Transcription
nng ioui atin ucnt EdCo icaledMObjectivesAfter reading this continuing educationarticle, the podiatric physician should beable to do the following:1) Be familiar with the clinical goals ofmedical nutritional therapy.2) Identify the eight principles of healing a diabetic foot wound.3) Be able to describe the basic principles of nutritional management of patients with diabetic foot wounds.NutritionalAspects of Healinga Diabetic FootWoundThis is an essential but often overlookedaspect of wound healing.4) Describe a comprehensive nutritionalassessment.5) Be able to relate the phases of woundhealing with basic nutritional needs.6) To discuss the role of calories andweight loss in diabetic foot wound healing.7) Understand the roles of proteins,fats, carbohydrates, vitamins, mineralsand trace elements in diabetic foot woundhealing.8) To delineate the appropriate bloodtests needed to assess nutritional status ina patient with a diabetic foot wound.Welcome to Podiatry Management’s CME Instructional program. Our journal has been approved as a sponsor of Continuing Medical Education by the Council on Podiatric Medical Education.You may enroll: 1) on a per issue basis (at 17.50 per topic) or 2) per year, for the special introductory rate of 109 (yousave 66). You may submit the answer sheet, along with the other information requested, via mail, fax, or phone. In the nearfuture, you may be able to submit via the Internet.If you correctly answer seventy (70%) of the questions correctly, you will receive a certificate attesting to your earned credits. You will also receive a record of any incorrectly answered questions. If you score less than 70%, you can retake the test atno additional cost. A list of states currently honoring CPME approved credits is listed on pg. 210. Other than those entities currently accepting CPME-approved credit, Podiatry Management cannot guarantee that these CME credits will be acceptable byany state licensing agency, hospital, managed care organization or other entity. PM will, however, use its best efforts to ensurethe widest acceptance of this program possible.This instructional CME program is designed to supplement, NOT replace, existing CME seminars. Thegoal of this program is to advance the knowledge of practicing podiatrists. We will endeavor to publish high quality manuscriptsby noted authors and researchers. If you have any questions or comments about this program, you can write or call us at: Podiatry Management, P.O. Box 490, East Islip, NY 11730, (631) 563-1604 or e-mail us at bblock@prodigy.net.Following this article, an answer sheet and full set of instructions are provided (p. 210).—EditorBy Kenneth B. Rehm, DPMIn a patient who has diabetes, healing a foot ulcer, just like healing aproblem in any other part of thebody, requires incorporating basicwww.podiatrym.comprinciples and a systematic approachthat must include medical nutritiontherapy. In general, the clinical goalsof medical nutrition therapy in a diabetic patient are to:1. Achieve and maintainglycemic control by balancing foodintake with insulin (exogenous or endogenous) or oral glucose-loweringmedications and activity levels.Continued on page 200NOVEMBER/DECEMBER 2003 PODIATRY MANAGEMENT199
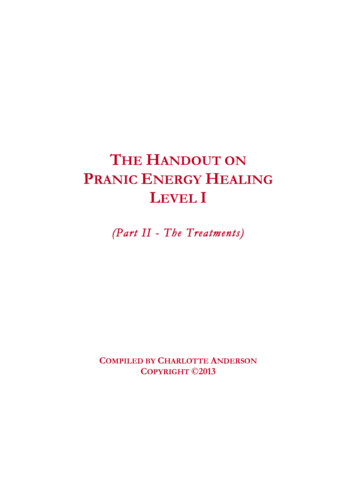
M Ced onica tinl E uidu ngcationNutrition.2. Achieve optimal bloodlipid levels3. Provide adequate calories tomaintain or attain reasonableweights for adults, normal growthand development rates in childrenand adolescents, metabolic needsduring pregnancy and lactation, orrecovery from illnesses that arecatabolic or to heal wounds.4. Eliminate, prevent, delay orcontrol nutrition-related risk factorsand complications such as hypoglycemia, short-term illnesses, exercise-related problems, renal disease,autonomic neuropathy, hypertension, cardiovascular and peripheralvascular disease, and skin breakdown.5. Achieve, maintain or improveoverall health through appropriatenutrition.Medical nutrition therapy is partof the systematic approach to healinga diabetic foot wound which incorporates the following basic principles:1. There must be adequate circulation to the wound site.2. A wound must be kept cleanand free from contamination.3. Necrotic tissue must be eliminated or reduced to a minimum.4. A wound must be free from infection.5. Dermatologic