Transcription
PART IVACUTE COMMUNICABLE DISEASES
LIST OF REPORTABLE DISEASE COVERED IN B-73 cellosisCampylobacteriosisChagas DiseaseChickenpox (outbreaks, fatal andhospitalized sticercosis (Taeniasis)DengueDiphtheriaE. Coli 0157:H7 Infection and HUSEhrlichiosisEncephalitis, Acute ViralEncephalitis, Arthropod-borne (arboviral)Foodborne DiseaseGastroenteritis, Viral (outbreaks)GiardiasisHaemophilus influenzae, Invasive DiseaseHantaviral Pulmonary SyndromeHepatitis, Type A (HAV, infectious hepatitis)Hepatitis, Type B (HBV)Hepatitis, Type B, PerinatalHepatitis CInfluenzaLegionellosisLeprosy (Hansen’s Disease)LeptospirosisListeriosisLyme BorreliosisMalariaMeasles (Rubeola)Meningitis, Viral (outbreaks)Meningococcal InfectionsMumps (outbreaks)Paratyphoid FeverPediculosis (outbreaks)Pertussis (Whooping cough)PlaguePneumococcal, Invasive DiseasePoliovirus InfectionPsittacosisQ Fever (Query fever)Los Angeles County Department of Public HealthAcute Communicable Disease Control, B-73 (rev. 11/2011) Rabies, Human and AnimalRelapsing Fever (louseborne, tickborne)Respiratory Disease (outbreaks)Ringworm of Scalp (outbreaks)Rocky Mountain Spotted FeverRubella, Acute or Postnatal (Germanmeasles, 3-day measles)Rubella, CongenitalSalmonellosisScabies (outbreaks)Severe Acute Respiratory Syndrome (SARS)Shigellosis (Dysentery, Bacillary dysentery)SmallpoxStaphylococcal InfectionsStaphylococcal Toxic Shock SyndromeStreptococcal Infections, Group AStreptococcal Toxic Shock Syndrome (STSS)TetanusToxic Shock SyndromeTrichinosis (Trichiniasis, Trichinellosis)TularemiaTyphoid Fever, AcuteTyphoid Fever, CarrierTyphus, Flea-borne (Murine typhus,endemictyphis)Vibriosis, Non-cholera SpeciesWest Nile VirusYellow FeverYersiniosis
PUBLIC HEALTH NURSING HOME VISITPROTOCOLBased on the Los Angeles County Public Health Nursing PracticeManual, the guidelines for home visit by district public health nursing for acutecommunicable diseases establish a standardized method of follow-up.The PHN will adhere to the following guidelines outlined in the three documents:o Public Health Nursing Home Visit Protocol for ACD and STDo Public Health Nursing Home Visit Required Algorithmo Public Health Nursing Home Visit As Necessary (HVAN) AlgorithmThe list of acute communicable disease on Public Health Nursing Home Visit Protocolfor ACD and STD is to clarify State legal mandates per California Code of Regulations.All other diseases listed in B-73 are considered HVAN unless directed byAMD/Supervision.
