Transcription
PsychologicalDisordersChapter 13
Psychological Disorders (1 of 6) Module 13.1 What Is Abnormal Behavior? Identify criteria used to distinguish normal behavior from abnormal behavior, andapply these criteria to the case examples of Claire and Phil. Identify the major contemporary models of abnormal behavior. Describe the features of psychological disorders and explain how they are classifiedin the DSM system. Module 13.2 Anxiety-Related Disorders Module 13.3 Dissociative and Somatic Symptom and Related Disorders Module 13.4 Mood Disorders Module 13.5 Schizophrenia Module 13.6 Personality DisordersJeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
Module 13.1 What IsAbnormal Behavior?Jeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
CulturalBases ofAbnormalBehaviorJeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
Models ofAbnormalBehaviorJeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
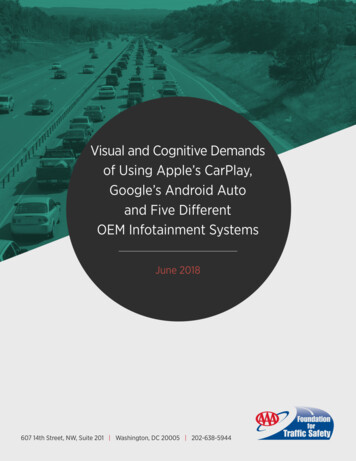
The Diathesis-Stress ModelFIGURE 13.1Jeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
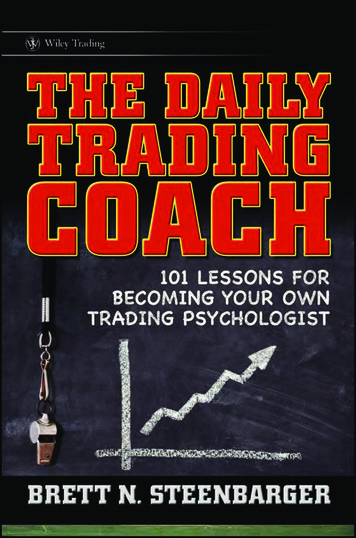
How Common arePsychological Disorders? Prevalence of PsychologicalDisorders FIGURE 13.2Jeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
Overview: Contemporary Models of Abnormal Behavior (1 of2) CONCEPT CHART 13.1ModelPsychological ModelsPsychological ModelsPsychological ModelsPsychodynamicmodelFocusKey QuestionsUnconscious conflicts andmotives underlying abnormalbehaviorHow do particular symptoms represent or symbolizeunconscious conflicts?Behavioral modelLearning experiences that shapethe development of abnormalbehaviorHow are abnormal patterns of behavior learned? What roledoes the environment play in explaining abnormalbehavior?Humanistic modelRoadblocks to self-awarenessand self-acceptanceHow do a person’s emotional problems reflect a distortedself-image?What are the childhood roots of a person’s problem?What roadblocks did the person encounter in the pathtowards self-realization?Psychological ModelsCognitive modelFaulty thinking underlyingabnormal behaviorWhat styles of thinking characterize people with particulartypes of psychological disorders?What roles do personal beliefs, thoughts, and ways ofinterpreting events play in the development of abnormalbehavior patterns?
Overview: Contemporary Models of Abnormal Behavior (2of 2) CONCEPT CHART 13.1ModelFocusKey QuestionsMedical modelBiological underpinnings of abnormalbehaviorWhat roles do neurotransmitters, genetics, and brain abnormalitiesplay in abnormal behavior?Sociocultural modelSocial ills contributing to the developmentof abnormal behavior, such as poverty,racism, and prolonged unemployment;relationships between abnormal behaviorand ethnicity, gender, culture, andsocioeconomic levelWhat relationships exist between social class status and risks ofpsychological disorders?Interactions of biological, psychological,and sociocultural factors in thedevelopment of abnormal behaviorHow might genetic or other factors predispose individuals topsychological disorders in the face of life stress?Biopsychosocial modelAre there gender or ethnic group differences in various disorders?How are these explained?What are the effects of stigmatization on people who are labeledmentally ill?How do biological, psychological, and sociocultural factors interactin the development of complex patterns of abnormal behavior?
