Transcription
HandbookPublic Health ERUCommunity Based Surveillance (CBS)Group lead:Group members:IFRC focal point:Norwegian Red Cross (focal point: PHiE Coordinator, Tonje Tingberg)Hong Kong Red Cross Society (Focal point, Karen Poon),French Red Cross (focal point, Aude Saintoyant)Belgium Red Cross (focal point, Robert Ghosn)Australian Red Cross (focal point, Lisa Natoli)PHiE senior officer, Gwendolen EAMERBig thank you, to the community-based surveillance technical working group, the public health ERUtechnical working group for good support during the development process. A specific thanks to LisaNatoli, Australian RC, for valuable inputs and support during this development. To Anine Kongelf,Tine Larsen, Roxanne Moore, IFRC, Norwegian Red Cross and all our dedicated delegates and volunteers who has made the development of the Public Health ERU possible.Oslo, November 2019, Tonje TingbergHandbook PHE ERU CBS – revised November 2019Page 1 / 55
ContentsABBREVIATIONS . 4TERMINOLOGY . 61.INTRODUCTION . 7HOW TO READ THIS HANDBOOK. 7BACKGROUND – DEVELOPMENT OF PUBLIC HEALTH ERUS . 8ARTICULATION BETWEEN PH AND CLINICAL ERUS . 92.FRAMEWORK FOR PUBLIC HEALTH ERU’S .12STRATEGIC AND INSTITUTIONAL FRAMEWORK . 12GUIDING PRINCIPLES. 12MINIMUM CORE STANDARDS . 133.THE PH ERU CBS CONFIGURATION .14WHAT IS CBS?. 14PURPOSE AND OBJECTIVES OF THE PH ERU CBS. 14ACTIVITIES. 15KEY CHARACTERISTICS . 15GENERAL DESIGN AND OPERATION. 15LINK TO OTHER SURVEILLANCE SYSTEMS . 164.HUMAN RESOURCES .18PH ERU CBS TEAM PROFILES . 18LOCAL COUNTERPARTS . 21THE DELEGATE TEAM . 21TRAINING OF HUMAN RESOURCES . 22BRIEFINGS, DEBRIEFING & END OF MISSIONS . 23Briefings .23Debriefings .24End of Mission Report .24Handover document .24Performance appraisal .24SAFETY AND SECURITY OF DEPLOYED STAFF . 25REMOTE SUPPORT AND LINES OF COMMUNICATION . 255.EQUIPMENT.25CBS DIGITAL KIT . 26Characteristics:.26Set up .27OTHER EQUIPMENT . 286.FINANCIAL .287.DEPLOYMENT MECHANISM .30DEPLOYMENT FLOW CHART. 30Handbook PHE ERU CBS – revised November 2019Page 2 / 55
ACTIVATION . 30DEPLOYMENT OF ADVANCE TEAM/FEASIBILITY STUDY: . 31Site selection .31Partner capacity .32Advocacy .33DESIGN AND SET-UP: . 33Community Engagement and Accountability (CEA).34IMPLEMENTATION . 35Training of volunteers .36CBS Operation .36Data collection, analysis, reporting and sharing .37Addressing fear and stigma during outbreaks .38Coordination and communication .39Monitoring and Evaluation .40EXIT OF ERU – HANDOVER TO OPERATION/ NS . 41ANNEXES .42ANNEX 1: LIST OF PH ERU CONFIGURATIONS . 42ANNEX 2. PH ERU CBS DELEGATE PERSONAL BOX CONTENT. 42ANNEX 3. CBS DIGITAL TOOLKIT MANUAL . 44Prepared by:Candela Iglesias Chiesa, MPH, PhDAnna Häggblom, MPHGlobal Health AdvisorsHandbook PHE ERU CBS – revised November 2019Page 3 / 55
AbbreviationsAWDAcute Watery DiarrheaCBHFACommunity Based Health and First AidCBSCommunity Based SurveillanceCCMCommunity Case ManagementCEACommunity Engagement and AccountabilityCP3Community Epidemic and Pandemic Preparedness ProgramCTCCholera Treatment CenterDREFDisaster Response Emergency FundDRMDisaster Response ManagementECVEpidemic Control for VolunteersEoMEnd of Mission ReportEMTEmergency Medical TeamsEPoAEmergency Plan of ActionERUEmergency Response UnitEVDEbola Viral DiseaseEWARSEarly Warning and Response SystemFACTField Assessment and Coordination TeamFADFinance and AdministrationGPSGlobal Positioning SystemHMISHealth Management Information SystemHPHealth PromotionICRCInternational Committee of the Red CrossIDSRIntegrated Disease Surveillance and ResponseIFRCInternational Federation of Red Cross and Red Crescent SocietiesIGERImplementation Guide for Epidemic ResponseHandbook PHE ERU CBS – revised November 2019Page 4 / 55
IPCInfection and Prevention ControlM&EMonitoring and EvaluationMoHMinistry of HealthNGONon Governmental OrganizationNSNational SocietyORPOral Rehydration PointORSOral Rehydration SaltPHPublic HealthPNSPartner National SocietyRCRed Cross or Red CrescentSBCCSocial Behavioural Change CommunicationSIMSubscriber Identification ModuleSMSShort Message ServiceSOPStandard Operating ProceduresTLTeam LeaderToRTerms of ReferenceTWGTechnical Working GroupWASHWater Sanitation and HygieneWHOWorld Health OrganizationWORCWorld of the Red CrossHandbook PHE ERU CBS – revised November 2019Page 5 / 55