Public Health Nursing Home Visit Protocol for ACD and STDState legal mandate(CA Code of Regulations)Amebiasis – HVANSalmonellosis – HVANShigellosis – HVANTyphoid Fever, Acute – RParatyphoid – RTyphoid, Chronic- RENTERICSPer B-73 GuidelinesACDNon-regulated EntericsCryptosporidiosis – HVANGiardiasis – HVANshiga toxin producing E Coli – HVANVibriosis – HVANYersiniosis – HVANDiseases that may requireTREATMENT orPROPHYLAXISfor cases or contactsPer B-73 GuidelinesDiphtheria – RHepatitis A – HVANHaemophilus influenzae ( 15 yrs of age) – RMeasles – RMeningococcal Infections – RPertussis – RRabies (Post Exposure Prophylaxis) – HVANOutbreaks (HC or non-HC settings) – R (unless waived by AMD)Non-Standard District request as per CHS Policy #206 - HVANOTHERChild under 12 years with syphilis, gonorrhea, chlamydia, or pelvic inflammatory disease (PID)(suspected child sexual abuse) – RNewborn with gonorrhea / chlamydia conjunctivitis – RSTD(‡) Pregnant/postpartum women with syphilis – R(‡) Pregnant/postpartum women with chlamydia or gonorrhea – HVAN(‡) Pregnant women with PID or HIV – HVANInfants whose mothers were diagnosed with chlamydia or gonorrhea at delivery – RMothers whose infants were diagnosed with chlamydia or gonorrhea – RInfants with suspected congenital syphilis in need of evaluation and treatment – RInterview record for investigation/referral of partners of pregnant women with syphilis – RInterview record for investigation/referral of partners of pregnant women with gonorrhea/ chlamydia or HIV- HVANLegend:HVAN: HOME VISIT AS NECESSARY - A face to face interview is conducted as necessary.R: REQUIRED - A face to face interview is required.(‡): Treatment must be verified with the Medical Provider.New 03/10
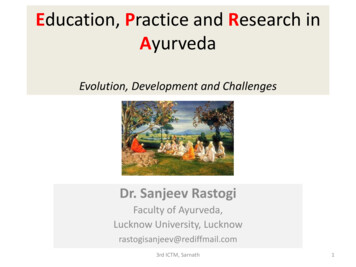
Public Health Nursing Home Visit REQUIRED AlgorithmNot reachableVerify contact info.New info found?NOYESCD/STD Caseassigned to PHNCall ClientRequiredHOME or SITE VISIT(SEE NOTE #1)Contact MadeAppt. EstablishedDoneInvestigation /follow-upcompletedSTDACDUnable to completeClient NFNew contactinfo foundClient NHorYESUTL client(Not found – initiatePostal address verification)PHNSNOACDConduct 2ndhome visit w/in 24 (including weekends)(SEE NOTE #1)Client found?CASE CLOSEDto DistrictAMDfordispoSTDAMD for disposition &PHNS for informationLegend (and examples):UTL – Unable To Locate client at known address oraddress is not a residence.NH – Not Home (address correct, client not home)NF – Not Found (e.g., person residing at reportedaddress denies client is living there)UTLNOSPHI fordispoSPHIPHInew contactinfo?YESNONOTE #1:Required face to face or site visit UNLESSapproved by PHNS and/or AMDNew 03/10CASECLOSEDto DistrictYESSPHI AMD& notify PHNSClient locatedInfo to PHNS forreturn to PHNRequiredHOME or SITE VISIT(SEE NOTE #1)PHNS review fordispoCASE CLOSEDto DistrictPHNS reviewAMD or designeefor dispo
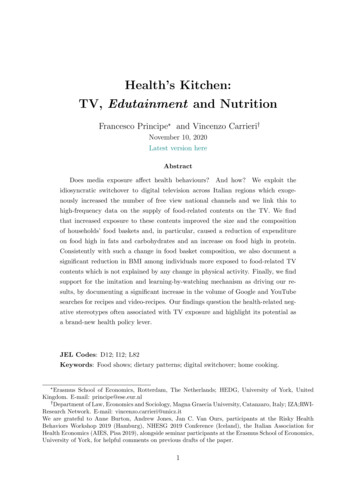
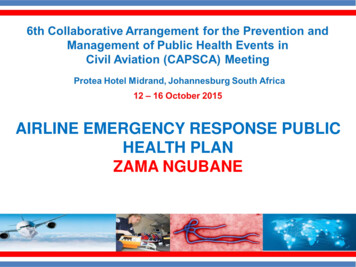
Public Health Nursing Home Visit AS NECESSARY (HVAN) AlgorithmYESCD/STD Caseassigned to PHNCall ClientContact MadeYESNONot reachable/No responseVerify contact infow/ referral sourceNONo newcontact infoPHNS for reviewACDAMD or designeefor dispositionCASECLOSEDto DistrictNew 03/10STDSPHI fordisposition(via Casewatch)Home Visit orderedSee Home VisitREQUIRED algorithmYESContactmade viarevised infoServicesprovided asneeded(e.g. refer toHC)STD cases:Submit to PHNS for review& dispo (via Casewatch)ACD cases:Submit to PHNS review àAMD or designee for dispoInvestigationcompleted byphoneNOPHNS or AMD / designeedetermine ifHome Visit iswarranted?CASE CLOSEDto DistrictNOYESHome Visit orderedSee Home VisitREQUIRED algorithm
