Transcription
Nutrition andWound HealingContent Creators:Members of the South West Regional Wound Care Program’s Clinical Practiceand Knowledge Translation Learning CollaborativeL
Learning Objectives2. Describe the role of nutrients in wound healing3. Identify nutritional requirements based on theetiology of the wound4. Describe available nutritional supports for thoseunable to meet their nutritional needs orallySouth West Regional WoundCare Program1. Describe the various aspects of nutritionalscreening and assessment2
South West Regional WoundCare ProgramNUTRITIONAL SCREENING ANDASSESSMENT3
Nutritional Screening1 Purpose - to pinpoint individuals who are malnourished or atnutritional risk: Malnutrition is associated with increased length of stay, costs,and morbidity/mortality Nutritional supports can help: Increase physical strength; Speed recovery and wound closure, and; Decrease the risk of infection.South West Regional WoundCare Program “The process of identifying characteristics known to beassociated with nutritional problems”4
Persons at Risk1 Inadequate absorption: Irritable Bowel Syndrome, Crohn’s, Colitis Diarrhea or vomiting Increased losses: Colostomy, ileostomy Fistula Wounds Increased requirements: Congestive Heart Failure, Chronic Obstructive Pulmonary Disease,pneumonia, asthma Wound healingSouth West Regional WoundCare Program Inadequate intake: Cerebral vascular accident (CVA) Elderly Reduced access to food Poor dentition or mouth sores Dysphagia Esophagitis5
Functional limitations Difficulty chewing, swallowing Inability to physically prepare meals or travel to dining room Poor hearing, vision Altered mental status Difficulty self feeding Inability to understand importance of eating Advanced dementia weight loss, dysphagia, malnutrition Drug therapy: Nausea/vomiting side effects Corticosteroids inhibit protein synthesis and cause depletion of vitamin A fromliver Impaired localized blood flow Poor appetite/intake Decreased thirst response Decreased ability to concentrate urine Intentional fluid restriction Advanced ageSouth West Regional WoundCare ProgramAdditional Risk Factors16
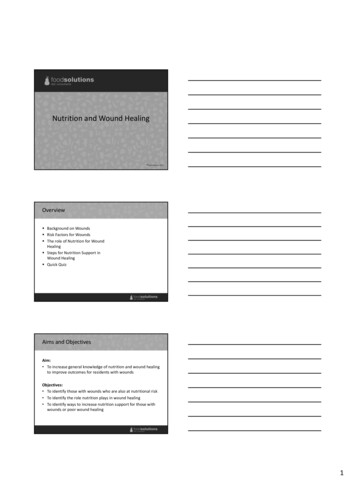
NESTLE NUTRITION INSTITUTE MININUTRITIONAL ASSESSMENT (MNA ) Allows for earlier intervention to provide adequate nutritionalsupport Six questions The screening score (max 14 points): 12‐ 14 points normal nutritional status 8‐11 points at risk of malnutrition 0 ‐7 points malnourishedSouth West Regional WoundCare Program MNA is a screening and assessment tool that identifies individualsage 65 and above who are malnourished or at risk of malnutrition7
South West Regional WoundCare ProgramMNA Form8
Nutritional Assessment1 The “interpretation of data from the (nutritional) screeningprocess” Purpose is to allow for the development of a nutritional careplanSouth West Regional WoundCare Program Includes a review of data from all disciplines9
Physical Conditions1-2 Skin condition: Signs of dehydration Edema Ascites Signs of weight loss Loose skin Non-healing wounds Purpura/bruisesSouth West Regional WoundCare Program Dry, flaky skin Skin that tents10
BMI1 Body mass index (BMI) Indicator of obesity (highly correlated with body fat) A BMI of 21 with unintentional weight loss puts a person atrisk for pressure ulcer developmentSouth West Regional WoundCare Program Weight to height ratio11
Height and Weight1 Regular and frequent weight monitoring is themost non-invasive, time-efficient, inexpensive andmost reliable indicator of nutritional adequacySouth West Regional WoundCare Program Weight and body composition change with age: Weight peaks in 60’s and decreases beyond 70’s Proportion of body fat increases with age12
Significant UnintentionalWeight Loss 5% loss of usual weight over one month 7.5% loss of usual weight over three months 10% loss of usual weight over six monthsSouth West Regional WoundCare Program Significant nutrition/health risk 13