disease must becontrolled or eliminated.6. Shearing, friction and directpressure on a wound must be kept ata minimum.7. The external wound healingenvironment must be controlled andkept free from excess dryness andmoisture.8. The wound host must be nutritionally, metabolically and medicallyESSENTIALS OF ANUTRITIONAL HISTORYWeight ChangeAppetiteSatiety levelTaste changes and aversionsNausea and/or vomitingBowel habits including any diarrhea, constipation, or steatorrheaAlcohol or recreational drug useSmoking historyChewing and swallowing abilityPain while eatingChronic diseases that affect the use of nutrientsSurgical resection or disease of GI tractUsual meal pattern and dietary historyDietary restrictionsUse of vitamin, mineral and nutritional supplementsFood allergies and intolerancesMedicationsLevel of Activity or ExerciseAbility to secure and prepare foodstable.It is the nutritional aspects thatare to be discussed in this paper.The ability of a patient with a diabetic foot ulcer to heal is affected bythe baseline nutritional status andpre-existing nutritional deficiencies.A resultant suboptimal outcome andpoor healing prognosis is related toincreased susceptibility to the development of foot ulcers, increased timeneeded for wound healing, increasedlikelihood for reoccurrence, decreased tensile strength of a closedwound, increased susceptibility to infection and post-surgical complications in general. Providers of care fordiabetic foot wounds should closelyscrutinize the nutritional status ofthese patients, and consider poor nutritional status a major causal element, especially in cases where thewound is not healing and all of theother factors for appropriate woundhealing are in place. Basic principlesof nutritional management of patients with diabetic foot wounds arethe following: correction of inappropriate appetite, swallowing, as well aschewing and dentition abnormalities, control of serum glucose, hyperlipidemia, hypertension, metabolicstatus, appropriate supplementationof vitamins and trace minerals, andascertaining and maintaining properdietary requirements. Before thesebasic principles of nutritional management are implemented, propernutritional assessment and its components must be accomplished.A comprehensive nutritional assessment evaluates macro- and micronutrient intake, co-morbiditesthat could affect the actual ingestionof nutrients and/or the assimilationof nutrients, medications that affectwound healing and/or serum glucoselevels, and the overall medical, nutritional and metabolic status of the patient. An optimal assessment shouldinclude relevant clinical and biochemical data, including the following blood tests: complete bloodcount with a differential, glycosylated hemoglobin levels, hematocrit,hemoglobin, lipid levels, blood ureanitrogen levels, serum creatinine, albumin, prealbumin, sodium andpotassium levels, total protein andtransferrin levels. Urine tests includequantitative values for protein, urineglucose and urine acetone. BloodContinued on page 201200PODIATRY MANAGEMENT NOVEMBER/DECEMBER 2003www.podiatrym.com
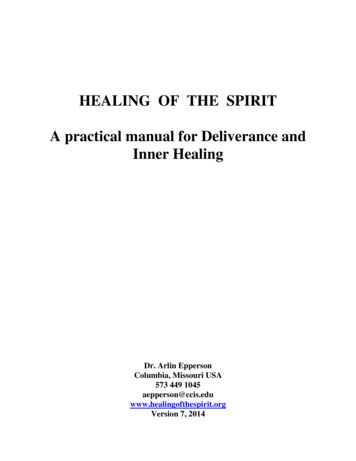
cells now begin to cover the surfaceof the wound until maturation occurs.In order for these four phases ofwound healing to progress, certainbasic nutritional requirements mustbe met:1. Proteins are required for tissuerepair2. Glucose is required for energy3. Lipids (fats) are required forcellular integritypressure readings are important.Determining the dietary prescription, restrictions, and level of compliance is essential information to beable to create proper nutritional status. It should be noted that poor nutritional status can be due to a poorappetite, a metabolic problem, or inability to digest or swallow appropriately. A close evaluation of food intake vs. caloric requirements should be performed, paying closeattention to proteins,fats, carbohydrates, keyvitamins, folic acid,Basal energy requirement is based upon the following:and key minerals, traceWomen: 655 (9.6 x W) (1.7 x H) - (4.7 x A)elements and micronutrients. Because of allMen: 66 (13.7 x W) (5 x H) – (6.8 x A)of these factors, it isW actual weight in Kg (2.2 lb 1 kg)imperative that a registered dietitian be inH height in cm (1 in. 2.54 cm.)volved in the assessment process.A age in yearsnng ioui