Acute Communicable Disease Control Manual (B-73)REVISION—AUGUST 2011AMEBIASIS1. Agent: Entamoeba histolytica, a protozoanparasite that exists as a trophozoite and cyst.A related non-pathogenic strain is distinctepidemiologically and biologically from thepathogenic species; this has been renamedEntamoeba dispar. E. dispar is notpathogenic in humans.E. histolytica is not to be confused with nonpathogenic protozoa found commonly inhumans, which require no treatment. Theseinclude E. dispar, E. hartmanni, E. coli, E.polecki, Iodamoeba butschlii, Endolimaxnana, Chilomastix mesnili, Trichomonashominis, Retortamonas species, Enteromonas species, and usually, Blastocystishominis.2. Identification:b. Differential Diagnosis: Other l illness. Amebic liverabscess should be differentiated frompyogenic abscess.3. Incubation period: Variable, a few days tomonths; commonly 2-4 weeks.4. Reservoir: Humans.5. Source: Cysts from feces of infected case.6. Transmission: Direct fecal-oraltransmission, sexual transmission, ingestionof fecally contaminated food or water, colonicirrigation.7. Communicability: Variable, as long a carrierstate persists.a. Symptoms: Depend on site.Intestinal: There are four distinct intestinalclinical syndromes with E. histolytica.Asymptomatic colonization (cyst passage), acute amebic colitis, fulminantcolitis, and ameboma. Asymptomatic cystpassageusuallyresolveswithouttreatment; many such cases actually mayhave E. dispar. Patients with acuteamebic colitis present with lower abdominal pain and have had frequentbloody stools over a period of severalweeks; only about 1/3 have fever.Fulminant colitis is an uncommon presentation, most commonly seen in children.There is diffuse abdominal pain, profusebloody diarrhea, and fever; concurrentliver abscess is common, and 3/4 maydevelop colonic perforations. Ameboma isa rare (1%) manifestation that may bewithout symptoms, or present as a tendermass accompanied by symptomaticdysentery.8. Specific Treatment: Consult the MedicalLetter or Pediatric Red Book for specificdrugs and dosages. Only E. ies do not perform the test todistinguish it from E. dispar, treatment iscommonly given to all persons with cysts ortrophozoites of E. histolytica /dispar complex.9. Immunity: None.REPORTING PROCEDURES1. Reportable: (Title 17, Section 2500,California Code of Regulations.) Reportwithin 1 working day of identification of acase or suspected case.2. Report Form:PARASITE EPIDEMIOLOGIC CASEHISTORY FORM (acd-parasite)3. Epidemiologic Data:Extra-intestinal: Amebic liver abscess,with either an acute clinical course withsymptoms of 10 days, or a subacutecourse with symptoms lasting up to 6months. Other sites of involvementinclude pleura, peritoneum, pericardium,and brain.a. Indicate whether case is: Acute (i.e., diarrhea within the past 6weeks), chronically symptomatic, orasymptomatic carrier. Intestinal or extra-intestinal (e.g., liver,lung abscess or other).PART IV: Acute Communicable DiseasesAMEBIASIS — page 1
Acute Communicable Disease Control Manual (B-73)REVISION—AUGUST 2011b. Sexual orientation.c. History of colonic irrigation, when andwhere.2. Non-sensitive Occupation or Situation:Release after clinical recovery unlesshousehold contacts are food employees.CONTACTS:d. Immigration from or travel to a developingcountry within 6 months prior to onset.Specific dates and places.Household members or persons who share acommon source.e. Exposure to carrier and other personswith diarrheal illness within incubationperiod.1. Sensitive Occupation or Situation:f. Occupation of case and household members.b. Asymptomatic: Clearance notrecommended.a. Symptomatic: Treat as a case.g. Residence in facility for thedevelopmentally disabled.2. Non-Sensitive Occupation or Situation:Clearance not recommended.h. Attendance in day care.CARRIERS:CONTROL OF CASE, CONTACTS &CARRIERSRefer for treatment. Release as for case.PREVENTION-EDUCATIONContact within 24 hours to determine if sensitiveoccupation or situation (SOS) involved.Otherwise, investigate within 3 days.1. Stress hand washing and personal hygiene.2. Advise about increased risk with anal andoral-anal sex.Public Health