Transcription
Volume 44 Number 18August 31, 2021Imaging of Fetal Head and Neck Masses: A Systematicand Anatomic ApproachJennifer A. Vaughn, MD, Luis F. Goncalves, MD, and Patricia Cornejo, MDAfter participating in this educational activity, the radiologist should be better able to plan the appropriate imagingworkup of fetal neck masses, perform a differential diagnosis based on anatomic location and imaging features, andrecommend optimal management strategies.Category: NeuroradiologySubcategory: Pediatric ImagingModality: MRI, UltrasoundKey Words: Fetal, Head and Neck, Neuroradiology, Headand Neck MassesCongenital neck masses are rare lesions typically encountered during second-trimester anatomy ultrasound. Accuratediagnosis is crucial to appropriate ante- and perinatal management though imaging characterization remains a challenge. Ultrasound and MRI play complementary roles in thediagnosis of prenatal head and neck masses now facilitatedby the increased availability of fetal MRI, technologicadvancements in both imaging modalities and large tertiaryreferral centers with specialized care teams. As in both adultand pediatric head and neck imaging, a solid understandingof the neck anatomic spaces is a requisite to formulate afocused differential diagnosis. In this review, the more common fetal neck masses in four anatomic locations are presented. Unlike the wide spectrum of potential pathologiesencountered in children, fetal neck masses can be categorizedinto three major groups: tumors, vascular malformations,Dr. Vaughn is a Pediatric Neuroradiologist, Dr. Goncalves is a PediatricRadiologist, and Dr. Cornejo is a Pediatric Neuroradiologist, Department ofRadiology, Phoenix Children’s Hospital, 1919 E. Thomas Rd, Phoenix, AZ85016; E-mail: jvaughn2@phoenixchildrens.com.The authors, faculty, and all staff in a position to control the content of this CMEactivity have disclosed that they have no relationships with, or financial interestsin, any commercial organizations relevant to this educational activity.and congenital lesions. Using an anatomic and systematicapproach, the radiologist can narrow the differential diagnosis into a single or a limited list of possibilities. This articleprovides a focused review of the more common fetal head andneck pathologies, emphasizing their location and imagingcharacteristics. Based on these features, a reasonable differential diagnosis can be formulated and applied to prenatalcounseling, delivery management, and postnatal treatment.Continued advances in prenatal diagnosis and managementhave expanded the horizons of multiple disciplines that counsel and manage these patients. It is crucial for the pediatricradiologist and neuroradiologist to become familiar with thesonographic and MRI features of a variety of fetal conditions.While 2D ultrasound can identify almost all cases of fetalneck masses, MRI remains an important adjunct that aids inrefining the diagnosis, offering prognostic information to thefamily in terms of fetal morbidity and mortality and predicting the likelihood for ex utero intrapartum treatment (EXIT)procedure or caesarian section at delivery. Combined withadvances in fetal and neonatal surgery, more patients withneck masses that have historically led to fetal and neonataldemise secondary to airway compression are electing to carrythe pregnancies to term with improved survival.1 Radiologistsare therefore encountering fetal neck masses at a wider variety of stages of development and being asked to provideincreasingly specific and accurate information to aid in surgical decision-making, treatment planning, and prognosis.2 Insome cases, imaging characteristics allow for definitive diagnosis. However, findings are usually nonspecific and reporting a sound differential diagnosis can be intimidating. InLippincott Continuing Medical Education Institute, Inc., is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medicaleducation for physicians. Lippincott Continuing Medical Education Institute, Inc., designates this enduring material for a maximum of 2 AMA PRA Category 1Credits . Physicians should claim only the credit commensurate with the extent of their participation in the activity. To earn CME credit, you must read the CMEarticle and complete the quiz and evaluation on the enclosed answer form, answering at least seven of the 10 quiz questions correctly. This continuing medicaleducation activity expires on August 30, 2023.1