TerminologyAlert: the message sent by the platform or by an individual to one or several pre-designed people inthe CBS hierarchy, when the number of reports has reached a pre-defined number (e.g. 1 for Ebola ormeasles, but a higher number for AWD).Case: this is part of the facility-based surveillance system and usually refers to clinically or laboratoryconfirmed cases of a disease.Report is the term for the message transmitted from the volunteer to its supervisor on a person in thecommunity who has signs and symptoms meeting the community case definition for a specific healthrisk. A report can also be a message of an unusual event (group of animal or human deaths, floods,fires, etc), as per the particular CBS protocol in that NS.Handbook PHE ERU CBS – revised November 2019Page 6 / 55
PART I Concept and context1. IntroductionHow to read this handbookThis handbook is intended for:a) Delegates trained in Public Health in Emergencies (Tier B) or with equivalent experience andknowledge who will be deployed as part of the PH ERU CBSb) NS staff who will be involved in the set up and/or running of a PH ERU CBS.c) Partner National Societies who wish to set up a PH ERU CBS moduleThe handbook intends to be a guideline for understanding a PH ERU CBS. It is complemented by severalother documents, which are mostly focused on CBS in non-emergency contexts, with which the readershouId become familiar. These documents are cited repeatedly throughout the handbook.BOX 1. KEY CBS DOCUMENTS TO KNOW IFRC. The CBS Guiding Principles. 2017 (revised version 2020). Available in English, French andSpanish IFRC. CBS Assessment Tool and Template. Not published, for internal use only. Available fromPH ERU CBS trainers. IFRC. CBS Protocol tool. Not published, for internal use only. Available from PH ERU CBS trainers.This document is divided into 3 sections, as follows:Part 1 -Concept and context (chapters 1 to 3) lays out the conceptual framework that supports thedevelopment of PH ERU’s, including strategic frameworks, guiding principles and minimum standards.It then focuses on the concept of the PH ERU CBS configuration, explaining what CBS is, the ERU’sactivities and objectives, how it integrates with other ERUs, and how it can be linked with other typesof surveillance systems.Part 2 – Operational Framework (chapters 4 to 6) lays out the information needed by ERU deployingNational Societies to develop and maintain their PH ERU CBS, including human resources needed,training, equipment and financial resources.Part 3 – Operational Management (chapter 7), is intended for deploying National Societies as well asHandbook PHE ERU CBS – revised November 2019Page 7 / 55
delegates, as it details the deployment phases, and explains key issues and procedures.Background – development of Public Health ERUsThe International Federation of Red Cross and Red Crescent (IFRC) and partners have long acknowledged the impact of disasters on the health of populations and the importance of disease outbreaksat local, regional and global levels.The Movement has not only vast experience in emergency response but also in preparedness, recoveryand development. The Movement is a major player among humanitarian organisations and has theworld’s largest network of volunteers and staff. Collectively, it has also the largest pool of trained andexperienced specialists1 ready to deploy within short notice. The IFRC has been coordinating the deployment of Health Emergency Response Units (ERUs) since 1996.During annual technical working group meetings, IFRC and ERU National Societies (NS) have observedthat clinical care alone in an emergency setting is not enough to mitigate health risks at the communitylevel, suggesting a need for Public Health-focused tools.Moreover, the Movement has been a major player both in some of the largest outbreak responsessuch as for example the Ebola outbreak in West Africa or the cholera outbreak in Somalia as well assmaller scale epidemics including the plague outbreak in Madagascar, cholera in Malawi or Ghana andmany others. In 2017, the Council of Delegates of the International Red Cross and Red Crescent Movement, the IFRC and NS committed to strengthen effective community engagement in disease outbreakprevention and response.The Red Cross and Red Crescent Movement2 believes that epidemic preparedness and response startsand ends with communities, and that