Psychological Disorders (2 of 6) Module 13.1 What Is Abnormal Behavior? Module 13.2 Anxiety-Related Disorders Identify and describe types of anxiety-related disorders andunderlying causal factors in these disorders. Module 13.3 Dissociative and Somatic Symptom and RelatedDisorders Module 13.4 Mood Disorders Module 13.5 Schizophrenia Module 13.6 Personality DisordersJeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
Module 13.2 AnxietyRelated DisordersJeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
AnxietyRelatedDisordersJeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
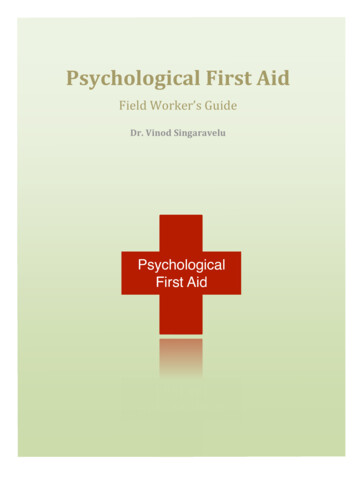
Cognitive Model of PanicFIGURE 13.3Jeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
Overview: Anxiety-Related Disorders CONCEPT CHART 13.2Type of DisorderLifetime Prevalence inPopulation (approximate)SymptomsAssociated FeaturesAgoraphobia1.4% to 2%Fear and avoidance of publicplacesThis generally develops secondarily to panic disorder, as theperson attempts to avoid situations in which attacks have occurredor in which help might be unavailable in the event of an attack.Panic disorder5.1%Repeated panic attacksaccompanied by persistentconcern about future attacksPanic attacks have strong physiological symptoms; beginningattacks occur without warning; this disorder may be accompaniedby agoraphobia.Generalizedanxiety disorder5.7%Persistent, excessive levels ofanxiety and worryAnxiety has a free-floating quality in that it is not tied to particularobjects or situations.Specific phobia12.5%Fear and avoidance of a specificobject or situationAvoidance of the phobic object or situation is negatively reinforcedby relief from anxiety.Social anxietydisorder12.1%Fear and avoidance of socialsituations or performancesituationsThis involves underlying fear of rejection, humiliation, orembarrassment in social situations.Obsessivecompulsivedisorder2% to 3%Recurrent obsessions and/orcompulsionsA repetitive cycle may ensue in which obsessive thoughtsengender anxiety that, in turn, is partially relieved (negativelyreinforced) by performing the compulsive ritual. Sources: Prevalence data based on American Psychiatric Association, 2013; Conway et al, 2006; Blanco et al., 2006; Grant, Hasin,Stinson et al., 2006; Kessler, Berglund, et al, 2005; Kessler, Chiu, et al., 2015; Stein & Sareen, 2015
Psychological Disorders (3 of 6) Module 13.1 What Is Abnormal Behavior? Module 13.2 Anxiety-Related Disorders Module 13.3 Dissociative and Somatic Symptom and Related Disorders Identify and describe types of dissociative and somatic symptomand related disorders and underlying causal factors in thesedisorders. Module 13.4 Mood Disorders Module 13.5 Schizophrenia Module 13.6 Personality DisordersJeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
Module 13.3Dissociative andSomatic Symptom andRelated DisordersJeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
DissociativeDisordersand TheirCausesJeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
SomaticSymptomand RelatedDisordersJeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
Overview: Dissociative and Somatic Symptom and RelatedDisorders CONCEPT CHART 13.3Type of DisorderLifetime PrevalenceFeaturesCommentsDissociative identitydisorderRareMultiple personalities emerge within thesame individualMay represent a type of psychologicaldefense against trauma or unbearableabuse from childhoodDissociativeamnesiaRareMemory loss that cannot be explainedas the result of head trauma or otherphysical causeTypically involves loss of memoriesassociated with specific traumatic eventsConversion disorderRare, but is reported in 5% ofpatients referred to neurologyclinicsA loss or change of physical functionthat cannot be explained by a medicalconditionMay have been much more common inFreud’s day than in our ownSomatic symptomdisorderUnknown, but may affectbetween 5% and 7% of thegeneral populationExcessive concerns about one’sphysical symptoms to the point that itsignificantly interferes with one’sthoughts, feelings, or behaviors in dailylifeMay have features similar to those ofanxiety-related disorders Sources: Prevalence data based on American Psychiatric Association, 2013
Psychological Disorders (4 of 6) Module 13.1 What Is Abnormal Behavior? Module 13.2 Anxiety-Related Disorders Module 13.3 Dissociative and Somatic Symptom and Related Disorders Module 13.4 Mood Disorders Identify and describe types of mood disorders and underlying causalfactors in these disorders. Identify factors linked to risk of suicide. Module 13.5 Schizophrenia Module 13.6 Personality DisordersJeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