Co-EditorsBiren A. Shah, MDDetroit Medical CenterDetroit, Michiganbshah@dmc.orgPaul J. Spicer, MDUniversity of KentuckyLexington, Kentuckypaul.spicer4@uky.eduSection EditorsAiden Abidov, MDJohn D. Dingell VAMedical CenterGulcin Altinok, MDDetroit Medical CenterSteven L. Blumer, MDNemours/Alfred I. duPontHospital for ChildrenLiem T. Bui-Mansfield, MDUniformed Services Universityof the Health Sciencesthese cases, the use of an anatomic and systematic approach in combination with imaging characteristics can help limit thedifferential diagnosis. For the purposes ofanalysis, it is useful to divide the head andneck into four major general anatomic locations recognizing that these are comprised ofseveral subgroups of deep neck spaces delimited by the fascial planes.3,4In the anterior neck, masses that areencountered in the parapharyngeal space,carotid space, pharyngeal mucosal space, retropharyngeal, and visceral space will begrouped. In the posterior neck, masses locatedin the posterior cervical space will be grouped.In the paraspinal neck, masses located in theperivertebral space will be grouped, andfinally, the oral cavity contains a distinct subset of masses, which will be discussed.This article is meant to serve as an overviewof fetal head and neck masses rather than aAnteriorJanice Y. Jeon, MDMedStar Georgetown UniversityHospitalJames T. Lee, MDUniversity of KentuckyHaresh Naringrekar, MDThomas Jefferson UniversityRakesh Navuluri, MDUniversity of ChicagoSheena Saleem, MDChildren’s Hospital of MichiganMichael Seidler, MDUniversity of AlbertaSameer Tipnis, PhDMedical University ofSouth CarolinaWilliam Thompson, MDUniversity of New MexicoEditor EmeritusRobert E. Campbell, MD2Masses in the anterior fetal neck are muchmore common than masses in the posteriorfetal neck, with the major categories of massesfound here being tumors, vascular malformations, and congenital lesions including bothcysts and thyroid goiters (Table 1).TumorsFetal neck tumors are very rare, with themost common tumor being a cervical teratomaoccurring in approximately one in 20,000 to40,000 live births.2 These masses are oftenvery large and readily visible on secondtrimester sonograms. Cervical teratomasaccount for only 6% of all teratomas,5 with theTumors: teratoma, sarcoma, hemangiomaVascular malformations: lymphatic malformation, venous malformation, mixedLM/VM, high-flow lesionsCongenital: branchial cleft cyst, thyroglossal duct cyst, foregut duplication cyst,thymic cyst, dermoid/epidermoid, goiterPosteriorPrachi Dubey, MBBS, MPHHouston Methodist HospitalChristopher Fung, MDUniversity of AlbertaAnterior Neck MassesTable 1. Differential Diagnosis of Fetal Neck Masses Based on LocationIshani Dalal, MDHenry Ford HospitalAdrian Dawkins, MDUniversity of Kentuckycomprehensive review with emphasis onmasses that are more commonly encounteredand offer the radiologist an approach to interpretation and management in clinical practice.Tumors: hemangioma, fibroblastic and myofibroblastic tumors, rhabdoidtumors, sarcomas, kaposiform endotheliomaVascular malformations: nuchal lymphatic malformation, high-flow lesionsCongenital: occipital encephaloceleParaspinalTumors: neuroblastoma, gangliogliomaOral cavityTumors: teratoma (epignathus), epulis, ranulaVascular malformations: lymphatic malformation, high-flow lesionsCongenital: foregut duplication cyst, thyroglossal duct cyst, dermoid/epidermoid, lingual thyroidAnywherelesionsLymphatic malformations, venous malformations, mixed LM/VM, high-flowvascular malformations, hemangiomasThe continuing education activity in Contemporary Diagnostic Radiology is intended for radiologists.Contemporary Diagnostic Radiology (ISSN 0149-9009) is published bi-weekly by Wolters Kluwer Health, Inc. at 14700 Citicorp Drive,Bldg 3, Hagerstown, MD 21742. Customer Service: Phone (800) 638-3030; Fax (301) 223-2400; E-mail: customerservice@lww.com. Visitour website at LWW.com. Publisher, Stella Bebos. opyright 2021 Wolters Kluwer Health, Inc. All rights reserved. Priority Postage paid atCHagerstown, MD, and at additional mailing offices. POSTMASTER: Send address changes toContemporary Diagnostic Radiology, Subscription Dept., Wolters Kluwer, P.O. Box 1610,Hagerstown, MD 21740.PAID SUBSCRIBERS: Current issue and archives (from 1999) are available FREE online at www.cdrnewsletter.com.Subscription rates: Individual: US 786; international 1248. Institutional: US 1687, international 1885. In-training: US resident 156with no CME, international 178. GST Registration Number: 895524239. Send bulk pricing requests to Publisher. Single copies: 73.COPYING: Contents of Contemporary Diagnostic Radiology are protected by copyright. Reproduction, photocopying, and storage or transmission by magnetic or electronic means are strictly prohibited. Violation of copyright will result in legal action, including civil and/or criminal penalties. Permission to reproduce in any way must be secured in writing; go to the journal website (www.cdrnewsletter.com), select the article, andclick “Request Permissions” under “Article Tools,” or e-mail customercare@copyright.com. Reprints: For commercial reprints and all quantitiesof 500 or more, e-mail reprintsolutions@wolterskluwer.com. For quantities of 500 or under, e-mail reprints@lww.com, call 866-903-6951, or fax410-528-4434.Opinions expressed do not necessarily reflect the views of the Publisher, Editor, or Editorial Board. A mention of products orservices does not constitute endorsement. All comments are for general guidance only; professional counsel should be soughtfor specific situations. Indexed by Bio-Science Information Services.