without community-driven efforts to prevent, detect and respond to infectious disease threats, government efforts can be delayed and potentially less effective3.In this context, a review of lessons learnt has led to the recommendations for improved IFRC PublicHealth response capacity. To ensure the IFRC remains ‘fit for purpose’ and can meet the demands ofglobal trends and requests for support from National Societies standalone, multi sectoral Public Health(PH) ERU configurations have been proposed.IFRC in collaboration with ERU NS have outlined seven spheres of activity that are needed in order tobetter respond to public health emergencies, that have been submitted to the Global Surge Working1The pool consists of specialists from diverse domains needed in order to respond to emergencies, includinghealth, WASH, logistics, finance/admin, IT, communication and others.2Further in the text, the Red Cross and Red Crescent Movement will be referred to as the Movement3IFRC, Council of Delegates of the International Red Cross and Red Crescent Movement; Working towards anInternational Red Cross and Red Crescent Movement Approach to Epidemics and Pandemics, Resolution, 2017Handbook PHE ERU CBS – revised November 2019Page 8 / 55
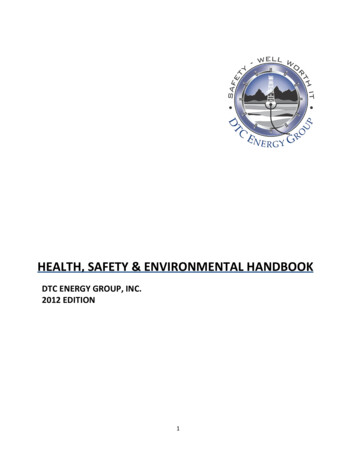
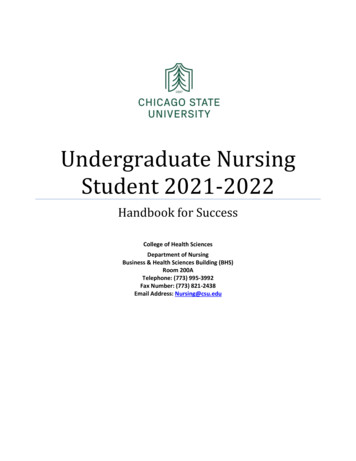
Group, the Human Resources Group for International Deployment of Delegates and the Disaster Management Working Group4.Six standalone, multi-sectoral PH ERU configurations and one clinical care support team for outbreakshave been prioritised for development and deployment:1. Community Case Management – Cholera or Nutrition2. Community Based Vector Control3. Community Based Surveillance4. Safe and Dignified Burials5. Social Behaviour Change Communication (SBCC)/Health Promotion6. Infection and Prevention Control7. VaccinationIFRC have invited National Societies with the capacity, or the willingness to develop capacity in one ormore of the PH ERU configurations. A list with all ERU configuration and leading as well as supportingNS can be found in Annex 1.This handbook focuses on Configuration 3 of the PH ERU’s: Community Based Surveillance. It reflectsstandard operating procedures that are particular for the PH ERU CBS configuration and complementsthe general IFRC ERU standard operating procedures (IFRC, ERU Standard Operating Procedures, 2012)as well as the IFRC handbook for delegates (IFRC, Handbook for delegates, 2002).Articulation between PH and clinical ERUsWithin the health domain, ERU NS have Red Cross hospitals and Red Cross clinics ready to deploy, andpublic health/community health delegates have supported prevention efforts in the communities. Thenew PH ERU CBS configuration will not replace but complement these elements. Neither do they replace capacity building of NS or contingency planning.Figure 1 shows articulation between clinical and PH ERU’s from the perspective of the PH ERU CBS.The PH ERU CBS will have close linkages to other response activities. For example, it can link detectedcases for referral to a clinical ERU. It can be deployed together with a community-case managementof cholera PH ERU (CCM ERU), to allow for effective data collection at oral rehydration points.4IFRC, Briefing note on Improving Response to Public Health in Emergencies, 2016Handbook PHE ERU CBS – revised November 2019Page 9 / 55
Figure 1: Complementarity of ERUs and link to pre and post disaster activitiesPre and postdisaster activitiesSurge capacityWASH ERU’sSafe and DignifiedBurials PH ERUDevelopment activities atNational Society andCommunity levelCommunity BasedVector Control PH ERUPrevention activities at atcommunity level (CBHFA,ECV, HP/WASH, RCCE, CBS,etc)Preparedness activities atNational Society andcommunity level (Health,WASH, Nutrition, DRM,etc)Handbook PHE ERU CBS – revised November 2019Community BasedSurveillance (CBS) PH ERUField Hospital ERUSBCC/HealthPromotion PH ERUCommunity CaseManagement Cholera PHERUClinical CaseManagement Cholera(CTC)Page 10 / 55