South West Regional WoundCare ProgramROLE OF NUTRIENTS IN WOUNDHEALING14
CarbohydratesProteinFatsVitaminsWaterMineralsSouth West Regional WoundCare ProgramKey Nutrients in Wound Healing15
Nutrition is ParamountA wound healed without optimal nutrition will be weak and ismore likely to break down againSouth West Regional WoundCare ProgramNutrients involved in wound healing function in cellular,structural, and immune processes and in all phases of woundhealing16
Carbohydrates1 Most readily available source of energy Regulate metabolism Provide flavor, color, variety to the diet Provide 4 kcal/g energySouth West Regional WoundCare Program Spare protein for building and maintaining tissues17
Food Sources of Carbs1GrainsCerealsLegumes (peas and beans)PastaBreadNatural sugars in fruits, veggies, and milkAdded sugarsSouth West Regional WoundCare Program 18Sources of CarbohydratesImages Source: National Cancer Institute (Renee Comet - Photographer
Synthesis of enzymes and hormones involved in wound healing Cell multiplication Synthesis of collagen, epidermal cell proliferation, skin integrity, andresistance to infection and immune response Supplies structural and binding material of muscle, cartilage,ligaments, skin, hair, and fingernails A component of antibodies and immune system function Helps to maintain the fluid and mineral composition of various bodyfluids Helps transport needed substances, such as lipids, mineral andoxygen, around the body Serves as building material for growth and repair of body tissues 4 kcal/gSouth West Regional WoundCare ProgramProtein119
Meat, fish, poultryEggsDairy products (milk, cheese, yogurt)LegumesSeedsGrains*Protein from animal sources are better as they have the amino acidsessential to human nutrition in adequate amountsSouth West Regional WoundCare ProgramFood Sources of Protein120Sources of ProteinImages Source: National Cancer Institute (Renee Comet – Photographer)
Maintains normal cell membrane function Permit fat-soluble substances to move in and out of thecell Provide insulation under the skin Cushion the kidneys and other organs from injury Provide flavor and aroma in foot Carry fat soluble vitamins Serve as the most concentrated source of heat andenergy: 9 kcal/g Provide energy during periods of food deprivationSouth West Regional WoundCare ProgramFats121
Meat Dairy products Fish and vegetable oils Nuts Some fruits, i.e. avocados and olivesSouth West Regional WoundCare ProgramFood Sources of Fat122Sources of FatImages Source: National Cancer Institute (Renee Comet – Photographer)
Facilitate various chemical reactions in the body Key role in normal cell functioning and cell’s ability to useenergy Participate in protein synthesis and cell replication Various therapeutic properties:VitaminPropertiesVitamin ARequired for inflammatory processVitamin BRequired for cross-linking of collagen fibersVitamin CCan increase activation of leukocytes and macrophagesSouth West Regional WoundCare ProgramVitamins123
A, D, E, KDerived from fatty and oily parts of certain foodsStored in fatty tissue and liver until neededLack of vitamin A can retard epithelialization and decreasecollagen synthesisSouth West Regional WoundCare ProgramFat Soluble Vitamins124
B, C, D, EDerived from the water components of foodsDistributed throughout water compartments of the bodyNot stored – excreted with concentration becomes too highVitamin B needed to produce energy from glucose, aminoacids, and fat Vitamin B6 helps maintain cellular integrity and helps formblood cells Thiamine and riboflavin needed for cross-linking andcollagenationSouth West Regional WoundCare ProgramWater Soluble Vitamins125
Vitamin C1 Required for production of strong collagen Facilitates leukocyte migration to the wound, increasing Needed for neutrophil superoxide formation and bacterialkilling Increases the activation of macrophages at the wound siteSouth West Regional WoundCare Programresistance to infection26