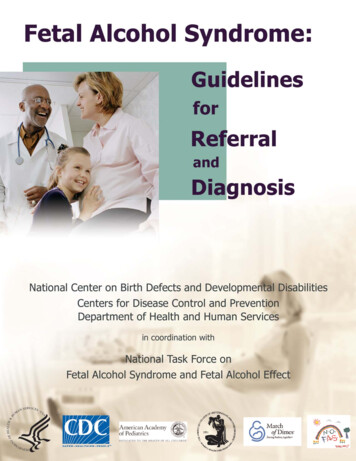
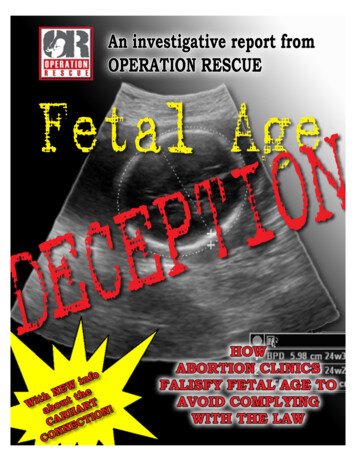
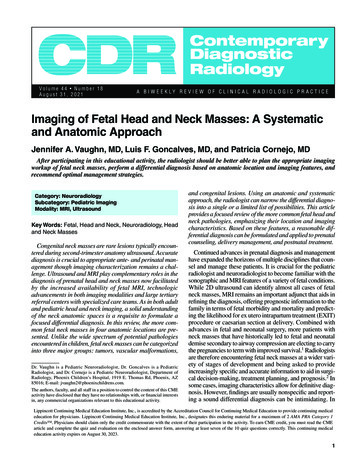
Figure 1. Cervical teratoma. Axial, T1-weighted MR image of theneck without contrast in a 1-day-old neonate demonstrates a largecystic and solid neck mass replacing the right lobe of the thyroid(arrow) with intact left thyroid lobe (star).majority located in the sacrococcygeal region. A germ celltumor, teratomas are thought by some to arise from thyroidtissue and may replace the thyroid gland rather than engulf it(Figure 1)—a feature that can be useful in distinguishing themfrom other large anterior cystic neck masses.6 They can beclassified into mature and immature subtypes, though the size,location, and extent of the tumor are much more important inpredicting the prognosis. Although these tumors can bedetected as early at 15 weeks’ gestation, the majority are notdiagnosed until the late second or third trimesters, suggestingthey can also develop later in the pregnancy.7Ultrasound, including Doppler and 3D imaging, and MRIare both useful in the diagnosis and evaluation of these fetusesin whom both fetal and maternal α-fetoprotein levels may benormal. On imaging, teratomas present as large cystic andsolid masses, which often hyperextend the neck and distortthe airway and vasculature. The use of T1-weighted highresolution isotropic volume excitation and gradient recallecho planar imaging (EPI) sequences may occasionally depictfat, internal hemorrhage, or calcium though these features arenot universally present in congenital cervical teratomas.Ultrasound is useful in evaluating the vascularity of the solidportion and to depict calcifications suspected by MRI, helping to differentiate teratomas from more complex venolymphatic malformations. Ultrasound can also most readilymonitor the tumor size and look for potential complicationsof airway obstruction including polyhydramnios and hydrops.Using a combination of T2-weighted single-shot turbo spinecho and heavily T2-weighted balanced turbo field echosequences in the axial, sagittal, and coronal planes, MRI canbest define the anatomic extent and internal characteristics ofthe mass. Advanced MR imaging techniques are also beingincreasingly applied to these challenging patients. The use ofcine imaging, such as a dynamic heavily T2-weighted nongated sequence, is capable of evaluating the fetal swallowingin real time and may prove to be helpful to evaluate for tonguemovement and/or involvement and for visualization ofdynamic airway obstruction. Volumetric measurements ofthe mass, and lungs in cases of severe airway compromise,can be obtained by applying superresolution postprocessingmethods to the original 2D multiplanar T2-weighted planesand aid in treatment planning and prognosis.8Although there are no specific selection guidelines in determining which fetuses should be delivered via EXIT procedure, certain imaging features predict a higher likelihood thata fetus may benefit from secured airway control before delivery given an elevated risk for severe airway obstruction. Theradiologist should thus be very descriptive in the specific location of the mass in the neck, outlining the relationship to theairway including whether or not the mass appears to arisefrom the airway, invade into the airway, or exert significantexternal compression on/deviation of the airway, as higherscores of airway deviation are predictive of a complicatedairway at birth.9 This is facilitated with T2-weighted MRI inwhich the entire course of the airway should be followed fromthe oropharynx to the carina (Figure 2). Internal characteristics of the mass are also important, such as whether the massis cystic or solid, as solid masses tend to have a higher propensity for airway obstruction. The presence of polyhydramnios should also be noted, as it is suggestive of impaired fetalswallowing and is predictive of a complicated airway at birth.Advances in neonatal surgery including the use of EXITprocedure, surgical