Nursing Home Visit Protocol:Home visit as necessary – a face to faceinterview is conducted as necessary.Refer to “Public Health Nursing Home Visit ASNECESSARY (HVAN) Algorithm” (B-73 Part IVPublic Health Nursing Home Visit Protocol).3. Dispose of feces in a safe, sanitary fashion.4. Take precautions with food and water whentraveling to endemic areas.5. Advise regarding risk associated with colonicirrigation.CASE:6. Protectwatercontamination.Precautions: Enteric precautions until clinicalrecovery.DIAGNOSTIC PROCEDURES1. Sensitive Occupation or Situation: Appliesonly to food employees, not other SOS.Remove food employees from work until 3consecutive feces specimens taken 3 ormore days apart are negative by O&P. Firstspecimen may be taken after patient is onmedication for 5 days. Alternatively, if the E.histolytica EIA test is negative, the patientdoes not have amebiasis and is no longer acase. See Diagnostic Procedures below.supplyfromfecal1. Microscopic:Container: Feces-ParasiteLaboratory Form: Test Requisition FormH-3021 (Rev. 9/07)Examination Requested: Ova & Parasites(O&P) for Amebiasis. Check appropriateboxes on laboratory form.Material: Feces. Follow instructions providedwith container.PART IV: Acute Communicable DiseasesAMEBIASIS — page 2
Acute Communicable Disease Control Manual (B-73)REVISION—AUGUST 2011Amount: Walnut size.Storage: Do not refrigerate; protect fromoverheating.Remarks: Mix thoroughly with PVApreservative. Do not collect specimen(s) for7-10 days after barium, mineral oil, bismuth,antibiotics, anti-malarials or antidiarrhealpreparations such as kaolin have beeningested. Specimen must be unpreservedand examined within 24 hours of passage.Note: This test does not distinguish betweenE. histolytica and nonpathogenic E. dispar. Afrozen, unpreserved stool sample can besubmitted for E. histolytica EIA test todistinguish between the two. Please refer toLA County Public Health Laboratory testcatalog for more information.2. Serology: (used for extra-intestinal diseaseonly) To California State Department ofHealth.Container: Sterile tube.Examination Requested: Amebiasisantibody.Material: Serum.Amount: 2 ml.Storage: Refrigerate.Remarks: Consult with Public HealthLaboratory for more information aboutserology testing. Diagnostic titer: 1:128 byIHA test. Allow 2 to 4 weeks for results.PART IV: Acute Communicable DiseasesAMEBIASIS — page 3
Acute Communicable Disease Control Manual (B-73)REVISION—FEBRUARY 2013ANAPLASMOSIS(formerly termed ehrlichiosis; human granulocytic ehrlichiosis [HGE])1. Agent: Anaplamosis is caused by Anaplasmaphagocytophila, an ehrlichial organismformerly known as Ehrlichia phagocytophila, E.equi.2. Identification:a. Symptoms:Humanehrlichiosis/anaplamosis are newly recognizeddiseases in USA. The spectrum of diseaseranges from mild illness to a severe, lifethreatening or fatal disease. Symptoms areusually nonspecific; the most commoncomplaints are fever, headache, anorexia,nausea, myalgia and vomiting. The diseasemay be confused clinically with RockyMountain spotted fever (RMSF) but differsby rarity of a prominent rash.Laboratory findings include leukopenia,thrombocytopenia, and elevation of one ormore liver-function tests. In hospitalizedcases, the laboratory findings may be onlyslightly abnormal on admission, andbecomemoreabnormalduringhospitalization.b. Differential Diagnosis: RMSF, bacterialsepsis, Lyme disease, endemic (murine)typhus, toxic-shock syndrome, gastroenteritis, viral syndromes, tick-borneencephalitis and other multi-system febrileillnesses.c. Diagnosis: Preliminary diagnosis ofehrlichiosis/anaplamosis in the USA isbased on clinical and laboratory findings.Confirmation is based on: the evaluation ofa blood smear, development of serumantibodies to E. chaffeensis for ehrlichiosisor A. phagocytophila for anaplamosis;immunofluorescence test; PCR.3. Incubation: 7 to 21 days forehrlichiosis/anaplamosis.4. Reservoir: