Transcription
Maintenance and Removal ofCentral Venous Catheters1
PresenterKaren Jones, RN, MPH, CICClinical Research Project CoordinatorUniversity of MichiganContributions byVineet Chopra, MD, MScUniversity of MichiganKristi Felix, RN, BSN, CRRN, CIC, FAPICMadonna Rehabilitation HospitalLen Mermel, DO, ScM, AM (Hon)Medical School of Brown UniversityRuss Olmsted, MPH, CIC, FAPICTrinity Health, Livonia MIPayal Patel, MD, MPHUniversity of Michigan2
Learning Objectives Discuss components of the central venous catheter(CVC) maintenance bundle Outline issues to address during the transition ofcare of a patient with a CVC Describe strategies to promote the removal ofunnecessary CVCs3
Impact of Infection CLABSIs result in increased mortality and health carecosts Of all healthcare-associated infections, CLABSIscause the highest number of preventable deaths 65% 70% of CLABSIs can be prevented byimplementing evidence-based practices(APIC Implementation Guide: Guide to Preventing Central Line-Associated Bloodstream Infections, APIC, 2015)4
Targeting Maintenance and RemovalStandardize CVCmaintenance carewhere possibleMaintain awareness ofCVCs that are in placeRemove CVC when nolonger necessary(Meddings J, Saint S. Disrupting the life cycle of the urinary catheter. Clin Infect Dis.2011;52(11):1291-3. PMID: 21596672)5
Case Study: MaintenanceMrs. Smith is admitted to the ICU following a motorcycle accident– Traumatic brain injury– Compound open fracture of femur, rib fractures– Requires mechanical ventilationHas an internal jugular CVC for hemodynamic support and antibioticadministration.Question: What are the CVC maintenance priorities for thispatient?Disclaimer: All case studies are hypothetical and not based on any actual patient information. Any similaritybetween a case study and actual patient experience is purely coincidental.6
Maintenance Bundle of CareConduct daily assessments of thenecessity of CVCs, with promptremoval if no longer neededAccess ports of entry with aseptictechniquePerform proper care of infusiontubingAssess and care for central venouscatheter dressings(Checklist for Prevention of Central Line Associate Blood Stream Infections, CDC, 2011)7
Basics to Consider(Marschall J, Infect Control Hosp Epidemiol, 2014)8
Daily Assessment of NecessityAssess necessity of CVC daily with a multidisciplinary teamIndications for ongoing use can include:– Clinical instability of the patient– Prescribed continuous or intermittent infusion therapy– Hemodynamic monitoring– Documented history of difficult peripheral venous accessUse tools like electronic medical record reminders, dailyrounding forms or checklists to prompt discussion among staffand leaders(Gorski L, J Infus Nurs, 2016)9
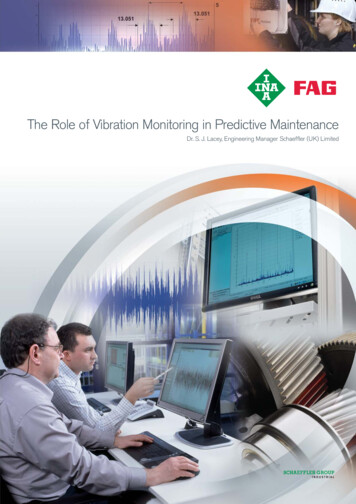
