Transcription
MicroscopicDentistryA PracticalGuide
MicroscopicDentistryA PracticalGuidePublisherEditorsCarl ZeissDr. Tony DruttmanDr. Greg FinnAuthorsDr. José Aranguren CangasCoordinationDr. Kristina BadalyanSlaven SesticDr. Rino BurkhardtDr. Annett BurzlaffDr. Maciej GoczewskiDr. Manor HaasOscar Freiherr von StettenDr. Bijan VahediDr. Maxim StosekDr. Claudia Cia WorschechDr. Tony Druttman
ForewordDear Reader,Enhancing the visualization of medicalThe authors have succeeded in providing a mostprofessionals is a core focal point for us at thevaluable guide to using the surgical microscope in aMedical Technology Business of ZEISS. We striverange of dental applications. The articles were writtento help our users across a broad range of medicalwith the idea in mind that they shall enable a step-by-disciplines see more. Seeing more can helpstep implementation that unlocks the full potential ofclinicians to generate better outcomes, master evensurgical microscopy in your daily practice:highly complex cases, to gain greater enjoymentand satisfaction from their work and finally - butHow can the surgical microscope support anmost importantly - improve patients’ lives.ergonomically correct, upright working position whichis health promoting for the dentist over the long term?Since its inception in 1921, surgical microscopy hasbeen crucial for the advancement of several surgicalHow can the surgical microscope broaden your clinicalfields, such as brain tumour surgery, vascularscope and increase your efficiency - as key to theneurosurgery, cataract or retinal surgery.realization of a return on your investments?As Pioneer in Surgical Microscopes, we haveconstantly pushed the boundaries of visualization.How can the use of the surgical microscope add crucialToday, a large number of the mentioned surgicalbenefit to specific procedural steps in every majorprocedures would not be conceivable without thedental application?use of a surgical microscope.How can documentation with the surgical microscopeIn dental visualization we are at an earlier stage ofincrease patients’ involvement in the treatment andthis journey. Even though the surgical microscopedemonstrate your skills?has become the standard of care in endodontics,today only a single-digit percentage of all dentistsI am confident that implementing some of the preciousworldwide enjoy the benefits of working withinsights of this book in your daily practice will changethis tool. We firmly believe that this will changeyour professional life for the better.as the surgical microscope will pave the way toaccelerated medical progress in many applicationsin dentistry by giving the clinician a greater degreeSincerely,of control in a range of delicate procedural steps.In endodontics, the surgical microscope is alreadyan integral part of the postgraduate curriculum.For other dental applications, we are not thereyet. Therefore many dentists are seeking guidanceon how to integrate microscopy into their dailyDr. Christian Schwedespractice, beyond endodontics. To help fill this gap,Director Business Sector Dental & Office,we asked leading clinical specialists in differentCarl Zeiss Meditec AGdisciplines of micro-dentistry to contribute to thispublication.