Module 13.4 MoodDisordersJeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
Types ofMoodDisordersJeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
Cognitive Factors in Depression (1 of 2) TABLE 13.1 Cognitive Distortions Linked to DepressionType of g thinkingViewing events in black or white terms, as either all good or allbadDo you view a relationship that ended as a totalfailure, or are you able to see some benefits inthe relationship?Do you consider any less-than-perfect performanceas a total failure?Misplaced blameTendency to blame or criticize yourself for disappointments orsetbacks while ignoringexternal circumstancesDo you automatically assume that it’s your fault when thingsdon’t go as planned?Misfortune tellingTendency to think that one disappointment will inevitably lead toanotherIf you get a rejection letter from a job you applied for, do youassume that all the other applications you sent will meet thesame fate?Negative focusingFocusing your attention only on the negative aspectsof your experiencesWhen you get a job evaluation, do you overlook the praise andfocus only on the criticism?Dismissing the positivesSnatching defeat from the jaws of victory by trivializing ordenying your accomplishments; minimizing your strengths orassetsWhen someone compliments you, do you findsome way of dismissing it by saying something like, “it’s no bigdeal” or “anyone could have done it”? Source: Adapted from Burns, 1980; Nevid & Rathus, 2010; Nevid, Rathus, & Greene, 2014
Cognitive Factors in Depression (2 of 2) TABLE 13.1 Cognitive Distortions Linked to DepressionType of CognitiveDistortionDescriptionExampleJumping to conclusionsDrawing a conclusion that is not supported by the facts at handDo you usually or always expect the worst to happen?CatastrophizingExaggerating the importance of negative events or personalflaws (making mountains out of molehills)Do you react to a disappointing grade on a particularexamination as though your whole life is ruined?Emotion-based reasoningReasoning based on your emotions rather than on a clearheaded evaluation of the available evidenceDo you think that things are really hopeless because it feels thatway?ShouldismsPlacing unrealistic demands on yourself that you should or mustaccomplish certain tasks or reach certain goalsDo you feel that you should be further along in your life than youare now?Do you feel you must ace this course or else? (Not that itwouldn't be desirable to ace the course, but is it really that youmust?)Name-callingAttaching negative labels to yourself or others as a way ofexplaining your own or others’ behaviorDo you label yourself as lazy or stupid when you fall short ofreaching your goals?Mistaken responsibilityAssuming that you are the cause of other people’s problemsDo you automatically assume that your partner is depressed orupset because of something you said or did (or didn’t say ordo)? Source: Adapted from Burns, 1980; Nevid & Rathus, 2010; Nevid, Rathus, & Greene, 2014
SuicideJeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
Common Myths about Suicide TABLE 13.2 Myths About SuicideMythFactPeople who threaten suicide are only seekingattention.Not so. People who go on to commit suicide often give clear clues concerning theirintentions, such as disposing of their possessions or suddenly making arrangementsfor a burial plot.A person must be insane to attempt suicide.Most people who attempt suicide may feel hopeless, but they are not insane (that is,out of touch with reality).Talking about suicide with a person withdepression may prompt the person to attempt it.An open discussion of suicide with a person with depression does not prompt theperson to attempt it. In fact, extracting a promise that the person will not attemptsuicide before calling or visiting a mental health worker may well prevent a suicide.People who attempt suicide and fail aren’tserious about killing themselves.Most people who commit suicide have made previous unsuccessful attempts.If someone threatens suicide, it is best to ignoreit so as not to encourage repeated threats.Though some people do manipulate others by making idle threats, it is prudent to treatevery suicidal threat as genuine and to take appropriate action.