Aids in hydration of wound site and oxygen perfusion Acts as a solvent for minerals, vitamins, amino acids, glucose,and other small molecules, and enables them to diffuse in andout of cells Transports vital materials to cells and carries waste away fromcells Serves as a lubricant Maintains body temperatureSouth West Regional WoundCare ProgramWater127
Dehydration in the OlderAdult4 Total body water decreasesKidneys can’t concentrate urine as wellDecreased thirst sensationChanges in hormone levels that affect the kidneyEffects of medications, i.e. diureticsChanges in mobility, cognition and independenceSelf-imposed fluid restrictions – fear of incontinenceSouth West Regional WoundCare Program One of the most common reasons for hospitalization As people age:28
Hydration status intake – outputRecommended fluid intake for average person 27-30mL/KgMinimal fluid intake for older adults 1500mL/dayYounger people need 35mL/Kg/dayConsider all routes of fluid losses: Gastrointestinal tractUrinary tractFever/sweatingWound exudateNegative pressure wound therapyAir-fluidized bedsRespiratory tractSouth West Regional WoundCare ProgramMonitoring Fluid Status429
Decreased urine outputDark, concentrated and/or strong smelling urineFrequent urinary tract infectionsDry lips/mouth and thick, stringy salivaConstipationOrthostatic hypotensionConfusion or change in mental statusWeight loss of 3.5Lbs in less than a weekFeverDecreased skin elasticitySunken eyeballsSouth West Regional WoundCare ProgramSigns of Deficiency1, 430
Tips to Increase Fluids1, 4Jell-O½ cup120mLPudding½ cup100mLIce Cream/Sherbet½ cup60mLPopsicle190mLYogurt½ cup90mLCanned fruit½ cup100mLSoup1 ½ cups165mLSouth West Regional WoundCare ProgramApproximate Fluid Provision from Common Foods Ice chips, ice cubes31
Build body structures Maintain fluid balance Activate enzyme systems Skeletal system depends on calcium, magnesiumand phosphorus for its structural integritySouth West Regional WoundCare ProgramMinerals132
Microelements1 Zinc Iodine Iron Copper Manganese MagnesiumSouth West Regional WoundCare Program Needed in small amounts:33
Needed for protein synthesis, collagen synthesisRe-epithelializationDNA synthesis, cell division, and proliferationDisposal of damaging compounds produced byleukocytes during wound debridement Trace mineral and component of 200 enzymesSouth West Regional WoundCare ProgramFunctions of Zinc in Wound Healing134
Meat, poultry, fish/seafood (especially oysters)LiverEggsMilkLegumesWhole wheat productsWheat germSouth West Regional WoundCare ProgramFood Sources of Zinc135Sources of ZincImages Source: National Cancer Institute (Renee Comet – Photographer)
South West Regional WoundCare ProgramNUTRITION BASED ON WOUNDETIOLOGY36
Burns1 Hypermetabolism accompanied by exaggerated proteincatabolism for energy and increased urinary nitrogenexcretion forcing use of protein for energy Protein loss through wound exudateSouth West Regional WoundCare Program Energy requirements can increase 100% depending onextent/depth of burn37
Skin Tears1 Protein Calories FluidsSouth West Regional WoundCare Program If limited improvement of wound after seven days, consideraddition of:38
Diagnose the causeImprove tissue perfusion if possibleProvide compressionManage concurrent diseasesSupport alterations in lifestyle: Weight loss Proper diet Smoking cessationSouth West Regional WoundCare ProgramLeg Ulcers139
Dermatitis1 PregnancyOral contraceptivesAntibiotic therapyDiabetesSkin macerationSteroid therapyEndocrinopathiesSouth West Regional WoundCare Program Candida albicans Normally found in mouth, vaginal tract, gut Candidiasis results from:40
Pressure Ulcers Depending on severity of the ulcer: Zinc should be reassessed at 10 days and discontinued if normal Protein: 1-2g/Kg Calories: 25-40Kcal/Kg Fluids: 20-45cc/KgSouth West Regional WoundCare Program Multivitamin supplementation if intake inadequate Vitamin C 500mg PO BID Elemental zinc 25mg PO BID41