resection of the teratoma while on placental support, and early surgical resection at specialized tertiarycenters have improved the morbidity and mortality of thesefetuses, which unfortunately still remains poor.Vascular MalformationsLymphatic malformations (LMs) are the most commoncervical tumor with variable reported incidence of four in10,000 and one in 16,0000 births,10 with the largest proportion seen in the posterior neck.11 These lesions have beenpreviously called by many names including cystic hygromawhen occurring in the nuchal location, and lymphangioma,although LM remains the most appropriate term.12 LMs maybe either macrocystic or microcystic in nature dependingFigure 2. Cervical teratoma. Axial, T2-weighted MR image of theneck in a 32-week fetus demonstrates a cystic and solid neck mass(star), which deviates the airway ventrally and to the left (arrow).3
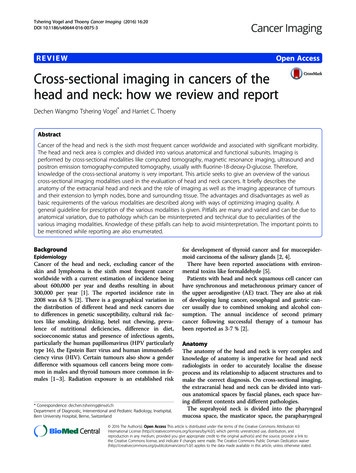
upon the size of the cystic spaces. They may also consist ofa mixture of venous and lymphatic components giving riseto combined lesions known as venolymphatic malformations.In the anterior neck, LMs are the main differential for a largeanterior cystic neck mass.Ultrasound is a useful first modality to document the cysticnature of these masses and exclude internal vascularity apartfrom within the internal septations, helping to differentiatethe more common subtypes of purely lymphatic and cysticvenolymphatic malformations from teratomas. The morecomplex venolymphatic malformations, which contain variable amounts of solid components and calcified phleboliths,remain a diagnostic challenge, as they can appear very similar to teratomas on prenatal imaging.13,14 LMs have the propensity to undergo internal cyst hemorrhage leading tocharacteristic fluid-blood levels. Similar to teratomas, MRIis useful to evaluate these lesions to document the positionof the airway and assess for deep neck extension of thesetransspatial lesions. LMs typically cause less mass effectcompared with similarly sized teratomas leading to lesshyperextension of the neck and less deviation and compression of the airway, vascular structures, and thyroid gland(Figure 3). They may also insinuate into the chest, mediastinum and axilla, a feature more commonly seen with venousLMs and LMs than cervical teratomas. LMs may grow,regress, or remain stable during the gestation and thus serialfollow-up is advised. Prenatal aspiration of cyst fluid can beconsidered in cases of rapid growth, infection, or hemorrhageto facilitate delivery but is rarely performed.10 Lesion airwayinvolvement necessitates similar considerations for cesareansection and EXIT procedure at delivery though less frequently needed than with similarly sized teratomas.Congenital MassesCongenital Cysts and Thyroid GoiterThe incidence of neck cysts detected during the fetal periodis unknown but very rare.15 Possible etiologies include thesame pathologies as seen in infants and young childrenincluding branchial apparatus anomalies (Figure 4), thymiccysts, thyroglossal duct cysts, foregut duplication cysts, andneurenteric cysts. In all instances, these fetuses may need tobe followed with serial imaging, as involvement of the airwaywith compromise will necessitate consideration for alternatedelivery plans. The prognosis for these patients is typicallyexcellent following curative surgical excision after delivery.Thyroid goiter is a very rare cause of a fetal neck mass presenting as diffuse enlargement of the thyroid gland and diagnosed most frequently in the late second trimester.15 It may beseen with fetal hyperthyroidism, usually in the setting of maternal Grave’s disease or fetal hypothyroidism, typically in thesetting of maternal antithyroid treatment, maternal iodine deficiency, or maternal antithyroid antibodies. Congenital dyshormonogenesis is the most common cause if maternal thyroiddisease is excluded.15 On ultrasound the thyroid will beenlarged, can vary in echogenicity, and is hypervascular(Figure 