Table of contents1The OPMI2Ergonomics25 Why use a surgicalmicroscope?26 Benefits27 How the OPMI differs frommedical loupes and theintra-oral camera55 Definitionsof ergonomics28 The human eye – how itworks and why it is limitedAccommodation29 Stereoscopy303132343536373840The components ofan OPMIObjective lensVarioscopeMagnification changerZoom systemBinocular tubeEyepiecesSet-up OPMI – Quick GuideCo-observation41 OpticsCorrection for chromaticaberration42 High transmission of lightDepth of field44 Field of view45 How to calculateend magnification46 Ergonomics and workflowVarioscope47 Looking around the corner –MORA interface and angledoptics48 LightLight sources49 Filters and pinhole diaphragm56 Overloads5860616264Minimizing overloadsPosition of dentistOperator range of 9-12 o’clockworking positionsPosition of the patientOPMI position66 Functional design67 OPMI assistance3OPMI in Endodontics73 Introduction74 Magnification in endodonticsWorking magnification75 Uses of the OPMI in endodontics76 Microendodontic instruments77 UltrasonicsUltrasonics tipsUses of ultrasonics in endodontics78 MirrorsMicro instruments Files with a handleStropko syringe79 BursDyes8082838485868891929395Examination of the externalsurface of the toothIdentification of the floorof the pulp chamberRemoval of coronal restorationsPreservation of tooth structureAssessement of canal cleanlinessafter preparationIdentification of internal cracksCanal locationCalcified canalsEvaluation and managementof perforationsObturation of the canalNon-surgical retreatmentUses of the OPMIin non-surgical retreatment:Apical plug with MTAFile evaluation94 Endodontic root-end surgery4OPMI in Periodontologyand Implantology5OPMI in Restorativeand Prosthodontics6Documentation7Practice Management105 Do we need an OPMIin periodontal and implanttherapy?135 Why use the surgicalmicroscope in restorative andprosthodontic dentistry?181 Why?191106 What are the advantagesand disadvantages ofthe use of an OPMIin periodontology andimplantology?136 Prevention and diagnosis110 What does the“microsurgical concept”consist of?142 Fractured line – “cracks”122 Which are the first steps togetting used to working withthe OPMI?150 Matrix adaptation126 How can you acquireexpertise in periodontaland peri-implantmicrosurgery?182 How?Photo/video186 Practical advice137 Bacterial plaque138 Caries148 Preparation controlThe benefits of the OPMIextend far beyondthe obvious and well-provenclinical benefits.192 Integration intoclinical practice193 The OPMIas a communication toolDento-legal aspects194 Marketingthe OPMI195 Health benefits to the dentist153 Rubber dam applications inanterior and posterior areas196 Financials of the OPMI154 Cervical lesions156 Finishing and polishing128 Which are the commonerrors in the use of theOPMI in surgical practice?160 Possibilities for analyzingthe surgical field at differentmagnifications130 References164 Replacements – avoiding wear166 The Tunnel preparation technique168 Indirect restorations172 Instruments174Excellence in operativeand prosthetic dentistry withregard to communicationwith patients176 References50 Free floating system –balanced system andmagnetic brakes51 Maintenance6OPMI and Varioskop are registeredtrademarks of Carl Zeiss7
The moment you see a hidden detailreveal a visible success.This is the moment we work for.// DENTAL OPTICSMADE BY ZEISS
Key benefit 1 // Magnification with OPMI*You can only treat what you can see *OPMI – Operation Microscope
Key benefit 1 // Magnification with OPMIINSTRUMENT REMOVALRETREATMENTCALCIFIED CANALSCRACKS AND FRACTURESSOFT TISSUE MANAGEMENTTUNNEL PREPARATIONTOOTH PRESERVATIONCARIES8.5X or you see more and treat more13.6X
Key benefit 2 // Ergonomics8 hours of spine strain 1415
Key benefit 2 // Ergonomics or 8 hours of working in comfort1617
Key benefit 3 // Visualization and DocumentationA picture is worth a thousand words 1819
Key benefit 3 // Visualization and documentation for better communication2021
11The OPMIAuthor: Dr. Annett Burzlaff25 Why use a surgicalmicroscope?26 Benefits27 How the OPMI differs frommedical loupes and intra-oralcamera28 The human eye – how itworks and why it is limitedAccommodation29 Stereoscopy303132343536373840The components ofan OPMIObjective lensVarioscopeMagnification changerZoom systemBinocular tubeEyepiecesSet-up OPMI – Quick GuideCo-observation41 OpticsCorrection for chromaticaberration42 High transmission of lightDepth of field44 Field of view45 How to calculateend magnification46 Ergonomics and workflowVarioscope47 Looking around the corner –MORA interface and angledoptics48 LightLight sources49 Filters and pinhole diaphragm50 Free floating system –balanced system andmagnetic brakes51 Maintenance23