atin ucnt EdCo icaledMNutrition.with pre-existing compromised nutritional status.Marasmus is a type of undernutrition associated with chroniccaloric deprivation. Depletion of somatic proteins and subcutaneous fatcauses a decrease in body weight. Significant marasmus is indicated by aweight that is less than 85% of a person’s ideal weight. Weight loss that isless than 10% of a person’s usualweight is considered mild, moderateif it ranges from 10% to20%, and severe if theweight loss is 20% orgreater. Mild to moderate weight loss may, infact, improve serumglucose levels even ifdesired weight is notreached. The problemis that without beingable to bear weight, asis the case in manywound patients, it isdifficult to achieveweight loss. In fact, it isoften necessary toavoid purposeful weight reductionuntil the foot wound is closed.BASAL ENERGY EXPENDITURE (BEE)Healing PhasesWith the nutritional assessmentmade, the correction or preventionof malnutrition is critical in optimizing wound healing. Nutritional status is the reserve from which the patient will draw upon to close the skindefect. With the other principles ofwound healing in place, if the patient is well nourished, and not challenged again, the wound is likely toclose. If the patient is malnourishedat the start of the healing process, thewound cannot be expected to closein a timely manner. The nutritionalsubstrate is essential for tissue formation because nutrients are importantto the appropriate completion of thefour phases of wound healing.These four phases are separateand overlapping. They are:1. The hemostatic phase. This isthe phase where platelet aggregationbegins the process of blood coagulation in the wound.2. The inflammatory phase. Thisphaseischaracterizedbymacrophage proliferation and theiringestion of bacteria and debris.3. The connective tissue phase. Thisis when fibrous tissue and collagenforms to create a lattice work thatsupports new blood vessels. Thewound now begins to contract andclose.4. The epithelial phase. Epithelialwww.podiatrym.com4. Vitamins, minerals and traceelements are required for optimalmetabolic function.The providers of care and thewounded individual must create ateam that provides the appropriatenutrients for healing through theproper intake of food and appropriate supplementation or tube feedingif needed.Calories and Weight LossIn a patient that has diabetes andfoot ulcers, the caloric requirementsare merely a function of metabolically active tissue, especially lean bodymass, and may vary significantlyamong patients. The requirementsare not different from those of astressed patient without diabetes. Accurately measuring energy expenditure, and therefore needs, is criticalin the patient who requires aggressive nutritional support by way oftotal parenteral nutrition or enteraltube feedings, a surgical procedure,or has a significant wound to heal.The most commonly used formulafor determining basal energy expenditure (BEE) is the Harris-Benedictequation.Weight as a percentage of idealbody weight or weight loss comparedwith the patient’s usual weight aremarkers used to identify patientsProtein RequirementsIn detailing the basic nutritionalrequirements, the first considerationis the protein and calorie requirements. The provision of sufficientcalories is a priority so that proteinwill be spared for its critical roles inthe stimulation of fibrin formation,cell multiplication, connective tissueformation, collagen formation anddeposition, increasing of enzyme activity, diminishing catabolism, enhancing immunity and improvingoverall wound healing. Protein deficiency suppresses the immune response, inhibits angiogenesis, decreases fibroblast formation and remodeling of collagen and impairsoverall wound healing.A review of the componentswe’ve identified in the four phases ofwound healing reveals that skin formation, white blood cell activity, immune function and collagen formation are all protein-based. The presence of all essential amino acids is required for protein synthesis. All aspects of wound healing are delayedunder conditions of protein deficiency. Therefore, adequate protein intake is absolutely essential for woundContinued on page 202NOVEMBER/DECEMBER 2003 PODIATRY MANAGEMENT201
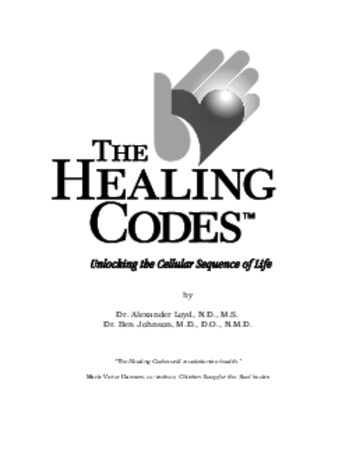
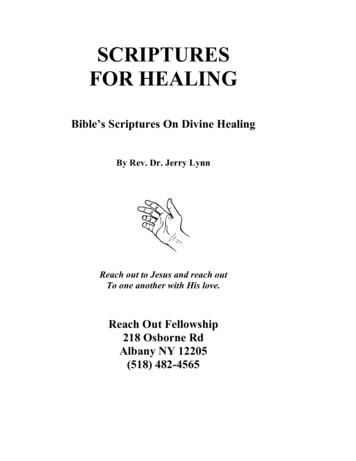