5). Direct evaluation of fetal thyroid function requirescordocentesis and, depending upon the underlying cause, willnecessitate various in-utero treatments. Goiters can grow to asignificant size and compromise the airway leading to furtherconsiderations regarding delivery planning.4Figure 3. Cervical LM.Coronal ultrasound withcolor Doppler (A) and coronal, T2-weighted MR image(B) of the neck in a 35-weekfetus demonstrate an avascular transspatial cysticneck mass (blue star),which insinuates aroundthe airway at the level of theglottis and extends inferiorly around the infraglottic airway withintact appearance of the vocal folds (red arrow) and only minormass effect on the airway (green asterisk).Posterior Neck MassesAs mentioned previously, fetal posterior solid neck massesare comparatively rare than anterior neck masses; however,cystic masses in this location are the most common neck massesencountered overall in the fetus.16 Masses in this location fallinto the categories of tumors, vascular malformations, and congenital lesions including occipital encephaloceles, which arebeyond the scope of discussion of this review (Table 1).TumorsVascular tumors, in particular congenital hemangiomas,likely comprise the majority of solid posterior fetal neckmasses17 though the literature remains sparse on the incidence of tumors in this location. Hemangiomas are nowhistologically classified based on the presence of glucose-1transporter into infantile and congenital subtypes with thecongenital form being further divided into those that rapidlyinvolute (RICH) and those that do not (NICH). Congenitalhemangiomas are present at birth and have been diagnosedas early as the first trimester. Although the RICH subtype ismore common, on imaging, both types of congenital hemangiomas appear similar presenting as well-circumscribed solidmasses with internal vascularity and high-flow velocity onultrasound. On MRI, they have heterogeneous signal onT2-weighted images (Figure 6) and may demonstrate flowvoids on EPI sequences related to the high-flow internal vessels and enlargement of the feeding vessels in the neck.Hemangiomas may occasionally calcify or have cysticspaces17 and should not be mistaken for a teratoma. Diagnosisof hemangioma is important as they are associated withhydrops and high-output cardiac failure and therefore requireserial imaging with consideration to fetal echocardiography.The differential diagnosis for posterior solid neck massesincludes very rarely Kaposiform endothelioma, another vascular mass that is typically larger in size, can behave aggressively, and is associated with the Kasabach-Merritt syndrome;
high association of other anomalies, a thorough evaluation ofthe heart, skeletal structures, genitourinary, and central nervous systems should be undertaken when a nuchal LM isencountered and referral for fetal echocardiogram and genetictesting if desired. In the absence of aneuploidy, cardiac malformation, and with normal sonographic anatomy, there is avery high likelihood of a good outcome.19Paraspinal MassesFigure 4. Third branchial cleft cyst. Coronal, T2-weighted MRimage of the neck in a 32-week fetus demonstrates a simpleappearing cyst in the ventral paramedian infrahyoid neck (arrow)extending inferiorly to the level of the thyroid.and other rare rhabdoid, fibrous, and sarcomatous massesincluding fibrosarcomas and myofibromas, which can appearsimilar on MRI with heterogeneous signal on T2 and internalflow voids on gradient echo sequences (Figure 7) but typicallydemonstrate less vascularity on ultrasound compared withhemangiomas.Fetal paraspinal masses are extremely rare with a limited setof differential possibilities arising from cells in the sympatheticneural chain including neuroblastoma and ganglioneuroma.Congenital cervical neuroblastoma is very rare with a reportedincidence of 4.4% of all types of congenital neuroblastomas,the most common location being in the fetal adrenal gland.20On ultrasound, masses are typically