BOX 2. CBS and ORPs – a special relationshipCBS was first tested in the context of an ORP (Oral Rehydration Point) during a Cholera outbreak. Since then, the advantages of linking CBS and ORP have become evident. CBS in anORP is one of the most common uses of CBS that delegates may encounter. It is thus worthto give it some special consideration. ORPs are now being integrated into PH ERU CCM Cholera.CBS can be used in an ORP to provide valuable, real-time information on Acute Watery Diarrhea (AWD) cases seen in the community. Since only 10 to 20% of cholera/AWD cases will bereferred and seen in a health facility, this information from ORPs is crucial to estimate thereal size of the outbreak. It is also useful in programmatic terms, helping to make evidencebased decisions on where to shut down ORPs and where to reposition them, as the outbreakincreases, decreases or shifts geographically.When CBS is used in ORPs, a number of variables will change. First, reports will be linked toan ORP site, and not to an individual volunteer, as several volunteers may be working in asame ORP.Second, more data may need to be collected, either through regular SMS to the digital CBStoolkit (see next chapters) or through other means (paper-based, phone calls, apps). This information includes number of people referred to a health facility (i.e. number of people withsevere dehydration, disaggregated by age group and gender), and potentially number of ORSand/or water tablets distributed, among others.Third, the response activities for CBS are very well defined in the ORPs (distribution of cleanwater, water purifying tablets, ORS, etc), and go beyond the prevention and health promotion messages that may be the only response provided by the volunteers in other outbreaks.Fourth, when ORPs are deployed with CBS, it will be in an active outbreak setting, as opposedto the preventive deployment of a PH CBS ERU in cases where an epidemic outbreak isfeared but not yet present. Thus, an “active” reporting system is needed. This means that thenumber of reports from the system will be high and daily/regular reporting is required. It alsomeans that “zero reporting” is needed, with all ORPs reporting daily, even if they have notseen any individuals with AWD that day.Finally, good communication with any Clinical ERUs (Cholera Treatment Centers or Units)present, is also needed, ensuring follow up of referred cases, and avoiding “double counting”(of cases seen in community and in facility).Handbook PHE ERU CBS – revised November 2019Page 11 / 55
2. Framework for Public Health ERU’sStrategic and institutional frameworkIFRC’s Strategy 2020 “Saving Lives, Changing Minds” renews the commitment to humanitarian aid andcalls for more action to prevent and reduce the underlying causes of vulnerability.5 The PH ERU CBSconfiguration unites Strategic aim One (save lives, protect livelihoods and strengthen recovery fromdisasters and crises) with Strategic aim Two (enable healthy and safe living).The Movement bases its activities on the seven Fundamental Principles: humanity, impartiality, neutrality, independence, voluntary service, unity and universality.The IFRC adheres to the following standards:-The Code of Conduct for the International Red Cross and Red Crescent Movement and NonGovernmental Organisations in Disaster Relief6-The Humanitarian Charter and Minimum Standards in Disaster Response (The Sphere Project,2018)Moreover, the Public Health ERUs also ensure that deployments adhere to-.-ERU Standard Operating Procedures7-Data protection principles8-Surge Guidelines and Standard Operating Procedures9-Implementation Guidelines for Epidemic Response (IGER)Guiding principlesThe PH ERU CBS configuration follows guiding principles that are aligned with the IFRC Strategy 2020.Access to health for all: The Movement strives to achieve that all community members have equalaccess to the PH ERU CBS, paying attention that also the most vulnerable and disadvantaged peoplesuch as women, children, the elderly and those living with disability have access.Cooperate in partnership, promote alliances and participate in networks: The PH ERU CBS will workunder the umbrella of the IFRC operation manager and in close collaboration with the local NS, other5IFRC. (2010). Strategy 2020; Saving lives changing minds. Geneva: IFRC.IFRC/ICRC. (1994). Code of Conduct for the International Red Cross and Red Crescent Movement and NonGovernmental Organisations in Disaster Relief.7IFRC. (2012). ERU Standard Operating Procedures. Geneva8IFRC. Data Protection Policy. Draft 2019 – unpublished.9IFRC. Emergency Surge personnel deployments. Deployment Guidelines and Standard Operating Procedures.Final Draft 2019 – unpublished.6Handbook PHE ERU CBS – revised November 2019Page 12 / 55