1 The OPMIWhy use an OPMI?Can you still remember the first time you looked through aBeginning in 1990, many innovative dentists from numerousmicroscope or magnifying glass? Perhaps the first thing youcountries pressed for the use of OPMIs in dentistry: thissaw was a daisy which you thought you knew well, but whichdrive towards microdentistry was led by Dr. Syngcuk Kimthen under the OPMI opened up a new world for you. We(Philadelphia, Pennsylvania) and Dr. Clifford Ruddle (Santaare not only drawn into the microcosm by our curiosity, butBarbara, California) in the USA, as well as Dr. Peter Velvartwe also benefit from the insight we can gain into intricate(Zurich, Switzerland) in Europe, among others. Whiledetails and structures. Microscopy is an integral part of manyendodontics is the main discipline in which OPMIs aresurgical disciplines nowadays. Doctors first used the surgicalused in dentistry, other disciplines such as periodontology,microscope for microsurgical operations in the ENT area inimplantology or restorative dentistry are adopting the use1921. Ophthalmologists then attached lighting technology toof magnification technology. The dentist benefits fromthe surgical microscope and used it to perform eye operations.several advantages of OPMIs, regardless of the discipline.In the mid-1960s, neurosurgeons recognized the advantagesMagnification enhances the visual acuity and supports moreof using OPMIs for operations. Neurosurgery is today noprecise treatment. However, no light means no information.longer imaginable without documentation and navigationOPMIs are therefore designed in such a way that they combinesystems. The OPMI had been undergoing development forthe magnifying lens and the light source. No matter whetheraround 60 years before finding its way into the world ofthey are working with low or high magnification, the dentistsdentistry.benefit from shadow-free, direct light. It is natural for us toorientate ourselves visually in our surroundings. That is howwe judge distances and perceive size and space. We are ableto do this thanks to stereoscopic vision. An OPMI provides theconditions required for stereoscopic vision and therefore fordepth orientation. This, in turn, enables the safe, precise useof instruments and improves ergonomics. Relaxed eye musclesand being able to sit upright during treatment prevent fatigueand posture impairments.2425
1 The OPMI3.5 X5.1 X8.5 X21.25 X13.6 XHow the OPMI differs from medicalBenefitsloupes and the intra-oral cameraWhen working with instruments on aA correctly configured OPMI can preventpatient, a certain distance is requiredsymptoms of fatigue. On the followingIn dentistry, the first introductionenables the dentist to switch betweenIntra-oral cameras also providebetween the object, i.e. the tooth inpages you will find detailed informationinto the world of magnification isoverview to detailed view in a mattermagnified images, but they are onlythe oral cavity, and the front lens ofabout the components of an OPMI,generally a medical loupe.of seconds. The working distance of atwo-dimensional and do not providethe OPMI. This is what is referred towhat makes a good image and how toA medical loupe fulfills some of themedical loupe is fixed. Since a medicalany depth information. When lookingas the working distance. In dentistry,best configure the microscope.aforementioned requirements andloupe is worn on the dentist’s head, itthrough the OPMI, the dentist hasthe working distance with an OPMI isbenefits, but compared to an OPMIfollows every movement of the wearer.three-dimensional vision which isusually between 200 and 300 mm tois somewhat limited in its options.For the duration of the movement, theimportant for orientation and perceptionensure that enough space is providedMedical loupes are available with afield of view is blurred to a greater orof spatial dimensions. This is necessary,to handle the instruments over thefixed magnification between 2 - 5lesser extent. The dentist has to find thefor example, to correctly position thepatient. The correct working distancetimes. If the dentist wishes to have acorrect working distance to enjoy a fullydental instruments. In addition, whendepends on the height of the dentist.different magnification, this