White-tailed deer are a major hostof lone star ticks and appear to represent onenatural reservoir for E. chaffeensis. Deer, elk,and wild rodents are likely reservoirs of theagent of HGE.5. Source: Ehrlichiosis/anaplamosis in NorthAmerica has been concentrated in thesoutheastern and south-central areas of theUSA. More than 12 human cases, including 3deaths, caused by a granulocytic Ehrlichia,have occurred in northern Minnesota,Wisconsin, Connecticut, Maryland and Florida.Rarely cases of ehrlichiosis/anaplamosis havebeen diagnosed in California.6. Transmission: In the United States, ehrlichiaeare transmitted by the bite of an infected tick.The lone star tick (Amblyomma americanum),the blacklegged tick (Ixodes scapularis), andthe western blacklegged tick (Ixodes pacificus)are known vectors of ehrlichiosis/anaplamosisin the US. Ixodes ricinus is the primary vectorin Europe. Most patients report a tick bite orassociation with wooded, tick-infested areas1prior to onset of illness.7. Communicability: No evidence of person-toperson transmission.8. Specific Treatment: A tetracycline such asdoxycycline; chloramphenicol for pregnantwomen and children under 8 years of age.9. Immunity: Susceptibility is believed to begeneral. No data are available on protectiveimmunity in humans from infections caused bythese organisms. Re-infection is rare but hasbeen reported.REPORTING PROCEDURES1. Reportable within 7 days of diagnosis (Title 17,Section 2500, California Code of Regulations).2. Report Form:EHRLICHIOSIS/ANAPLASMOSIS CASEREPORT (CDPH 8573)3. Epidemiologic Data:a. Recent travel to endemic areas.1 See http://www.cdc.gov/anaplasmosis/.PART IV: Acute Communicable DiseasesANAPLASMOSIS — page 1
Acute Communicable Disease Control Manual (B-73)REVISION—FEBRUARY 2013b. History of tick bites.c. History of possible exposure to ticks inwooded areas.d. Occupational exposure.CONTROL OF CASE & CONTACTS:CASE:1. Isolation: None.2. Concurrent disinfection: Remove any ticks.CONTACTS: No restrictions.PREVENTION-EDUCATION1. Use of tick repellants in endemic areas.2. Wear protective clothing in wooded areas.3. Control ticks on domestic animals.4. Avoid tick-infested areas when possible.Check skin periodically and remove attachedticks immediately.DIAGNOSTIC PROCEDURES1. Serology: Indirect immunofluorescence.Container: Serum separator tube.Laboratory Form: State special serology.Examination Requested:Ehrlichiosis/anaplamosis.Material: Whole blood.Amount: 10 ml.Storage: Refrigerate until transported.2. PCRContainer: Red top or red-grey top tube.Material: Serum.Amount: 1 ml.Storage: Refrigerate or freeze untiltransported.PART IV: Acute Communicable DiseasesANAPLASMOSIS — page 2
Acute Communicable Disease Control Manual (B-73)REVISION—OCTOBER 2011ANISAKIASIS1. Agent: Larval nematodes of the subfamilyAnisa-kinae, genera Anisakis, andPseudoterranova.2. Identification: A parasitic disease of thehuman gastrointestinal tract usually manifestedby cramping, abdominal pain and vomiting,resulting from the ingestion of uncooked orunder treated marine fish containing larvalnematodes. The motile larvae burrow into thestomach wall producing acute ulceration withnausea, vomiting and epigastric pain,sometimes with hematemesis. They maymigrate upward and attach in the oropharynx,causing cough. In the small intestine, theycause eosinophilic abscesses, and thesymptoms may mimic appendicitis or regionalenteritis. At times they perforate into theperitoneal cavity; they rarely involve the largebowel. Diagnosis is made by recognition of the2 cmlong larva invading the oropharynx or byvisualizing the larva by gastroscopicexamination or in surgically removed tissue.3. Incubation period: Gastric symptoms maydevelop within a few hours after ingestion.Symptoms referable to the small and largebowel occur within a few days or weeks,depending on the size and location of larvae.4. Reservoir: Anisakinae are