M Ced onica tinl E uidu ngcationNutrition.healing to occur. Adequate protein consumption is so vital thateven a mild depletion has a negativeimpact on the wound healing process.Protein-Calorie MalnutritionThere are basically three types ofprotein-calorie malnutrition: (1)Marasmus involves decreased caloriesand protein. It is usually associatedwith prolonged starvation, anorexia,chronic illness and the elderly. Ittakes months to years to develop. (2)Kwashiorkor involves decreased protein intake alone and is usually a result of fad diets, liquid diets, or longterm dextrose-containing IV fluidsupplementation with nothing bymouth. It takes weeks to months todevelop. (3) Combined is a result ofdecreased calories, protein intake andstress. It is usually associated with acatabolic stress situation without nutritional support. It is important todifferentiate the type of protein-calorie malnutrition because each has adifferent effect on wound healing.Clinical studies have shown thatany protein-calorie malnutritionleads to compromised wound healing and a greater risk for developingpressure-related ulcerations.Various diseases can lead to allforms of protein-calorie malnutrition. Common diseases linked withthis form of malnutrition include: cancer chronic illness protein loss in the gastrointestinal tract anorexia and other eating disorders multiple traumas liver disease obesity pancreatitis burns over 30% or more of yourbodyOvert signs of malnutrition mayexist and include severe wasting, extreme weight loss, weakened resistance to infection, being unable tothink clearly, or hair becoming brittleor falling out. In addition, the skinmay be dry or yellowish, musclesmay feel weak, and fainting spellsmay occur. In younger women, menstrual periods may stop.Protein-calorie malnutritionposes a severe danger to the patientbecause it can occur very rapidly andwithout overt signs of malnutrition.Therefore it is important to appropriately monitor the nutritional statusby examining serum levels of pre-albumin, albumin, total protein, andtransferrin levels and by performinga CBC with a differential, hematocritContinued on page 203PROTEIN-CALORIE MALNUTRITIONMarasmusKwashlorkorCombinedNutritional settingDecreased caloriesand protein intakeDecreased protein intakeDecreased calories,decreased protein intakeand increased stressClinical settingProlonged starvation,anorexia, chronicillness, elderlyFad diets, liquid diets, longterm dextrose-containingIV fluid supplementationwith nothing by mouthCatabolic stress withoutnutritional supportTime course todevelopMonths to yearsWeeks to monthsDays to weeksClinical featuresStarved appearanceMay look well-nourishedor obese. Edema, ascitesmay be present. Normalanthropometrics.Moderately to severelystarved appearanceDecreasedanthropometricsLaboratory findingsNormal visceralproteinsDecreased visceralproteins, Decreasedlymphocyte count,AnergicDecreased immunefunction valuesDecreased visceralproteinsClinical courseReasonably preservedand responsive toshort-term stressDiminished woundhealing, Diminishedimmunocompetence,Increased infections,Increased overallcomplicationsDiminished woundhealing, Increasedoverall complicationsand slower recoveryMortality rateLow unlesscomplications ofunderlying diseaseprocessHighHigh202PODIATRY MANAGEMENT NOVEMBER/DECEMBER 2003www.podiatrym.com
and a hemoglobin.The pre-albumin test measures aprotein that reflects nutritional status. Pre-albumin most often is usedto help diagnose protein-calorie malnutrition. In this condition, whichcan affect more than 30% of physiologically stressed or wounded patients, the body breaks down muscle,protein, and body fat. This type ofmalnutrition can lead to complications and even death if not treated.The test also is used to monitorchanges in patients who are receivingparenteral nutrition (nutrition fromoutside of the gastrointestinal tract,such as nutrients given through intravenous treatment). The test also isused to monitor changes in nutritionstatus for patients who are receivinghemodialysis.Depending on the exact levels, ifpre-albumin is low, minor nutritional deficiencies can be the only problem or if pre-albumin is very low,then protein-calorie malnutrition hasto be considered.Conditions that may lead tolower levels of pre-albumin are thefollowing: Severe or chronic