Example of CVC Necessity Tracking ToolReview Daily with Physician for Central Line Necessity Tracking ToolPatient Name:Central Line Insertion Date:DateTime(check once per day)Room #D/C Central Line Date:Necessity of Central Line ReviewedIndication for Central Line Use/Continued Use(see list below)MR #If no longer indicated, is there a plan to removeCentral Line?Yes NoYes No N/AYes NoYes No N/AYes NoYes No N/AYes NoYes No N/AYes NoYes No N/AYes NoYes No N/AYes NoYes No N/AYes NoYes No N/ARN SignatureINDICATIONS FOR CENTRAL LINE USE/CONTINUED USE: (List all that apply)1. Prolonged IV therapya. Antibioticsb. Total parenteral nutritionc. Chemotherapy2. Irritating medications3. Poor peripheral venous accessComment: Blood sampling is not indication for a central line unless there is poor peripheral venous access4. Critical illness requiring central venous accessa. Hemodynamic monitoringb. Vasoactive drips5. Hemodialysis or plasmapheresisModified from IPRO's "Review Daily With Physician for Foley Catheter Necessity" Tracking Tool.(Used with permission: New York State Partnership for Patients and IPRO. Review Daily with Physician for Central Line Necessity Tracking Tool [NYSPP],adapted from Review Daily With Physician for Foley Catheter Necessity Tracking Tool [IRPO]. Accessed [date] athttp://www.nyspfp.org/Materials/Central Line Necessity Tracking Tool.xlsx.10
Proper Access of CVCAccess CVC only with sterile devices“Scrub the hub” vigorously for at least 5 seconds withan appropriate antiseptic and allow to dry prior toevery accessAssess patency of lines by flushing and aspirating forblood returnMinimize the interruptions of the CVC– Maintain a closed system as much as possible– Minimize frequency of tubing disconnects and flushing(Gorski L, J Infus Nurs 2016; Marschall J, Infect Control Hosp Epidemiol,2014; O’Grady NP, Am J Infect Control, 2011)11
CVC Infusion TubingReplace administration sets not used for blood, blood productsor lipids at intervals of no more frequently than every 96 hoursbut at least seven days– Includes secondary piggyback sets attached to primary continuous setif it remains connectedReplace tubing used to administer Propofol infusions every 6 or12 hours, per the manufacturers’ recommendations or when thecontainer is changedChange needleless components at least as frequently as theadministration set– There is no benefit to changing these more frequently than every 72hours(Gorski L, J Infus Nurs 2016; O’Grady NP, Am J Infect Control, 2011)12
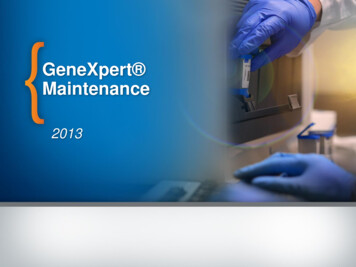
CVC Dressing ChangeAssess dressing status at least dailyReplace dressing:– Every 2 days for gauze dressings– Every 7 days for transparentdressings– And whenever dressing becomesdamp, loosened or soiledUse aseptic technique and prepareclean skin with greater than 0.5%chlorhexidine with alcohol(O’Grady NP, Am J Infect Control, 2011)13
CVC Dressing Change (Continued)Document date and timeon dressingDo not disturb or changea clean, dry, intactdressing until the duedate14
Case Study: Transfer of CareTracheotomy placed for continuous ventilator supportNeurological status remains poorDiagnosed with osteomyelitisPeripherally inserted central catheter (PICC line) placed for long-termcourse of antibioticsMrs. Smith to be transferred to LTACHQuestion: What aspects of care coordination for the centralline need to be addressed upon transfer?Disclaimer: All case studies are hypothetical and not based on any actual patient information. Any similaritybetween a case study and actual patient experience is purely coincidental.15