solid and contain scatteredcalcifications, areas of necrosis and/or hemorrhage. If suspected, fetal MRI should be performed to evaluate for metastatic disease, which may be seen in the liver, bones, skin,lymph nodes, placenta, and umbilical cord.21 On MRI thesetumors present as solid or mixed solid and cystic vascularparaspinal masses, which may splay the ribs (Figure 8) anddemonstrate internal calcification or hemorrhage. Evaluationof tumor extension into the neural foramina and assessment ofextremity motion are paramount, as the presence of cord compression may lead to consideration for premature delivery.Vascular MalformationsNuchal LM has a reported incidence of 0.75%17 and isunique compared with the nonnuchal LM discussed previouslyin that there is a relatively high association with chromosomalabnormalities, reported up to 51% for those diagnosed in thefirst trimester15 including association with trisomy 21, 13, and18, Turner’s syndrome, several different duplication, andmicrodeletion syndromes and other genetic disorders including Sotos syndrome, Cornelia de Lange, and Roberts syndrome among others.18 As with LMs elsewhere in the neck,these lesions present as large avascular cystic multiseptatedmasses with a propensity for internal hemorrhage. Given theOral Cavity MassesFigure 5. Goiter. Coronal ultrasound demonstrates diffuseenlargement and increased echogenicity in the thyroid gland(star) surrounding the fetal airway (arrow). (Courtesy of Dr. MarioJulio Franco, Clinica Materno-Fetal, Florianopolis, Brazil.)Figure 6. Hemangioma. Axial, T2-weighted MR image in a34-week-fetus demonstrates a heterogeneous signal in posteriorwell-circumscribed neck mass (arrow) with prominent vascularityon ultrasound (not shown).Fetal oral cavity masses are rare though several entitiesencountered in this location have a specific imaging appearance allowing the radiologist to be definitive in their diagnosis. The vast majority of masses encountered in this location5
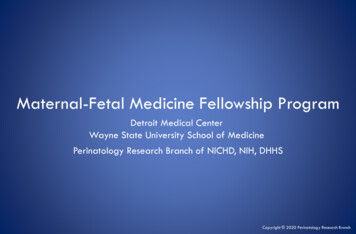
Figure 7. Myofibroma. Axial EPI image in a 36-week fetus demonstrates prominent internal flow voids (arrow) in a large posteriorcervical mass.are benign22; however, due to their location, they can have asubstantial impact on fetal morbidity and require specializedperinatal management.TumorsTeratomas occurring in the oral cavity are the most rarelyencountered anatomic site, accounting for only 0.47% of allcongenital teratomas.2 Although they often appear to be centered in the oral cavity and project out the mouth, theseFigure 8. Paraspinal neuroblastoma. Sagittal, T2-weighted MRimage in a 30-week fetus demonstrates a mildly T2 hypointenseparaspinal mass, which splays the ribs posteriorly (arrow).6Figure 9. Epignathus. Sagittal CT scan of the face in a 1-day-oldneonate demonstrates a large heterogeneous cystic and solidmass with fat density and internal calcifications centered in theposterior palate (star) extending out of the mouth (not shown)and nasal cavity and extending intracranially (arrow) with secondary obstructive hydrocephalus.masses arise from the palate in cells from the craniopharyngeal canal or Rathke’s pouch.23 On imaging the componentsare heterogenous, solid, and cystic and typically reach a largesize at presentation making them readily detected on screening ultrasound. Ultrasound can variably demonstrate calcifications and internal vascularity. MRI is useful in thesepatients to define the full anatomic extent including establishing the relationship to the airway and evaluating for intracranial extension. These tumors may grow rapidly, thus serialimaging is important. Unfortunately, the prognosis of thesefetuses is very poor due to airway involvement, which canlead to polyhydramnios and the potential for intracranialFigure 10. Epulis. Sagittal, T2-weighted MR image in a 33-weekfetus demonstrates a well-circumscribed, T2 hypointense, pedunculated mass arising from the maxillary gingiva protruding out ofthe oral cavity (arrow).