illness, suchas cancer Hyperthyroidism Liver disease Serious infections Digestive disorders Inflammatory disordersWhen inflammation and malnutrition are both present, pre-albuminlevels fall very far, very quickly.Higher levels of pre-albumin arecommon in patients with: high-dose corticosteroid therapy hyperactive adrenal glands high-dose non-steroidal anti-inflammatory medications Hodgkin’s diseaseIf a patient is in renal failure, prealbumin results may be falsely higherthan they actually are.Inflammation can interferewith the results of your pre-albumin test, causing it to be lowerthan it would be. Certain drugs canalso lower your pre-albumin level,including amiodarone, estrogens,and oral contraceptives (birth control pills). Drugs that can causeyour pre-albumin level to rise inyour blood are anabolic steroids,www.podiatrym.comandrogens, and prednisolone.Recent research has shown thatthe pre-albumin test can predict pooroutcomes for hemodialysis patients.A low initial reading (baseline level)of pre-albumin predicts that a patientmay have problems, and steadilydropping pre-albumin values are associated with low survival.Pre-albumin is the best marker ofmalnutrition because it has a shortserum half-life, it is less affected byliver disease than other proteins andis not affected by hydrations status orvitamin deficiency (except zinc).Serum albumin levels measurevisceral protein levels and thereforethe body’s ability to manufactureprotein. It is an adequate indicatorof this ability for stable patientswith a chronic medical condition,such as diabetes. If the patient isbeing evaluated during an acute illness, the urinary creatinine heightindex should be used. Serum albumin levels are often used to test forliver or kidney problems, or tolearn if there is a lack of amino acidabsorption. Because turnover timefor albumin is 14 days, it is less sensitive than other measures. For instance, pre-albumin changes morequickly, making it more useful fordetecting changes in short-term nutritional status than albumin.AlbuminAlbumin is the major proteinsynthesized by the liver. It maintains plasma oncotic pressure andtransports nutrients in the bloodstream. Low albumin levels maylead to edema in the lower extremities, skin breakdown and openwounds and increased infection, aswell as increased morbidity andmortality. Decreased albumin levelscorrelate with poor clinical outcomes, increased length of hospitalstay, increased risk for complications and death. It should be notedthat hypoalbuminemia is an excellent marker for the stress response,but is considered to be a poor marker for overall nutritional status eventhough albumin levels are oftenused to monitor nutritional status.According to a recent study, thosepatients with diabetes and foot ulcers had significantly higher levelsof fibrinogen and C-reactive protein. (This is a test that measuresthe concentration of a special typenng ioui atin ucnt EdCo icaledMNutrition.of protein in serum, produced by the liver, which isonly present during episodesof acute inflammation. The mostimportant role of CRP is its interaction with the complement system,which is one of the body’s immunologic defense mechanisms.)Diabetics also had lower albuminlevels when compared to twogroups of control patients, thosewith diabetes and no foot ulcersand those with neither diabetes norfoot ulcers. The decreased albuminlevels results from a shift in thehepatic synthesis of proteins thatresult in an increase in acute-phaseproteins and decreased productionof homeostatic proteins. It is important to note that vascular permeability is increased because ofthis shift and proteins escape fromthe vascular space.A common mistake made by clinicians in treating patients with diabetes and foot ulcers is to interprethypoalbuminemia as a sign of malnutrition. When hypoalbuminemiashows up, calories are often increasedsignificantly, leading to hyperglycemia and weight gain, both ofwhich interfere with wound healing.Total protein measurements canreflect nutritional status. In addition,low total protein levels can suggest aliver disorder, a kidney disorder, or adisorder in which protein is not digested or absorbed properly. Morespecific tests, such as albumin andliver enzyme tests, must be performed to identify which proteinfraction is abnormal, so that a specific diagnosis