Care Coordination of Central LineKey details to communicate:– Initial indication for CVC If for antibiotics, the date they were started and reason fortreatment– Date that the line was placed– Date that the dressing and tubing were last changed– Issues with patency of lumensOngoing assessment of necessity should occur in the new care settingDisclaimer: All case studies are hypothetical and not based on any actual patient information. Any similaritybetween a case study and actual patient experience is purely coincidental.16
Case Study: Removal of LineDay 28: Mrs. Smith is improving and breathing on her own and she ishemodynamically stableAntibiotic course is completed and the infection has resolvedShe is scheduled for routine lab tests every two daysQuestion: Does Mrs. Smith need to continue to have a PICCline in place? Can the line be removed?Disclaimer: All case studies are hypothetical and not based on any actual patient information. Any similaritybetween a case study and actual patient experience is purely coincidental.17
Removal: A Bundle ElementMichigan Keystone ProjectDecrease in CLABSIs in 103 ICUs in Michigan (66%reduction)––––––Hand hygieneFull barrier precautions during central line insertionSkin cleansing with chlorhexidineAvoiding femoral siteRemoving unnecessary cathetersUse of insertion checklist(Pronovost P, N Engl J Med, 2006)18
MAGIC Criteria for Ongoing PICC UseAppropriate Indications for PICC useDelivery of peripherally compatible infusates when the proposed duration of such use is 6 daysDelivery of non-peripherally compatible infusates (e.g., irritants or vesicants), regardless ofproposed duration of useDelivery of cyclical or episodic chemotherapy that can be administered through a peripheral vein inpatients with active cancer, provided that the proposed duration of such treatment is 3 monthsInvasive hemodynamic monitoring or requirement to obtain central venous access in a critically illpatient, provided the proposed duration of such use is 15 daysFrequent phlebotomy (every 8 hours) in a hospitalized patient, provided that the proposedduration of such use is 6 daysIntermittent infusions or infrequent phlebotomy in patients with poor/difficult peripheral venousaccess, provided that the proposed duration of such use is 6 daysFor infusions or palliative treatment during end-of-life careDelivery of peripherally compatible infusates for patients residing in skilled nursing facilities ortransitioning from hospital to home, provided that the proposed duration of such use is 15 days(Chopra V, Ann Intern Med, 2015)19
Barriers to CVCMaintenance and Removal Difficulty engaging physicians and nurses Lack of insertion and maintenance supplies Lack of knowledge and skill regarding CVC careand maintenance processes Poor communication across the continuum ofcare20
Solutions for Improvement Use data to drive action: monitor and share CVCutilization and infection data Standardize where you can– Pre-packaged dressing change kits– Protocols for care processes Audit adherence and provide with “just-in-time”education and feedback Address CVC need at every hand-off21
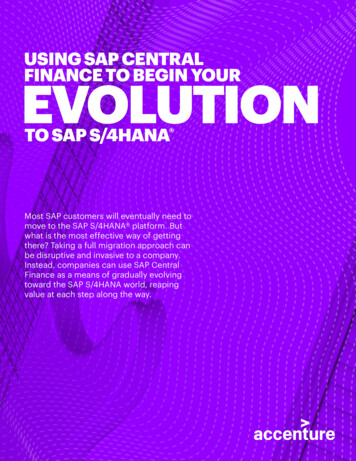
Tools for ImprovementCDC TAPDays Since Last CLABSI. Eliminate HarmAcross the Board.22CLABSI Surveillance. Dressing IntegrityObservation Audit. University ofRochester.