ConclusionEncountering a fetus with a neck mass can seem daunting;however, the use of an anatomic and systematic approachcan help narrow the differential and, in some cases, providea specific prenatal diagnosis. Familiarity with the appearance of the most commonly encountered congenital neckmasses on both ultrasound and MRI, and knowledge ofsome specific imaging features, which can affect the anteand perinatal clinical management, is critical for optimalpatient outcome.ReferencesFigure 11. Foregut duplication cyst. Sagittal, T2-weighted MRimage in a 24-week fetus demonstrates a well-circumscribed,simple-appearing cyst in the anterior tongue (arrow).extension with secondary hydrocephalus and mass effect(Figure 9).Another entity with a specific imaging appearance in thefetal oral cavity is the congenital granular cell tumor or epulis. These masses are gingival in origin arising from the softtissue of the maxillary or mandibular alveolus with intactunderlying bone. They present most often in the third trimester with a significant female predominance (8–10:1).24 Theimaging appearance is that of a pedunculated mass, whichprotrudes out of the oral cavity (Figure 10). They are hypointense in signal on T2-weighted imaging and ultrasound maydemonstrate a vascular stalk. The prognosis for these patientsis typically excellent, as these rarely impair fetal swallowingor impact the airway, though follow-up with serial ultrasoundto monitor growth and evaluate the extent is advised as occasionally they may grow large and lead to obstruction.Lastly, one may occasionally encounter cystic masses inthe fetal oral cavity. Here, an anatomic approach can helpnarrow the possibilities and provide a useful differential diagnosis. When a simple thin-walled unilocular cystic lesion isencountered in the midline anterior tongue, one should consider a foregut duplication cyst, dermoid, or LM (Figure 11).MRI with diffusion-weighted imaging can occasionally behelpful in differentiating a dermoid/epidermoid, which maydemonstrate reduced diffusivity, though often a definitivediagnosis prenatally is not possible. In the midline base oftongue, a thin-walled unilocular cyst should prompt one toconsider congenital lesions arising from the thyroid includingthyroglossal duct cyst. Finally, in the lateral oral cavityinvolving the sublingual and/or submandibular space, a cysticlesion should prompt consideration of a ranula or LM.1. Cass DL. Impact of prenatal diagnosis and therapy on neonatal surgery. SeminFetal Neonatal Med. 2011;16(3):130-138.2. Tonni G, De Felice C, Centini G, et al. Cervical and oral teratoma in thefetus: a systematic review of etiology, pathology, diagnosis, treatment andprognosis. Arch Gynecol Obstet. 2010;282(4):355-361.3. Harnsberger HR, Glastonbury CM, Michel MA, eds. Diagnostic Imaging:Head and Neck. Philadelphia, PA: Lippincott Williams & Wilkins; 2010.4. Meesa IR, Mukherji SK. A simplified approach to the spaces of the suprahyoid neck. Appl Radiol. 2017;46(4):6-14.5. Barnes L, Eveson JW, Reichart P, et al. Pathology and genetics of head andneck tumors. In: Kleihues P, Sobin LH eds. World Health OrganizationClassification of Tumors. Lyon, France: IARC Press; 2005.6. Riedlinger WFJ, Lack EE, Robson CD, et al. Primary thyroid teratomas inchildren: a report of 11 cases with a proposal of criteria for their diagnosis.Am J Surg Pathol. 2005;29(5):700-706.7. Daskalakis G, Efthimiou T, Pilalis A, et al. Prenatal diagnosis and management of fetal pharyngeal teratoma: a case report and review of the literature.J Clin Ultrasound. 2007;35:159-163.8. Uus A, Zhang T, Jackson LH, et al. Deformable slice-to-volume registrationfor motion correction of fetal body and placenta MRI. IEEE Trans MedImaging. 2020;39(9):2750-2759.9. Lazar DA, Cassady CI, Olutoye OO, et al: Tracheoesophageal displacementindex and predictors of airway obstruction for fetuses with neck masses. JPediatr Surg. 2012;47(1):46-50.10. Oosthuizen JC, Burns P, Russell JD. Lymphatic malformations: a proposedmanagemen
Detroit Medical Center Detroit, Michigan bshah@dmc.org Paul J. Spicer, MD University of Kentucky Lexington, Kentucky paul.spicer4@uky.edu seCtion editors Aiden Abidov, MD John D. Dingell VA Medical Center Gulcin Altinok, MD Detroit Medical Center Steven L. Blumer, MD Nemours/Alfred