can be made. High totalprotein levels can indicate dehydration or some types of cancer (e.g.,multiple myeloma) in which an abnormal protein is accumulated, andfurther tests must be performed.Total iron binding capacity(TIBC) is an indirect measurementof transferrin, a protein that bindsand transports iron. It quantifiestransferrin in terms of the amountof iron it can bind and is reportedas percent saturation. Transferrinlevels are generally depressed in patients who are malnourished orwho have chronic disease states;however, it may be normal in manypatients who are iron deficient.Patients who are malnourished orprotein-depleted benefit by earlyContinued on page 204NOVEMBER/DECEMBER 2003 PODIATRY MANAGEMENT203
M Ced onica tinl E uidu ngcationNutrition.feeding with a high protein formula. Some evidence exists thatprotein supplements (T) improve thehealing process in any physiologically or metabolically stressed individual. This has a positive impact on allphases of wound healing, especiallythe critical initial phases. It should benoted that every patient’s needs aredifferent. Protein requirements varyaccording to1. the size of the wound2. the nutritional and physiologicstate of the patient3. complications associated withprotein absorption and/or proteinmetabolismIt should be noted, however, thatmost wound healing patients, especially diabetics, require an increase inprotein in their diet in conjunctionwith adequate calories. Research suggests that increasing protein intaketo 20% or more of total calories mayresult in improved nitrogen balancein malnourished patients. Obtainingpositive nitrogen balance is important to counter the effects of nitrogen losses, common in diabetics andpatients under physiologic stress,and maximize the retention of nitrogen. At least 1 1/2-2 grams of proteinand 25-30 calories per Kg. of bodyweight is recommended. For severelystressed or injured patients, as inburn patients, up to 2 1/2 grams ofContinued on page 205NUTRITIONAL ASSESSMENTNORMAL REFERENCE LABORATORY VALUESDetermination Blood,Plasma, or Serum ValuesReference RangeCommentCholesterol120-220 mg/100 mL(serum)FastingTriglyceride40-150 mg/100 mL (serum)FastingCreatinine0.6-1.5 mg/100 mL (serum)FastingGlucose70-100 mg/100 mL(plasma)FastingGlucose (1 hr postprandial)180 mg/dL (plasma)Values above this number areconsidered diagnosticfor diabetes and requireconfirmation by otherdeterminations.Hemoglobin A1c3.8-6.4% (plasma)Potassium3.5-5.0 mEq/L (serum)HematocritMale: 45-52%Female: 37-48%HemoglobinMale: 14-18 g/dlFemale:12-16 g/dlFerritin-iron deficiency0-12 ng/mL13-20 borderline (serum)Prealbumin16 to 35 mg/dl (serum)Albumin3.5-5.0 g/100 mL (serum)Blood Urea Nitrogen8-25 mg/100 mL (serum)Sensitive measure ofnutritional statusUrine TestsAcetone plus acetoacetateQuantitative0Protein Quantitative 150 mg/24 hMay require more informationin diabetesGlucose Quantitative024 hour or other timed specimen204PODIATRY MANAGEMENT NOVEMBER/DECEMBER 2003www.podiatrym.com
protein and 35 calories per Kg. ofbody weight may be needed. If thepatient has nephropathy, a range of1.0 to 1.5 gm of protein per Kg. ofbody weight is recommended. If thiscannot be accomplished with increasing the amount of food a person eats, enteral formulas can be analternative.A standard enteral formula has 40grams of protein per 1000 calories.The high-protein formulation, whichis better equipped to meet the requirements of wound healing patients, has 60 grams of protein per1000 calories. Studies suggest that forthose patients who need a dietary alternative, high protein formulationshave been recommended. This is because they have lower calorie-to-nitrogen ratios and therefore are associated with increased nitrogen retention and balance, improved serumprotein levels and improved immunological function. Clinically, thisleads to reduction in the size of largewounds and improved healing ofsmaller wounds. It is important tonote that exceeding protein requirements will not cause the wound toheal faster.An elevated BUN in elderly patients on a high-protein diet shouldnot be of concern given that the patient does not have a pre-existingrenal condition, has normal creatinine levels and the state of hydrationon physical exam is normal. Urea isnot a toxic molecule and the buildupof urea in this patient is of no consequence; and