widely distributed innature, but only certain of those that areparasitic in sea mammals constitute a majorthreat to humans. The natural life cycleinvolves transmission of larvae by predationthrough small crustaceans to squid, octopus orfish, then to sea mammals, with humans asincidental hosts.5. Source: The disease occurs in individuals whoeat uncooked and inadequately treated(frozen, salted, marinated, smoked) saltwaterfish, squid or octopus. This is common inJapan (sushi and sashimi), the Netherlands(herring), Scandinavia (gravlax) and LatinAmerica (ceviche).6. Transmission: The infective larvae live in theabdominal mesenteries of fish; often afterdeath of their host they invade the bodymuscles of the fish. When ingested by peopleand liberated by digestion in the stomach, theymay penetrate the gastric or intestinal mucosa.7. Communicability: Direct transmission fromperson to person does not occur.8. Specific Treatment: Gastroscopic removal oflarvae; excision of lesions.9. Immunity: None.REPORTING PROCEDURES1. Reportable: (Title 17, Section 2500, CaliforniaCode of Regulations). Report within 1 workingday of identification of a case or suspectedcase.2. Report Form: OUTBREAK / UNUSUALDISEASE REPORT (CDPH 8554) Ifanisakiasis infection is associated with afoodborne illness, see also foodborne illnessreporting. If a prepared commercial food itemis the LIKELY source of this infection, aFOODBORNE INCIDENT REPORT should befiled. For likelihood determination and filingprocedures, see Part 1, Section 7 - Reportingof a Case or Cluster of Cases Associated witha Commercial Food: Filing of FoodborneIncident Reports.3. Epidemiologic Data:a. History of food items eaten during thesuspect incubation period, and location,where food was consumed.b. Listing of all individuals with opportunity toconsume suspect food items, whether ill ornot. Obtain individual food histories.c. For ill individuals: symptoms, onset dateand hour, duration, medical treatment andlaboratory results.d. For suspected food(s): source, date andhour of purchase, when consumed, methodof preparation, availability of sample(s).PART IV: Acute Communicable DiseasesANISAKIASIS — page 1
Acute Communicable Disease Control Manual (B-73)REVISION—OCTOBER 2011CONTROL OF CASE, CONTACTS & CARRIERSCASE: No restrictions.CONTACTS: Examination of others possiblyexposed at the same time may be productive.PREVENTION-EDUCATION1. Avoid ingestion of inadequately cooked marinefish. Heating to 60 "C (140 "F) for 10 minutes,blast-freezing to -35 "C (-31 "F) or below for 15hours or freezing by regular means at -23 "C(10 "F) for at least 7 days kills the larvae.Irradiation effectively kills the parasite.2. Cleaning (evisceration) of fish as soon aspossible after they are caught reduces thenumber of larvae penetrating into the musclesfrom the mesenteries.DIAGNOSTIC PROCEDURESConsult Public Health Laboratory, ParasitologySection.PART IV: Acute Communicable DiseasesANISAKIASIS — page 2
Acute Communicable Disease Control Manual (B-73)REVISION—MARCH 2014ANTHRAX1. Agent: Bacillus anthracis, a Gram-positivespore-forming bacillus.2. Identification:a. Symptoms:Cutaneous anthrax: An initial vesicle atsite of inoculation develops into apainless black eschar. Progresses tosystemic anthrax in 10-20% of cases;systemic anthrax, if untreated, has afatality rate up to 20%. Fatalities forcutaneous anthrax are 1% if effectiveantibiotics are given.Inhalational anthrax: Initially fever,chills, sweats, malaise, mild cough,dyspnea, nausea, or vomiting followed 35 days later by acute onset of respiratorydistress, shock; radiologic evidence ofmediastinal widening and pleural effusion.Fatality rate is extremely high.Anthraxmeningitis:hypotension,delirium or coma follow quickly; refractoryseizures, cranial nerve palsies, andmyoclonus have been reported. Candevelop hemorrhagic meningitis withcerebrospinal fluid analysis showingelevated protein, low