Transcription
DATA AND ADVANCED ANALYTICS INHIV SERVICE DELIVERYUse Cases to Help Reach 95-95-95
The lead author of this report was Boston Consulting Group (BCG), incollaboration with the United States Agency for International Development(USAID) South Africa with additional funding and support from USAID’sCenter for Accelerating Innovation and Impact (CII). This report could nothave been written without the support and invaluable contributions of theUSAID team, programme partners, industry experts, workshop participants,and all who contributed their time, insights and experience. The authorsparticularly wish to thank the participants of this review from Project Last Mileand Panagora Group.Launched in 2003, the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) isthe largest commitment by any nation to address a single disease in history, enabledby strong bipartisan support across nine U.S. congresses and three presidentialadministrations, and through the American people’s generosity. The USAID Officeof HIV/AIDS drives the Agency’s efforts under PEFPAR in controlling the HIV/AIDSepidemic by providing global expertise to strengthen the impact of USAID’s overallresponse.USAID’s Center for Innovation and Impact (CII) takes a business- minded approachto fast-tracking the development, introduction, and scale-up of health interventionsthat address the world’s most important health challenges. CII invests seed capitalin the most promising ideas and novel approaches, using forward-looking businesspractices to cut the time it takes to transform discoveries in the lab to impact onthe ground.Boston Consulting Group (BCG) is a global management consulting firm and aleading advisor on business strategy. BCG works with organizations in the social,public, and private sectors to deliver solutions to the most complex problems incontemporary society.BCG GAMMA is BCG’s global team dedicated to applying artificial intelligence andadvanced analytics to business at leading companies and organizations. The teamincludes 800-plus data scientists and engineers who apply AI and advanced analyticsexpertise (e.g., machine learning, deep learning, optimization, simulation, text andimage analytics) to build solutions that transform business performance. BCGGAMMA’s approach builds value and competitive advantage at the intersectionof data science, technology, people, business expertise, processes and ways ofworking.For contact information, and to download the latest version of Data and Advanced Analytics in HIV ServiceDelivery: Use Cases to Help Reach 95-95-95, please visit www.usaid.gov/cii.
Table of Contents1. Foreword.22. Introduction.33. Executive Summary.54. Understanding pain points.74.1 Key themes .74.1.1 Focusing. 74.1.2 Tailoring. 84.1.3 Touchpoints. 84.1.4 Tracking. 94.1.5 Responsiveness. 95. Addressing pain points through use cases.115.1 Introduction to advanced analytics use cases. 115.2 Prioritization criteria. 115.3 Ten impact-generating use cases. 125.4 Key learnings. 215.4.1 Factors affecting impact. 215.4.2 Feasibility. 236. Data sources, challenges, and opportunities.256.1 Patient-level data in LMIC countries. 256.2 External data considerations and sources. 277. Next steps: Key considerations for developing a use case.308. Conclusion.339. Appendix.34A.B.C.D.E.Glossary. 34Long list of pain points. 35Long list of use cases. 40Detailed descriptions of impact and feasibility sub-criteria. 42Categories and details of external data sources. 43
1. ForewordI write this from my post as a member of the United States Agency for International Development (USAID) team inSouth Africa and a privileged contributor to this compendium of good ideas. The United States government has hadthe privilege of supporting the South African government to help maintain almost 4 million people living with HIV ontreatment, with the aim of supporting all 7.5 million people living with HIV before the end of 2020. With an everchanging and complex world, I am grateful to the team at Boston Consulting Group’s (BCG) Scale for Impact project forpulling together this useful tool when the world needs it most.South Africa made strides in controlling the HIV epidemic by developing some of the most innovative approaches todifferentiating models of treatment delivery. While the HIV program is no stranger to combatting fear, stigma, limitedresources, and staff shortages, the health system will be tested more than ever in light of COVID-19. The disease enteredSouth Africa’s borders as the country was making tremendous strides toward reaching its global 90-90-90 HIV epidemiccontrol targets. The introduction of COVID-19 presents new challenges for the provision of care and calls for innovativeways to address the barriers that clients face when obtaining care, so that we don’t lose the gains of recent years.Despite its focus on data and advanced analytics, this report is above all else about the client and the health worker. Theauthors mapped the common journeys of clients (typified by the character named “Gift”) and health workers (typifiedby the character “Ruth”). In a report about data, it’s crucial to humanize these groups and provide narratives of theirexperiences to illustrate pain points faced by the clients and staff. Pain points are the millions of tiny inconveniences andinstances of confusion, duplication, and worry that prevent large-scale programs from sustainably succeeding. This reportdisplays a comprehensive tabulation of what a common HIV program faces in providing a framework for readers toprioritize the issues in their own contexts. Print out the accompanying graphic showing the synthesized list of pain points,hang it over your computer, look at it every day—never forget the human factors that drive epidemic control and anefficiently operating program.The authors of this report also gifted us all with a modern, shiny toolbox: a range of approaches related to predictivemodeling, machine learning, artificial intelligence, sentiment analysis, and geospatial analytics, tied under the commontheme of advanced analytics. For each problem, the authors tapped into one of the largest teams of data scientists in theworld, the BCG GAMMA team, to identify problem-solving use cases that could be applied using the data commonlyavailable in a national HIV program and modern data sources.To the reader, may the ideas in this report inspire you to ask, “How might we ?” How might we use data from busroutes and satellite maps to deliver services to clients who move for