in a patient with awound, the priority is healing thewound and not a normal BUN. Therisk of underfeeding and sub-optimalprotein consumption is non-healingand non-function. In patients whoare adequately fed or fed slightlyabove what’s needed, elevated serumurea is a result of an extra amino acidbeing changed to glucose.Hematocrit and hemoglobin values can be used as a gross indicatorof iron status in individuals with diabetes. Low values are generally associated with chronic blood loss,heavy menstrual bleeding, or gastrointestinal bleeding. Diets low insaturated fat and cholesterol that areroutinely prescribed for personswith diabetes often contain inadequate supplies of foods high inwww.podiatrym.comheme iron. The need for an ironsupplement should be assessed.A CBC with a differential willgive an indication as to if there is ahigh white cell count, common inmalnutrition and in infections. Protein intake should be monitored inclients at risk for renal disease. Modification of protein intake should become a decision reached by the physician, dietitian and the patient.There is suggestive evidence thatseveral amino acids, particularly arginine and glutamine, appear to promote wound repair. Arginine’s effectis linked to enhanced wound collagen synthesis and pituitary hormonesecretion; glutamine improves gutmucosal repair and serves as fuel forthe immunocytes. No improvementin wound healing has been demonstrated using high-dose supplementsof branched chain amino acid infusions.Carbohydrate RequirementsThe role of carbohydrates, as isthe case with fats, is less well-definedthan protein’s role. It is known, however, that the role of carbohydratesand fats is to provide the energyneeded for cell proliferation that occurs in all phases of wound healing.Leucocytes, which are white bloodcells that perform phagocytosis, utilize glucose as their primary fuel. Fibroblast proliferation, the key to collagen formation, also depends onglucose as their primary source of energy. It is clear that an abnormalityin glucose metabolism would be expected to have an effect on thesefunctions and therefore wound healing.Fat RequirementsFat in the diet is an absolute necessity for wound healing in a diabetic. However, because granulation tissue is an obligate glucose consumer,it follows that adherence to a highcarbohydrate diet can be of benefit.Some evidence exists in animal models that low-fat diets may be morebeneficial to wound healing than anover-all higher fat intake. Reductionin total fat intake, especially saturated fats, is therefore recommended.Less than 30% of the calories consumed should be from fat and lessthan 10% should be from saturatedfats. Fats, however, do help providethe fuel for all the phases of woundnng ioui atin ucnt EdCo icaledMNutrition.care as well as providefatty acids. The precise roleof fatty acids in wound healingis unknown. However, they are akey ingredient of triglycerides andphospholipids that are major components of cell membranes. Also, unsaturated fatty acids are precursors toprostaglandins and other regulatorsof the immune and inflammatoryprocesses. Therefore, it is reasonableto assume that a deficiency in fattyacids likely results in sub-optimalwound healing.A blend of fats has been shown tobe more beneficial in wound healingthan fats that come from a singlesource; and because various fats havedifferent benefits than others, a fatblend can play an advantageous rolein the healing of wounds where ahigh metabolic or physiologic stresssituation exists or in wound healing.For this reason, a lipid profile including essential fatty acids, especially omega 3 fatty acids, is critical.Why “essential?” Omega-3’s (andomega-6’s) are termed essential fattyacids (EFA’s) because they are criticalfor good health; and a deficiency inthem has been shown to inhibit tissue regeneration. However, the bodycannot make them on its own. Forthis reason, they must be obtainedfrom food, thus making outsidesources of these fats essential.Although the body needs bothomega-3’s and omega-6’s to thrive,most people consume far more 6’sthan 3’s. Hardly a day goes
Healing Phases With the nutritional assessment made, the correction or prevention of malnutrition is critical in optimiz-ing wound healing. Nutritional sta-tus is the reserve from which the pa-tient will draw up