glucose, and apositive Gram stain and culture. Seventyfive percent of patients died within 24hours of presentation.Gastrointestinal (GI) anthrax: Acutevomiting, abdominal distention, GIbleeding, peritonitis; fatality rate high.b. DifferentialDiagnosis:Cutaneousanthrax- includes spider bite, Orf,ulceroglandular tularemia, scrub typhus,ecthymagangrenosum,cutaneousleshmaniasis rickettsialpox. Inhalationalanthrax- includes pnuemonic plague,tularemia,communityacquiredpneumonia, viral pneumonias, Q fever.c. Diagnosis: Demonstration of B. anthracisby smear, animal inoculation or culture orPCR from blood, CSF, pleural fluid,ascitic fluid, vesicular fluid, or lesionexudate. Serologic test for B. anthracistoxin. Histopathology from fresh or frozentissue.3. Incubation: Within 7 days, usually 2 to 5.4. Reservoir: Soil; infected animals (cattle,sheep, goats, horses, pigs, etc.).5. Source: Spores from soil or contaminatedanimal products (hides, hair, meat, bones).6. Transmission: Inoculation,spores, or ingestion ofcontaminated meat.inhalation ofundercooked,7. Communicability: Inhalational Anthrax: Noevidence of transmission from person toperson. Contaminated products and soilremain infective for years. CutaneousAnthrax: Transmission through non-intactskin contact with draining lesions possible,therefore use Contact Precautions if largeamountofuncontaineddrainage.Handwashing with soap and water preferableto use of waterless alcohol based antisepticssince alcohol does not have sporicidalactivity. Environmental: Aerosolizable sporecontaining powder or other substance: Untildecontamination of environment complete,wear respirator (N95 mask or PAPRs),protective clothing; decontaminate persons.8. Specific Treatment:Cutaneous anthrax: ciprofloxacin ciprofloxacin or doxycycline in combinationwith one or two other active drugs. Penicillinor amoxicillin may be used if strain issusceptible.9. Immunity: Uncertain.REPORTING PROCEDURES1. Report any case or suspect cases bytelephone immediately (Title 17, Section2500. California Code of Regulations).a. Call Morbidity Unit during working hours.PART IV: Acute Communicable DiseasesANTHRAX — page 1
Acute Communicable Disease Control Manual (B-73)REVISION—MARCH 2014b. Call ACDC; after working hours, contactAdministrative Officer of the Day (AOD)through County Operator.c. Any laboratory that receives a specimenfor anthrax testing is required to report tothe State Microbial Diseases Laboratoryimmediately (Title 17, Section 2505,California Code of Regulations).d. ACDC must notify the State Division ofCommunicable Disease Control (DCDC)immediately upon receiving notice of acase of suspected anthrax. ACDC willsupervise investigation and controlmeasures.2. Report Form: ANTHRAX (HUMAN) CASEREPORT (CDPH 8578)3. Epidemiologic Data:a. Specify type (cutaneous, inhalational, Notify ACDC immediately and open promptly forACDC review. ACDC will investigate to identifypotential association to bioterrorist activity. Ifdeemed to be unaffiliated with bioterrorism, theresponsibility for the control of cases, contactsand carriers will be returned to the district whereupon action should be initiated within 7 days.CASE:Precautions:1. Cutaneous: Wound and skin precautionsuntil lesions are completely healed.2. Inhalational: Standard precautions as inTitle 17, Section 2500, California Code ofRegulations. Section 2518 is recommendeduntil patient recovers.CONTACTS: No restrictions.b. Occupation: Farmer, dairyman,veterinarian, wool processor, weaver,butcher, slaughterhouse employee,tanner, taxidermist, hunter, or laboratoryworker. Also postal workers, politiciansand their staff, and members of newsmedia as in the 2001 anthrax letterattacks.CARRIER: Not applicable.c. Contact with animals or animal products.Determine if veterinary diagnosis wasmade.2. Educate workers in high-risk occupations.d. Ingestion of undercooked meat.e. Exposure to animal products (e.g., hair,skins, paint brushes, bongo drums,leather, and wool) imported from outsidethe USA, especially Haiti and Asia.f. Bioterrorism: B. anthracis has been listedby the CDC as one of the agents mostlikely to be used in a bioterrorist attackbecause of the devastating physical andpsychological effects of inhalationalanthrax and the ability to be weaponizedand effectively delivered to a target area.Please see State of CaliforniaBioterrorism Surveillance andEpidemiological Response Plan.