requiresfocused image again. The OPMI on theusing the intra-oral camera the dentistThe taller the dentist, the longer theusing a different pair of loupes. Theother hand, is mounted on a stand, ishas to interrupt the workflows to recordworking distance. Using the correctmagnification factor of an OPMI ismoved into position by the dentist andimages. Video recording of treatmentindividual working distance on an OPMIvariable between approximately 1.5 -then remains stable. Special optics allowhas to be done by a third party.is crucial for a correct working posture.30 times and can be altered by usingthe working distance to be changedConversely with an integrated cameraUsing an OPMI supports the ergonomicsthe magnification changer or zoomto ensure a comfortable workingor with still or video cameras attachedof the dentist as the microscope cansystem, depending on the model ofposture of the dentist. The higher theto the OPMI, images or video recordingsmore or less look “around the corner”.OPMI. While an overview of the mouthmagnification of loupes, the heavierof exceptional quality can be obtainedTherefore, the dentist can sit uprightcan be seen at lower magnifications,they become and therefore potentiallywhile treatment is being carried out.and benefits from good ergonomics.detailed structures can be viewedmore uncomfortable. Modern loupesbetter using the higher magnificationalso have a battery operated headlightof an OPMI, e.g. to locate a root canal,which needs to be rechargedor to find additional root canals. Thisperiodically.2627
1 The OPMIThe human eye – how it works and why it is limitedOptical axisSmallworkingdistanceLarge working distanceLarge angle of viewSmall angle of viewFigure 1.1: The focused object is on the opticalaxis. The farther the object is removed from theeye, the smaller the angle at which it is projectedon the retina. Finer details can be recognized onlyif the object is closer to the eye and thus the angleto the retina is greaterAccommodationStereoscopyThe human eye is a flexible opticaldepicted on the retina with a small anglenear objects. The ability to see detailedThe fact that we have two eyes thatan instrument is in front of, next to orsystem that can adapt to variousof view. To be able to see fine details,structures also begins to deteriorate. Anare adjacent to one another forms thebehind an anatomical structure. In orderrequirements. It can produce an imagewe have to bring the object closer toOPMI overcomes these natural limitations.basis of stereoscopic vision. The left andto enable this orientation, OPMIs areof objects at a great distance, but wethe eye. As a result, the angle of viewOn the one hand, it magnifies detailedright eyes perceive a particular objectdesigned as stereomicroscopes. Thiscan also read a text that is onlyincreases and we can break down thestructures, and the fine structures canfrom two different angles (parallax).enables the left and right eyes to view30 cm away. The eye adjusts to variousindividual structures (Figure 1.1). This isthen be distinguished. On the other hand,The brain then puts these two slightlyan object from slightly different angles.distances. In order to focus objects atwhy a dentist has to bend down over thethe eye can adjust almost to infinity whendifferent sets of visual informationWe can then retain three-dimensionalvarious distances, a system of musclespatient’s oral cavity in order to be able tolooking through an OPMI. This relaxes thetogether to form a 3D image. Thisvision and this depth perception whengenerates the required refractive powersee details at a distance of approximatelyciliary muscles and fatigue symptoms areallows us to see the third dimension, tolooking through the OPMI.for the lenses of the eyes. If we look30 cm. The easiest type of magnificationreduced.estimate distance, size and position andat a landscape, the ciliary muscle isis therefore to bring an object closer toto orientate ourselves. We also requirerelaxed and the lens is flat. However,the eye. However, the eye’s abilities arethree-dimensional image informationif we read text, the ciliary muscleslimited. A baby can clearly see objectswhen looking at a treatment area. Onlycontract, causing the lens to becomethat are 7 cm away, a 30 year-old personwith three-dimensional vision are weconvex. The refractive power is thusat 30 cm. On reaching the age of 40,able to determine whether the tip ofincreased and we can clearly recognizemost people become presbyopic andsmall letters. Extended contraction ofthe distance between the object andthe ciliary muscle can cause fatigue. Inthe eye becomes increasingly bigger.order to relax the eyes, we look to aThe eye’s ability to accommodate tomore distant scene. If we look at a smallshort distances deteriorates, meaningobject from a greater distance, it isthat we can no longer focus as well on2829