SummaryUse a bundled approach to improve CVC maintenance andremoval practicesAddress of CVC care for patients that move from one care settingto anotherTo overcome barriers, use strategies that involve data, audits,feedback and standardize care and supplies where possible23
ReferenceAPIC Implementation Guide: Guide to Preventing Central Line-Associated Bloodstream Infections.Association for Professionals in Infection Prevention and Epidemiology, APIC. 2015.http://apic.org/Resource /TinyMceFileManager/2015/APIC CLABSI WEB.pdfCDC Targeted Assessment for Prevention (TAP) CLABSI Implementation Guide. Centers for DiseaseControl and Prevention, CDC. Available at cklist for Prevention of Central Line Associate Blood Stream Infections. Centers of Disease Controland Prevention, CDC.2011. Available at bsi.pdfChopra V, Flanders SA, Saint S, et al. The Michigan Appropriateness Guide for Intravenous Catheters(MAGIC): Results from a multispecialty panel using the RAND/UCLA appropriateness method. AnnIntern Med. 2015; 163(6): S1-S40.CLABSI Surveillance. Dressing Integrity Observation Audit. University of Rochester. Available ocuments/dressingintegrityaudit.pdfDays Since Last CLABSI. Eliminate Harm Across the Board. Available -attachments/6.clabsi days between events.pdfGorski L, Hadaway L, Hagel M, et al. Infusion Therapy, Standards of Practice. J Infus Nurs. 2016;39(1S): S1-169.24
Reference (cont’d)Healthcare Infection Control Practices Advisory Committee (HICPAC), 2011 Guidelines for thePrevention of Intravascular Catheter-Related Infections. Am J Infect Control. 2011; 39: 3(11)00085-X/fulltextKane RL, Shamliyan TA, Muella C, et al. The association of registered nurse staffing levels andpatient outcomes: systematic review and meta-analysis. Med Care. 2007; 45(12): 70Marschall J, Mermel LA, Fakih M, et al. Strategies to Prevent Central Line–Associated BloodstreamInfections in Acute Care Hospitals: 2014 Update. Infect Control Hosp Epidemiol. 2014; 35(7):753-71.Meddings J, Saint S. Disrupting the life cycle of the urinary catheter. Clin Infect Dis.2011;52(11):1291-3. PMID: 21596672.O’Grady NP, Alexander M, Burns LA, et al. Guidelines for the prevention of intravascular catheterrelated infections. Am J Control. 2011; 39(4 Suppl 1): S1-34.Pronovost P, Needham D, Berenholtz S, et al. An Intervention to Decrease Catheter-RelatedBloodstream Infections in the ICU. N Engl J Med. 2006; 355(26): 2725-32.Review daily with physicians for central line necessity tracking tool. New York State Partnershipfor Patients, accessed [date] athttp://www.nyspfp.org/Materials/Central Line Necessity Tracking Tool.xlsx.25
Speaker Notes26
Speaker Notes: Slide 1This module, titled “Maintenance and Removal of CentralVenous Catheters,” will review key steps and strategies to ensureproper maintenance and removal of central venous catheters.27
Speaker Notes: Slide 2This module was developed by national infection preventionexperts devoted to improving patient safety and infectionprevention efforts.28
Speaker Notes: Slide 3After completing this module you will be able to: Discuss components of the central venous cathetermaintenance bundle; Outline issues to address during the transition of care of apatient with a central venous catheter; and Describe strategies to promote the removal of unnecessarycentral venous catheters.29
Speaker Notes: Slide 4To begin our discussion of maintenance and removal of centralvenous catheters, let’s review the impact of central lineassociated bloodstream infections, or CLABSIs. Data show thatCLABSIs result in a higher rate of mortality for patients andincreased health care costs. Of all the healthcare-associatedinfections, CLABSIs cause the highest number of preventabledeaths. But the good news is that by implementing evidencebased practices, 65 to 70 percent of CLABSIs can be prevented.30
Speaker Notes: Slide 5Other modules for this course describe appropriateness ofcentral venous catheters and best practices for insertion. Thismodule will focus on best practices for maintenance and removalthat hospital teams should implement as part of their CLABSIprevention program. This includes standardizing CVCmaintenance care where possible, maintaining awareness ofCVCs that are in place, and promptly removing CVCs when nolonger necessary.31
Speaker Notes: Slide 6Let’s consider a case study to help illustrate commonmaintenance and removal issues for central venous catheters.Mrs. Smith is a 52-year-old woman who was just in a severemotorcycle accident. Mrs. Smith suffered a traumatic braininjury, multiple rib fractures and a compound open fracture ofher right femur. In the emergency department, an internaljugular, or IJ central line was placed for infusion of fluids andvasopressors for her hypotension and antibiotics for her openfracture. The patient is admitted to the ICU.Question: What are the CVC maintenance priorities for Mrs.Smith?32