deployed ERUs and the Ministry of Health. Interventions follow the national health policies or WHOguidelines. The PH ERU CBS also works with other international partners where appropriate.Do no harm and take conflict-sensitive action: The PH ERU CBS always considers the unintended negative effects of its work (do no harm). Conflict-sensitive project management is therefore a fundamental component of the project management in all areas. Barriers and enablers are carefully assessed inthe community and services are provided equally for all segments of the population. Together withstakeholders, intervention areas are carefully selected to ensure the best possible service coveragewith equal access for all.Gender and diversity: The minimum standard commitments on gender and diversity will follow thefour specific areas dignity, access, participation and safety as described in the IFRC minimum standardcommitments to gender and diversity in emergency programming guidelines10Minimum core standardsAll the PH ERU NS are expected to confirm that they are able and willing to adhere to IFRC ERU SOP11and to the defined minimum standards for each PH ERU.Table 1 shows the minimum core standards are criteria to which the PH ERU CBS team must adhere.They describe structure and performance during deployment, but they should be acknowledged andimplemented prior to deployment. This allows the affected country to have confidence in the capabilities of the PH ERU CBS and an opportunity to hold PH ERU CBS accountable if they do not meet theirstated capability.Table 1. Minimum core standardsStandard 1Adhere and follow IFRC ERU SOPStandard 2Collaborate and coordinate with inter-agency response coordination mechanism at global, regional and national level, as well with other response team and health system if appropriateStandard 3Ensure regular reporting to designated stakeholders during the response in accordance to IFRCdeployment orderStandard 4Ensure data protection rules and regulation followed appropriatelyStandard 5A. Adhere to professional guidelines – all delegates have the appropriate knowledge,skills and relevant formal education to practice the work they are assigned to.B. Adhere to IFRC Humanitarian Health Competency Framework in selection, training andevaluation of delegatesC. Ensure that delegates deployed within the PH ERU CBS are appropriately trained in accordance to agreed training requirementsEnsure that all equipment deployed complies with international quality standardsStandard 61011IFRC. (2015). Minimum standard commitments to gender and diversity in emergency programming. Geneva.IFRC. (2012). ERU Standard Operating Procedures. Geneva.Handbook PHE ERU CBS – revised November 2019Page 13 / 55
Standard 7Ensure that the PH ERU CBS have arrangements in place for care of the team members healthand safety including repatriation and exist strategies if requiredStandard 8Ensure that the PH ERU CBS is self-sufficient and do not put demand on logistic support fromthe affected National Society, unless agreed otherwise before deploymentEnsure integration of crosscutting approaches are included in the response such as CEA, gender,diversity and protection.Standard 9Standard 10Ensure system for compliance mechanism and plans for evaluation are in place during responseand undertake evaluation of deployment to ensure learning and enhance good practice3. The PH ERU CBS configurationWhat is CBS?Outbreaks normally begin with a cluster of sick people, or sudden deaths in a community, that is notdetected in a timely manner by traditional surveillance systems12. This may be aggravated in scenarioswhere traditional surveillance systems have weaknesses or there is inadequate coverage of communities by health facilities. This allows them to start an immediate response, while waiting for supportfrom the NS.Meanwhile, trained staff and delegates can monitor in the real-time the notifications being sent in byvolunteers and carry out an appropriate
Handbook PHE ERU CBS – revised November 2019 Page 1 / 55 Handbook Public Health ERU Community Based Surveillance (CBS) Group lead: Norwegian Red Cross (focal point: PHiE Coordinator, Tonje Tingberg) Group members: Hong Kong Red Cross Society (Focal point, Karen Poon), French