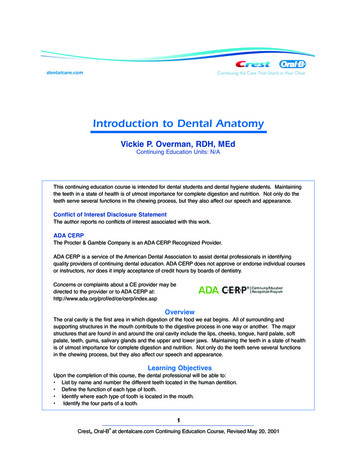
1 The OPMIThe components of an OPMIBefore going into greater detail about the individualcomponents of an OPMI, let us first look at theoptical paths (Figure 1.2).Image planeon the retinaEyepieceIntermediateimage planeTube HeadIf the treatment field is in the focalObjective lensplane of the objective lens, the objectiveThe objective lens is the first opticalthe focal distance, i.e. the workingcomponent that the image informationdistance of the lens, the greater thecrosses on its path from the object toend magnification (for calculation ofthe eye. The lenses vary in their focalthe end magnification, see Sectionbeam splitter can be inserted. Thedistance ( focal length). This influences4.5) and the greater the resolution.magnification changer magnifies orthe working distance (i.e. the distanceThe lens should be equipped with aminimizes the image by a given factor.between the object in the treatmentfine-focus knob. That means that evenThe binocular tube head is placed onfield and the surface of the lens), theat high magnification levels, imageslens creates an image at infinity. Behindthe main objective lens the opticalpaths are parallel. Different componentslike the magnification changer or theOPMI body withmagnfication changermagnification and the resolution. Thesecan be precisely focused over a shorteyepieces for the left and right eyes.three criteria influence one another.distance (e.g. when viewing root canalsThe two optical paths provide slightlyThe most common working distancesin great detail). To change the workingdifferent viewing angles, which createsare 200, 250 and 300 mm. The focaldistance, the lens must be unscreweddistance of e.g. f 250 mm is engravedand replaced with an lens with afrom the object. The left and right optical paths inon the lens mount. This roughly equatesdifferent focal distance. However, this isis referred to as the stereo base. Thethe OPMI view different angles of the object andto the working distance of the lens.impractical in practice and interrupts thestereo base is essential for producing athus create the impression of a three-dimensionalIn order to view the image clearly, theworkflow. A varioscope is useful in thisimage depending on the selected position. TheOPMI lens ( e.g. f 250 mm) must haveevent and offers much more flexibilitytube creates an intermediate imagetube lens of the binocular tube head creates ana working distance of approximatelyas it can change the working distancewhich is magnified by the eyepiece andintermediate image of the object, which is projec-250 mm to the object. The object iscontinuously.the OPMI body and contains the twothe stereoscopic image impression. Thedistance between the two optical pathsthree-dimensional image. The binocularprojected onto the exit pupils. The lensof the eye then receives the image andfocuses it on the retina.LensFigure 1.2: The lens collects the image informationimage. The magnification changer magnifies theted into the eye, magnified with the eyepiece. Thethe right way. The tube head allows adjustment ofThe OPMI can be raised or loweredthe pupil distance, so that the pupils of the viewerto focus the object, provided the lensmatch the OPMI‘s exit pupils30then within the focal point of the lens.prisms in the binocular tube head rotate the imageObject planehas been set to a distance of e.g.250 mm from the object. The shorter31
1 The OPMIInternal displacementof the lens systemFigure 1.4: The working distance can be changedaccording to the internal displacement of thevarioscope’s second lens system. There are motorized varioscopes which focus on the image at thepress of a button. Therefore, the dentist can focusLarge workingdistancewithout changing his or her own seated position.The height of the OPMI can be set in a range fromSmall workingdistance200 to 415 mm, e.g. above the patient‘s oral cavity.This allows the dentist to adjust the OPMI to suit hisor her individual ergonomic needsObject planeFigure 1.3: Using Varioskop 100 of OPMI pico thedentist can focus continuously, for example, fromthe incisors to the molars in the