Speaker Notes: Slide 7To answer that question, we can look at maintenance practicesusing a bundled approach. There are four practices to consideras priorities for CVC maintenance.First, conduct a daily assessment of the necessity of CVCs, withprompt removal if no longer needed. In some cases—like ourcase study, for example—in some cases, lines placed emergentlycan require closer monitoring since adherence to aseptictechnique in emergencies can be variable. Second, always accessports of entry using aseptic technique. You also want to ensureproper care of infusion tubing, assessment, and care for CVCdressings. By ensuring that these basic practices occur in aconsistent way, we can reduce harm to patients.33
Speaker Notes: Slide 8There are some basic practices that we need to consider whenpreventing central line infections. Anyone accessing ormanipulating a CVC must perform hand hygiene prior toperforming line care. Clinicians that are involved in the lineinsertion, removal or dressing change, should don properpersonal protective equipment (PPE) including sterile gloves,masks and gowns. To ensure that staff are properly trained inthese and other CVC practices, they should receive competencybased training for aspects of both line insertion andmaintenance.34
Speaker Notes: Slide 8 ContinuedThis includes aseptic technique for insertion and properassessment of insertion site and dressing integrity. For criticallyill patients that are at higher risk of developing central lineinfections, staffing should ensure appropriate nurse-to-patientratio. And finally but just as important, hospitals need to engagepatients and families by providing them education about centrallines and encouraging them to speak up when they haveconcerns about CVCs.35
Speaker Notes: Slide 9Now that we have discussed the basics, let’s look at some of thekey components of the maintenance bundle. An important stepto preventing CLABSIs is to conduct a daily assessment of CVCnecessity. On each day of CVC use, a multidisciplinary team ofphysicians and nurses should review and discuss to meet theindications for ongoing need of the device. Indications ofongoing need can include clinical instability of the patient,receiving continuous or intermittent infusion therapy,hemodynamic monitoring or the patient may have adocumented history of difficult peripheral venous access. Formore information about CVC appropriateness, please reviewmodule CLABSI102.36
Speaker Notes: Slide 9 ContinuedThere are many different tools to help promote the dailyassessment of CVC necessity. These can include daily promptsbuilt into the electronic medical record (EMR) and roundingforms or checklists that help generate discussion among theteam caring for the patient. Electronic medical record promptscan help highlight assessment criteria, ensure accuratedocumentation of necessity and support monitoring ofadherence to best practices. Use of a rounding tracking tool orchecklist ensures that all important items are covered in thedaily discussion.37
Speaker Notes: Slide 10Here is an example of a rounding tool that can be used duringmultidisciplinary rounds to help address the ongoing need forthe CVC and prompt removal if it is no longer needed. Ask for theinput of your relevant clinical team members (including unitmanager and critical care staff) that the tool you decide to use isappropriate and useful for your hospital.38
Speaker Notes: Slide 11Another important aspect of CVC maintenance is accessing theline using aseptic technique. Disinfecting the connection siteprior to accessing the CVC reduces the risk of pathogencontamination to the internal lumen of the catheter, which canlead to infection. Before accessing catheter hubs, needlelessconnectors or injection ports, vigorously apply mechanicalfriction or “scrub the hub” for no less than five seconds with anantiseptic such as alcoholic chlorhexidine preparation, 70percent alcohol, or povidone-iodine and allow it to dry.39
Speaker Notes: Slide 11 ContinuedSome hospitals now use connector access devices like alcoholimpregnated port protector caps. If using these devices, makesure staff are properly trained to follow the manufacturer’srecommendations for use. To help maintain patency of the CVC,it should be flushed per hospital protocol and all ports assessedon a regular basis. Finally, try to access the CVC and access onlywhen absolutely necessary. Consider consolidating lab draws andswitching IV meds to oral when appropriate.40