Diabetic Foot Ulcers6 Hyperglycemia may be induced by: People with diabetes are at greater risk of infection due totheir host resistance: When blood glucose is high, chemotaxis and phagocytosis arecompromised This prolongs the inflammatory phase and impedes resolution ofinfection “The achievement of optimal glucose control is the mostimportant factor affecting wound healing in patients withdiabetes”South West Regional WoundCare Program Wound occurrence Presence of infection42
South West Regional WoundCare ProgramNUTRITIONAL SUPPORTS43
The provision of a liquid nutritional supplement in lieu ofwater with each medication pass Take medications with 60mL a 2-calorie per mL formula 1 can/day 500 calories, 20 grams protein, vitaminsand minerals Can use pudding supplements, thickened liquidsupplements Obtain physician order; enter on medication record Limits taste fatigue, decreases product wastage; smallportions multiple times/day; improves tolerance,improves nutritional status Specialized formula for wound healing availableSouth West Regional WoundCare ProgramThe Med Pass Program344
Other Practical Considerations3 Liberalization of diet restrictions if intake poor7 Address impairments in swallowing Supplement dysphagia dietsSouth West Regional WoundCare Program Address impairments in dentition Conduct supplement/snack audits45
Practical Considerations3 Address physical and cognitive impairments Encourage friends and family to bring in appropriatefavorite/familiar/cultural foods and beveragesSouth West Regional WoundCare Program Incorporate foods/fluids into therapy and/or recreationsessions46
Switch to Homo milk from skim Add dry milk powder to milk, cereal, pudding, casseroles,cream soups, etc. Switch to a higher calorie content nutritional supplement Add nutrient dense supplements to hot cereals, cream soupsand mashed potatoesSouth West Regional WoundCare ProgramConsider Other Ideas347
Review2. Role of nutrients in wound healing3. Nutritional requirements based on the etiologyof the wound4. Nutritional supports for those unable to meettheir nutritional needs orallySouth West Regional WoundCare Program1. Various aspects of nutritional screening andassessment48
SWRWCP Nutrition Resources Nestle Mini Nutritional Assessment (MNA ) Tool Procedure: Mini Nutritional Assessment (MNA ) Tool Patient Pamphlet: The Importance of Nutrition in WoundHealingSouth West Regional WoundCare Program A Guide to Completing the MNA Short Form49
1.2.3.4.5.6.7.Posthauer ME. Nutritional assessment and treatment. In: Sussman C, BatesJensen B. Wound Care: A collaborative practice manual for health professionals.3rd Ed. Baltimore, MA: Lippincott Williams & Wilkins, 2007:52-71.Niedert K, Dorner B. Nutrition care of the older adult. Chicago: American DieteticsAssociation, 2004:125.Fraser C. Enhancement of nutrition and hydration in patients. Wound Care Canada.2008;6(1):54-55, 81.Fraser C. The importance of monitoring hydration status in our clients. WoundCare Canada. 2009;7(1):18-20.Fraser C. The identification of barriers to pressure ulcer healing. Usingnutrition/hydration-related blood work. Wound Care Canada. 2010;8(2):20-25.Fraser C. Nutrition and wound care: The importance of investigating hyperglycemiain individuals with wounds. Wound Care Canada. 2007;5(2):20-21.Dorner B, Niedert C, and Welch P. Liberalized diets for older adults in long-termcare. J Am Diet Assoc 2002;102:1316-1323.South West Regional WoundCare ProgramReferences50
1. Describe the various aspects of nutritional screening and assessment 2. Describe the role of nutrients in wound healing 3. Identify nutritional requirements based on the etiology of the wound 4. Describe available nutritional supports for those unable t





![WOUND HEALING lecture.ppt [Read-Only]](/img/18/wound-healing.jpg)