patient‘s oral cavityVarioscopewithout changing the position of the OPMI. Theheight of OPMI pico can be set in a range from 200to 300 mm above the patient‘s oral cavity allowingUnlike an objective lens with fixed focaladaptation to the personal ergonomic needs of thelength, a varioscope has a variabledentist.focal length. Therefore, it can be set toa range of working distances to meetdifferent application and ergonomicrequirements. The focal range of aup and down results in much moremotorized varioscope of OPMI PROergo,Figures 1.5a, 1.5b: OPMI PROergovarioscope can be varied from 200 toprecise focusing and speeds up theit can be controlled by pressing acomes with a motorized varioscope.300 mm or even from 200 to 415 mmworkflow. How is this possible? The lensbutton on the handgrip (Figure. 1.5).depending on the OPMI. This ensuressystem of a varioscope is composed ofThis makes the workflow more efficienta wide range of working distances fortwo lens groups. To focus at a selectedand contributes significantly to thea comfortable working position, evenworking distance, the upper lens groupergonomics of the OPMI. Automaticfor hours at a time. Unlike an OPMIis repositioned along the optical axisfocus is even more convenient.with a fixed focal length lens, it is not(Figure 1.4). The adjustment of theBy pressing a single button, the ZEISSnecessary to raise or lower an OPMIfocal plane within the working distanceSpeedFocus system of the OPMIwith a varioscope to focus it within itsrange can be performed manuallyPROergo focuses the OPMI in a matterfocal range. For example, it is possible(S100 / OPMI pico with Varioskop 100)of seconds by analyzing live imagesto focus by turning the focus knob ofor motorized (S7 / OPMI PROergo).recorded by a camera.the varioscope from the incisors toWhen using a manual Varioskop 100the molars in the patient’s oral cavityon OPMI pico, it can be controlledwithout moving the OPMI. Using theby manually turning the knob on thevarioscope instead of moving the OPMIvarioscope (Figure 1.3). When using a32The dentist can vary the workingdistance over a range of200 – 415 mm by using thecontrol button of the handgrip33
1 The OPMIFigure 1.6: A five-step magnification changer iscomposed of a turret with two telescopes and oneposition without a lens. Depending on the positionof the magnification changer in the optical path,there are different magnification factors.The factor in the lens-free position is 1.Zoom systemMagnification changerDuring treatment it is importantempty position without optics thatThe advantage of step magnificationZoom systems allow the magnificationA zoom system shows its fullthat the magnification factor can beprovides a magnification factor of 1.changers is their compact constructionof the overall system to be set aspotential when motorized as inaltered to gain an overview at lowerTherefore, a total of 5 magnificationwith low technical complexity, yetrequired by the treatment. The dentistS7 / OPMI PROergo:magnifications and to view in morefactors are available. Usually thehigh optical quality and efficiency. Thecan continuously change between stepless zoomdetail at higher magnifications. Theremagnification factors are 0.4, 0.6,limitation is that magnification canoverview and a detailed view. As with faster adjustment of magnificationare two technical solutions for this1.0, 1.6, 2.5. (Please note that theseonly be selected in steps, and the viewthe magnification changer, the zoom control via multi-functional handgrippurpose: the magnification changernumbers are not the end magnifications.of the treatment area is blocked whileratio (1:6) can be calculated by dividing control via foot switch. If the dentist( Galilean changer) and the steplessTo calculate the end magnification,the turret is being turned. Turningthe highest magnification factor (2.4) byuses a foot switch, he or she canzoom system. The majority of OPMIs arefurther optical parameters must bethe magnification factor must bethe smallest (0.4). The zoom system isadjust the zoom factor without havingfitted with a magnification changer. Theconsidered, as described in Section 4.5).performed manually. Zoom systems arecomposed of several optical elements,to take their hands off the instrument.most common magnification changerThe ratio between the largest and theconsiderably more convenient.of which two are adjustable. By alteringhas 5 steps. The optical principle issmallest magnification factor gives thethe position of the two