Speaker Notes: Slide 12CVC infusion tubing or administration sets should be changedper established guidelines. The timeframes are dependent onthe type of fluid being infused and potential rate of bacterialgrowth associated with that fluid. For administration sets notused for blood, blood products or lipids, tubing should bechanged at intervals no more frequently than every 96 hours butat least seven days. For infusions of propofol, the tubing shouldbe changed every six to 12 hours, per the manufacturers’recommendations or when the propofol container is replaced.Hub, connector or ports should be changed at least as frequentlyas the administration set, but no more frequently than every 72hours, unless specified by the manufacturer.41
Speaker Notes: Slide 13Another important aspect of the maintenance bundle is CVCdressing care. Nurses should assess the status of the dressing atleast daily, and some hospitals promote assessment every shift.Dressings should be changed every two days for gauze dressingsand every seven days for transparent dressings. If a dressing isdamp, loosened or soiled it should be changed immediately.42
Speaker Notes: Slide 13 ContinuedClinicians should use aseptic technique when performingdressing changes. This includes wearing sterile gloves and amask. An alcohol chlorhexidine solution should be used for skinantisepsis during dressing changes. Standardizing these productswithin a pre-made kit can help promote adherence with thesepractices.Auditing adherence with dressing change practices can provideopportunities for quality improvement and staff education. Onthe right side of the slide is an example of a dressing integrityaudit tool that can be used.43
Speaker Notes: Slide 14Here are a couple of other important aspects of CVC dressingcare to keep in mind. First, be sure to have clear documentationof the date the dressing was changed or change due date (asfacility policy dictates). And remember, unless loose, damp orsoiled, do not disturb or change a dressing until the necessarydue date. Changing CVC dressings too frequently can increasethe risk of introducing bacteria to the entry site.You can see in the images on the slide how a dressing should bedated and timed.44
Speaker Notes: Slide 15Now we’ll return to our case study. After five days in the ICU,Mrs. Smith is unable to be weaned from the ventilator andreceives a tracheotomy for continued ventilator support. She ishemodynamically stable, but her neurological status remainspoor and after developing a fever, blood cultures and CT scanshow that she has developed MRSA osteomyelitis in her injuredright femur.45
Speaker Notes: Slide 15 ContinuedThe team inserts a peripherally inserted central catheter, or PICCline, and removes the internal jugular central line. On day eight,the patient’s neuro and respiratory status remain unchanged andthe decision is made to move the patient to the long-term acutecare hospital or LTACH, for continued support.Question: What aspects of care coordination regarding thecentral line need to be addressed upon transfer?46
Speaker Notes: Slide 16In preparation for receiving Mrs. Smith, the LTACH admissionnurse calls the ICU to receive her report. When coordinating thecare of a patient with a CVC from one care setting to another,there are important details that must be communicated.These include describing what the initial indication for the CVCwas. Why did the patient need the central line? And why is it stillin place? If the CVC is being used for antibiotic infusions, be sureto share the date the antibiotic was started, the duration oftreatment, the antibiotic dose, and the reason for the antibiotictreatment.47
Speaker Notes: Slide 16 ContinuedOther key information to share across care settings is the datethat the CVC was placed and the date the dressing andadministration tubing were last changed. Also report any issueswith patency of the lumens. If the CVC will remain in place afterthe transfer of care, the accepting care location should continueto assess the necessity of the line on a daily.48
Speaker Notes: Slide 17By day 28, Mrs. Smith’s neurological status is beginning toimprove and she is now able to breathe on her own without theassistance of the ventilator. She is hemodynamically stable andhas completed her course of antibiotics. Her most recent bloodcultures were negative and CT scan shows her osteomyelitis isresolved. She is scheduled for routine blood testing every twodays.Does Mrs. Smith need to have a PICC line in place? Or can theline be removed?49