Overview: Mood Disorders CONCEPT CHART 13.4Lifetime Prevalence(approximate)Type of DisorderSymptomsAssociated FeaturesMajor depression12% in men, 21% in women,16.5% overallDowncast mood, feelingsof hopelessness andworthlessness, changes insleep patterns or appetite,loss of motivation, loss ofpleasure in pleasant activitiesFollowing a depressiveepisode, the person mayreturn to his or her usualstate of functioning, butrecurrences are commonBipolar disorder1%Periods of shifting moodsbetween mania anddepression, perhapswith intervening periods ofnormal moodManic episodes arecharacterized by pressuredspeech, flight of ideas, poorjudgement, hyperactivity, andinflated mood and sense ofself Sources: Prevalence data based on American Psychiatric Association, 2013; Conway et al., 2006
Psychological Disorders (5 of 6)Module 13.1 What Is Abnormal Behavior?Module 13.2 Anxiety-Related DisordersModule 13.3 Dissociative and Somatic Symptom and Related DisordersModule 13.4 Mood DisordersModule 13.5 Schizophrenia Describe the features of schizophrenia and underlying causal factors. Explain the development of schizophrenia based on the diathesis-stressmodel. Module 13.6 Personality Disorders Jeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
Module 13.5SchizophreniaJeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
Symptoms ofSchizophreniaJeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
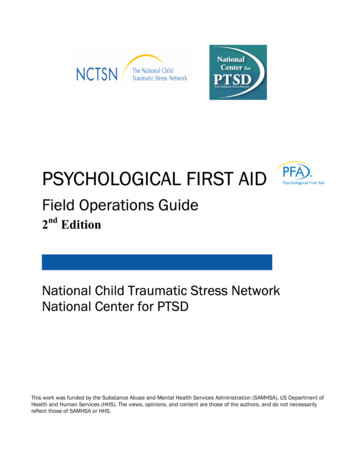
Causes ofSchizophreniaFIGURE 13.5Jeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
Overview: Schizophrenia CONCEPT CHART 13.5DescriptionA chronic psychoticdisorder affecting about1% of the populationSymptomsDelusions, hallucinations, bizarrebehavior, incoherent or looselyconnected speech, inappropriateemotions or lack of emotionalexpression, social withdrawal, andapathyProbable CausesAn interaction of a geneticpredisposition and life stress;underlying brain abnormalities
Psychological Disorders (6 of 6) Module 13.1 What Is Abnormal Behavior?Module 13.2 Anxiety-Related DisordersModule 13.3 Dissociative and Somatic Symptom and Related DisordersModule 13.4 Mood DisordersModule 13.5 SchizophreniaModule 13.6 Personality Disorders Define the concept of personality disorders. Describe the features of antisocial personality disorder and borderlinepersonality disorder and underlying causal factors in these disorders.Jeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
Module 13.6Personality DisordersJeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
AntisocialPersonalityDisorderJeffrey S. Nevid, Essentials of Psychology: Concepts and Applications, 5th Edition. 2019 Cengage. All Rights Reserved. Maynot be scanned, copied or duplicated, or posted to a publicly accessible website, in whole or in part.
Overview: Antisocial and Borderline Personality Disorder CONCEPT CHART 13.6DisorderLifetime Prevalence inPopulation (approximate)SymptomsAssociated FeaturesAntisocialpersonalitydisorderUpwards of 6% in men,1% in womenA pattern of antisocial and irresponsiblebehavior; callous treatment of others;lack of remorse for wrongdoingLacks empathy for others and may takeadvantage of people or fail to meet ��5.9%Unstable moods and stormyrelationships with others; unstableself-image; lack of impulse controlMay engage in self-destructivebehaviors, such as cutting themselves Sources: Prevalence data based on American Psychiatric Association, 2013; Cale & Lilienfeld, 2002; Kernberg & Michels,2009; Kessler et al., 1994; Paris, 2010
What Is Abnormal Behavior? Identify criteria used to distinguish normal behavior from abnormal behavior, and apply these criteria to the case examples of Claire and Phil. Identify the major contemporary models of abnormal behavior. Describe the features of psychological disorders and expla