’ awareness ofimportant issues in patients’ lives that could drive customized plans of care. Maureen Bisognano,IHI President Emerita and a champion of the “What matters to you?” concept in health care,argues that eliciting a patient’s goals, preferences, hopes, and dreams is essential to flip the focusfrom treating disease to co-producing health because it activates people’s intrinsic motivations forbeing healthy.The same lesson applies in improvement work. Leaders of improvement cannot assume that thereasons they believe a change will be an improvement apply to other people and their perspectives.Instead, improvement leaders can ask each member of an improvement effort what matters tothem so that those affected by the change can articulate why the change is, or is not, valuable fromtheir perspective.18 The leader’s task is not to judge the source of the motivation, but rather toenable people to access this motivation, over and over, to advance and sustain improvement.How to Unleash Intrinsic MotivationThere are many methods to unleash intrinsic motivation. Here we present an overview of publicnarrative, motivational task design, and play and celebration, underutilized but high-leverage toolsin improvement contexts. Use Public NarrativeDeveloped by Marshall Ganz, public narrative provides a practical approach to identifying andunleashing intrinsic motivation (see Figure 2).Figure 2. Public NarrativeSource: Ganz M. What Is Public Narrative: Self, Us & Now (Public Narrative Worksheet).21 Adapted with permission.Institute for Healthcare Improvement ihi.org10
WHITE PAPER : IHI Psychology of Change Framework to Advance and Sustain ImprovementPublic narrative includes three elements:19 A story of self: Personal stories that can access the emotional resources embedded in ourvalues that can enable mindful action; A story of us: Collective stories that can access the emotional resources embedded in thevalues shared by the group of people engaged in action; and A story of now: Stories that transform the present moment into a narrative moment in whichwe are confronted by an urgent challenge, access sources of hope, and respond mindfully(instead of reacting fearfully).Taken together, these three narrative threads establish a foundation within which an individual,team, or organization can lead on the basis of individual motivating values (stories of self),collaborate on the basis of shared values (stories of us), and access sources of courage to respondmindfully to an urgent challenge, as opposed to reacting to it (stories of now). These storiescommunicate the intrinsic motivations that propel improvement efforts, such as dignity andrespect, fairness and equality, justice and safety, and love and kindness.For instance, anesthesiologist Dr. Michael Rose drew on public narrative to unleash intrinsicmotivation for the widespread adoption of an evidence-based surgical safety checklist at McLeodRegional Medical Center in Florence, South Carolina. For 18 months prior, adoption rates hadhovered at 30 percent despite efforts to raise awareness, train, market, convince, cajole, and evenmandate the use of the checklist. To unleash intrinsic motivation, Dr. Rose convened surgical teammembers to share what called them to enter the health care profession and care for patients. Teammembers shared stories of self: loved ones who experienced harm in hospitals, or injustices inhealth care. They described personal trials as children of elderly parents, as spouses, as parents ofyoung children. They shared universal moments of grief and loss, or of people who had helpedthem through profoundly uncertain moments — and how those people and moments transformedthem as human beings and professionals.Through these stories, surgical staff connected to each other and their intrinsic motivations aroundpatient care. Some described that they were hearing about each other’s motivations to do the workthat they do for the first time, despite having worked together for more than 25 years. Dr. Rose andhis team then built a story of us and now, as they shared how the improvement work brought themall closer to what drew them to medicine: to care for people, safely and justly. They contrasted theurgent challenge of patient harm with hopeful stories about patients with improved surgicaloutcomes as a result of using the checklist and the positive effects for patients’ families, employers,the broader community, and hospital staff. The results followed: 100 percent sustained utilizationof the checklist, 35 percent decrease in mortality, and a reduction of 80,000 hours of annualresource time due to improved performance.20 In addition, surgical team members reportedimproved safety culture measures, increased job satisfaction, and decreased burnout.Improvement leaders create the space to elicit these stories. It is in sharing them that we revealwho we are as leaders and remind people (ourselves included) why we care — which, in animprovement context, motivates others to make hopeful, intentional choices to adopt and sustainimprovement efforts. For instance, many boards of trustees and other health system committeesstart meetings with stories from patients, families, or staff members. Stories enable agency byeliciting people’s emotions, feelings of urgency, anger at injustice, hope, solidarity, and the sensethat they can make a difference. Action motivators help people overcome inhibitors such asInstitute for Healthcare Improvement ihi.org11
WHITE PAPER : IHI Psychology of Change Framework to Advance and Sustain Improvementfeelings of inertia, apathy, fear, isolation, and self-doubt.21 Emotions motivate people to act,serving as a source of courage, especially in moments of difficulty or uncertainty, which in turnenables people to exercise power (the ability to act with purpose). Integrate Motivational Task Design into ImprovementDeveloped by Richard Hackman and Greg Oldham, motivational task design focuses on designingthe tasks involved in an improvement effort in ways that generate people’s intrinsic motivationsand sustain their commitment. This method enables improvers to design meaningful actionswhereby people see their effort tied to a valuable outcome, with the responsibility and freedomto make decisions (instead of being told what to do), alongside opportunities for feedback andlearning.22Hackman and Oldham identify five design criteria to build into motivational tasks: 1) actionidentity: the action can be completed from start to finish; 2) action significance: the action makes adifference and contributes to a larger goal; 3) skill variety: the action requires many skills and isnot repetitive and boring; 4) autonomy: the actors have the freedom to choose their approach; and5) feedback: the results are accessible and can be used to identify improvements going forward.When improvement leaders design actions to maximize these criteria, people experience threepsychological states: meaningfulness of the work, responsibility for the outcomes, and knowledgeof the actual results.
What Is the Psychology of Change? 6 Methodology 6 IHI Psychology of Change Framework: Activating People’s Agency 7 Power: The Ability to Act with Purpose 7 Courage: The Emotional Resources to Choose to Act in the Face of Challenge 8 1. Unleash Intrinsic Motivation 9 2. Co-Design People-Dri