Speaker Notes: Slide 18As was shown by the Michigan Keystone Project, central linebundles including removal of unnecessary CVC’s reduce CLABSIs.50
Speaker Notes: Slide 19The beginning of this module explored the importance ofassessing CVC necessity and removing lines that are not needed.The Michigan Appropriateness Guide for Intravenous Cathetersor MAGIC Guidelines published by Chopra and his colleagueswere discussed in more detail in CLABSI102. The guidelinesoutline appropriate indications for PICC use and help to provideclinicians evidence-based criteria to guide their decision-making.Reviewing the appropriate indications on this slide, we can seethat Mrs. Smith does not meet any of these criteria and,therefore, her PICC line should be removed.51
Speaker Notes: Slide 20This module describes many different practices to help improvemaintenance and promote appropriate removal of CVCs. Let’sconsider some of the barriers that hospitals may encounterwhen implementing these practices. Sometimes it can be difficult to engage physicians and nurses inchange. Changing practices for CVC maintenance and removalmay be met with resistance from clinicians, which will need tobe addressed to implement sustainable change.52
Speaker Notes: Slide 20 Continued Lack of adequate supplies can also present a barrier. If a cliniciandoes not have access to the supplies they need, it can makecompleting a task like a dressing change more difficult. Lack of skill and knowledge of staff regarding CVC care andmaintenance processes can be another significant barrier. If staffdo not demonstrate competency for aseptic technique, CVC siteassessment, dressing care and appropriate indications, thepatient could be at increased risk of harm. Poor communication across care settings, for example, about thepatient’s CVC need, is sometimes poor. Hospital teams shouldassess communications and other barriers a their facility andcreate plans for improvement to overcome these challenges.53
Speaker Notes: Slide 21Some possible solutions to consider are: Using data to drive action. Engage staff by sharing infection anddevice utilization data with them in real time. Share data that are unitspecific and when infections do occur, involve staff in the root causeanalysis to identify contributing factors and recommendations forimprovement. Standardize where you can. Make it easy for staff to do the right thingby standardizing supplies. For example, use all-inclusive dressingchange kits and keep them stocked in a location that is close to thepoint of care. Develop standardized protocols for care and maintenanceprocesses. For example, consider a protocol that states that all CVCdressings are routinely changed on the same day of the week unlessthey are loose, damp or soiled.54
Speaker Notes: Slide 21 Continued Audit staff adherence with practices and provide “just-in-time”education and feedback. Audit care and maintenance practices,including assessment of condition of dressings, and adherence toscrubbing the hub prior to accessing the line. Use results to educateand coach staff. For more ideas on auditing best practices, pleasereview the foundational course on competency-based training, auditsand feedback. Finally, make sure to address CVCs at every hand-off opportunity.Clinicians should consider the continued need for CVCs at everytransfer of care. As we saw in the case study, when patients aretransferred to different care settings, there is critical information thatshould be shared to ensure continuity of care.55
Speaker Notes: Slide 22Here are a couple of examples of tools that you might findhelpful. On the left is a poster that displays the number of dayssince a unit’s last CLABSI. This is a great visual way to engagestaff in their CLABSI improvement efforts. On the right is a CVCdressing integrity audit tool from the University of Rochester.These tools and more can be found online at CDC’s TAP CLABSIImplementation Guide.56
Speaker Notes: Slide 23In summary, this module described how to use a bundledapproach to improve CVC maintenance practices; shared how toaddress CVC care for patients that move from one care setting toanother; and finally, outlined several strategies that can be usedto improve maintenance and ensure prompt removal of CVCs.57
Speaker Notes: Slide 24No notes.58
Speaker Notes: Slide 25No notes.59
Maintenance Bundle of Care. Conduct daily assessments of the necessity of CVCs, with prompt removal if no longer needed. Access ports of entry with aseptic technique. Perform proper care of infusion tubing . Assess and care for central venous catheter dressings . 7 (Checklist for Prevention o