adjustablechecked: in combination with anan astronomical telescope, called theextension range of the magnificationelements over a precisely calculatedinternal video camera, the endGalilean telescope after its inventor.changer: 2.5 / 0.4 6.25curve, the various magnification factorsmagnification or a scale bar can beThe magnification ratio is 1:6.25.can be achieved smoothly along the the magnification level can bedisplayed on the monitor. For the purposes of documentation,The magnification changer is composedmagnification range. In order to achieveof a turret with two telescope systemsthe stereoscopic effect, there are twothe image section can be optimallyof different magnification factorsparallel optical paths in the zoom systemadjusted to the size of the camera(Figure 1.6). By turning the turret thethat must behave absolutely identicalsensor, so that a tooth, for example,telescopic systems can be viewed inwith regard to their optics and precision.can be displayed to fill the wholeeither direction to achieve differentphoto or monitor.magnification factors. There is a totalof four magnification factors plus one3435
1 The OPMIFigure 1.7a: For more user comfort, the distance to theFigure 1.7b: The foldable tube f170 / f260 head accommodates easily to the various ergonomics ofsurgical field can be adjusted as needed with thedifferent operators. Both dentists can work with the same working distance as the different eye levels ofmulti-link design of the foldable tube f170/f260 head.the dentists are compensated for by the adjustable foldable tube f170 / f260 head. The foldable tube headcan be mounted to OPMI pico or OPMI PROergoEyepiecesBinocular tubeOPMIs are used in an almostlong reach and multilink design thisJust like a magnifying glass, the twoability is limited and the dentist needsperpendicular position above thetube head accommodates differenteyepieces magnify the intermediateto be able to see normally when notpatient in dentistry. In order to provideergonomics of different operators orimage produced in the tube.looking through the OPMI. Certain eyethe dentist with a comfortable anddifferent positions of the patient.problems, e.g. astigmatism, cannotThe magnification factor (10x or 12.5x)be corrected by the eyepiece. If theFigure 1.8: The blue circle corresponds to theinclinable or foldable tube head isThe tube head also uses the stereoscopicis labeled on the eyepieces. Thus, therefractive error of the eye is correctedfield of view of a 10x eyepiece and the redmounted to the OPMI body and directsprinciple of the left and right opticaleyepieces have an effect on the endby prescription lenses, the dioptriccircle corresponds to the field of view of athe optical path to the eyes of thepath for a three dimensional image.magnification. Anyone requiring as highcorrection of the eyepiece should bedentist. A 45 inclined tube head isThe binocular tube head contains a lensa magnification as possible (e.g. forset to 0. The dentist’s eyes must be atfixed at an angle of 45 and offersand has a defined focal distanceendodontics) will choose eyepieces witha certain distance to the eyepieces sothat, conversely, the maximum final magnificationlimited ergonomics. A inclinable tube(e.g. f 170 mm as shown on the tube12.5x magnification. Eyepieces with 10xthat they are in the exit pupils of theis higher when using a 12.5x eyepiecehead (0-180 ) allows the dentist tohead). Prisms inside the tube headmagnification do, however, provide aeyepieces and can see the entire field ofalter the angle of the eyepiece holderscreate an upright, accurate image. Theconsiderably larger field of view, and canview. Eyecups or distancing rings shouldby 180 . That means that the viewingeyepieces in the binocular tube head aretherefore provide a better overview ofbe extended when using the OPMIangle of the tube can be adjusted to thethe interface between the OPMI and thethe entire treatment area (Figure 1.8).without glasses. Dentists who wearposition of the OPMI in such a way thatdentist’s eyes. The distance between thethe dentist’s head can remain uprightpupils varies from person to person andEyepieces are fitted with a ring forrings as the glasses already functionand the dentist does not have to leanranges from 54
valuable guide to using the surgical microscope in a range of dental applications. The articles were written with the idea in mind that they shall enable a step-by-step implementation that unlocks the full potential of surgical microscopy in your d