&ANIMAL: Veterinary Public Healthinvestigate potential animal sources.willPREVENTION-EDUCATION1. Disinfect animal products prior to processing.3. Double-bag discharges from lesions andsoiled articles. Autoclave or burn allinfectious material.4. If anthrax is suspected, necropsy must notbe done on the animal.5. Infected animal carcasses should be burnedor deeply buried and covered with calciumoxide (CaO, quicklime).6. Maintain properindustries.ventilationinhigh-risk7. Ensure proper disposal of wastes fromrendering plants and factories that processpotentially contaminated animal products.8. A vaccine is available for veterinary andother high-risk occupations.PART IV: Acute Communicable DiseasesANTHRAX — page 2
Acute Communicable Disease Control Manual (B-73)REVISION—MARCH 20149. Any possible bioterrorist exposures shouldbe reported immediately to local lawenforcement and public health for evaluation.DIAGNOSTIC PROCEDURESSpecimens: Blood, CSF, pleural fluid, asciticfluid, vesicular fluid, lesion exudates or othermaterials for direct examination or culture.Consult the Public Health Laboratory.PART IV: Acute Communicable DiseasesANTHRAX — page 3
Acute Communicable Disease Control Manual (B-73)REVISION—MARCH 2014BOTULISM(See also INFANT BOTULISM and WOUNDBOTULISM, below.)1. Agent: Toxin produced by Clostridiumbotulinum (and rarely other clostridiumspecies), a gram-positive bacillus. Mostcases due to type A, B or E toxin. Heat-labiletoxin is produced under anaerobic nsically in the gastrointestinal tract(intestinal botulism, infant botulism) or wound(wound botulism).2. Identification:a. Symptoms: An intoxication characterizedby weakness, extreme dryness of themouth, headache and constipation(although vomiting and diarrhea mayoccur), followed by symmetrical cranialnerve motor paralysis, ptosis, visualdifficulty, and descending paralysis.Severity appears dose related.Death may occur from respiratory failureor superimposed infections.b. Differential Diagnosis: Guillain-Barrésyndrome (Miller-Fisher variant),myasthenia gravis, cerebrovascularaccident, tick paralysis, neoplasia, orchemical intoxication.c. Diagnosis: Demonstration of toxin infeces or serum of the patient or in a suspected food item. Isolation of theorganism from feces, wound, orsuspected food is indicative of source.3. Incubation period: Usually within 12-36hours of eating contaminated food, but mayoccur several days afterward. Woundbotulism occurs within days of injury.4. Reservoir: C. botulinum spores in soil,water, and the intestinal tracts of animals,including fish.5. Source: Toxins are produced by C.botulinum and rarely other clostridiumspecies under anaerobic conditions, usuallyby improperly home-canned foods, especiallylow acid food, corn, beans; baked potato ormishandled foods that should have beenrefrigerated. Also in contaminated, closedwounds, similar to tetanus (C. tetani).6. Transmission: Ingestion of toxin orproduction of toxin in infected wound or GItract.7. Communicability:person to person.Notcommunicable8. Specific Treatment: Heptavalent (A-B-C-DE-F-G) equine-based botulinum antitoxin(HBAT). ACDC or CA Dept. of Public Health(
PUBLIC HEALTH NURSING HOME VISIT PROTOCOL Based on the Los Angeles County Public Health Nursing Practice Manual, the guidelines for home visit by district public health nursing for acute communicable diseases establish a standardized method of follow-up. The PHN will adhere to