seasonal work? How might we promote clientadherence by optimizing how we implement appointment reservations at facilities? How might we use client attributesto learn who may be at higher risk for getting lost in the health system? How might we achieve a balance of preservingethical protections for individual data while leveraging the possibilities of modern technology? These questions and moreare reviewed in this report with recommendations for resourcing and implementation.Many of us working in HIV programs globally are often enmeshed in our own program data. This report reminds us thatthere are diverse sources of information relevant to our efforts beyond the conventional. After all, the clients we serveoften use social media, take public transportation, seek private health care, and buy goods from local pharmacies. Theapplication of diverse data sets emphasizes the importance of clients’ lives outside of health facilities. When we designprograms that synthesize the complex lives of our clients and health workers, we affirm their personhood beyond merelyseeing them as patients and clinicians. This is a necessary step toward controlling the HIV epidemic and ensuring theglobal effort to control COVID-19 better prepares the global public health community to protect the well-being of futuregenerations.Josef TayagHealth Systems Strengthening Team Lead – ActingUSAID South Africa/Health Office2
2. IntroductionGlobal health efforts have made significantprogress against the HIV/AIDS pandemic.1 At theturn of the millennium, less than seven hundredthousand of the almost thirty four million people livingwith HIV (PLHIV) had access to antiretroviral therapy(ART). In 2019, that number stood at around twenty-fivemillion of the thirty eight million PLHIV.As the gap to reaching targets of controlling andeliminating this pandemic closes, the difficulty to achievethem increases. The year 2020 marks a transition:the Joint United Nations Programme on HIV/AIDS’s(UNAIDS) target of 90-90-902 by the end of this yearbecomes 95-95-953 by 2030. However, many countrieswill struggle to achieve 95-95-95 in the next ten years.Global data suggests that in 2018, 79% of PLHIV wereaware of their status, and 78% of PLHIV aware of theirstatus were on stable treatment, equivalent to 62% ofall PLHIV. Of the PLHIV on stable treatment, 86% werevirally suppressed, which is a laudable achievement, butonly equivalent to 53% of all PLHIV.4,5 Achieving 95%treatment rates will require continued innovation ofpersonalized and differentiated care models. General,widespread interventions—while important to maintaina critical mass—will not be enough for the remainingindividuals who are hard to find, who have difficultybeing linked to treatment, or who have dropped out oftreatment.We think that data could make the difference. Vastvolumes of structured and unstructured data arecollected on the millions of PLHIV globally, but sufficientinsight isn’t being gained from it. This could be improvedthrough more widespread use of advanced analyticstechniques such as clustering to better understand atrisk populations, predictive modeling to understandlikelihood of risk for an individual, and optimizationof ART inventory. The insight garnered using thesetechniques can be used to predict patterns of disease,optimize treatment decisions, and improve patientexperience, to name a few examples.Advanced analytics has an important role to play byaddressing crucial pain points that contribute to thegap between where we are today and 95-95-95. In theprivate sector, advanced analytics has been leveraged foryears with success ranging from optimizing manufacturingprocesses to understanding customers better to enabletargeted product offerings. Identifying high-impact,feasible use cases for advanced analytics and addressingthe data access and quality requirements to supportthem are interlinked and must be tackled together. Betterdata quality and integration in low- and middle-incomecountries (LMIC) could ensure the usefulness of this data.Without this improvement, it will be difficult to close thegap toward 95-95-95 in the years to come. This is not justan opportunity, but an imperative: advanced analytics isthe lever enabling us to meet increasingly ambitious goalsin a resource- constrained world. In countries where theHIV/AIDS burden is high, budgets are being stretched,both for global donors and local governments, even astargets to control HIV increase.This repor t reflects the output of an analysis conductedby Boston Consulting Group (BCG) on behalf of theUnited States Agency for International Development(USAID). The objective of the analysis was to identifyhigh-priority advanced analytics use cases that couldimprove HIV service delivery globally. The identificationof use cases is necessarily informed by a review of themost pressing challenges in HIV service delivery, witha focus on improved data quality and utilization. Basedon this review, our ideation process led to a long listof use cases that we prioritized and refined. We alsoconsidered enablers for these use cases: how thequality of patient-level treatment data can be improvedand how external data sets can be better leveragedto enrich insight. 6 Lastly, for those looking to applyanalytics use cases in their own work, we speak to keyconsiderations for implementing a por tfolio of use casesover time.Our objective is to help drive global thinking on howto leverage advanced analytics to improve HIV service3
delivery, and more specifically, to support programmanagers and implementers to include use cases in theirstrategy to reach 95-95-95. Key learnings gained fromour analysis can provide a useful launch pad for othersseeking to do similar work in different contexts.Footnotes1. Malaria No More and World Health Organization statistics.2. This means 90% of PLHIV are aware of their status, of whom 90% are on HIV treatment, of whom 90% are virally suppressed.3. This means 95% of PLHIV are aware of their status, of whom 95% are on HIV treatment, of whom 95% are virally suppressed.4. Data from the UNAIDS treatment cascade, published in 2019.5. Viral suppression refers to an HIV-positive person having a very low level of HIV in his or her body: less than 1,000 copies of HIV per milliliter ofblood, according to UNAIDS.6. For the purposes of this work, external data sets are defined as non-health data sets, and health data sets curated or owned within the privatesector, that can provide insight into population behavior and area trends.4
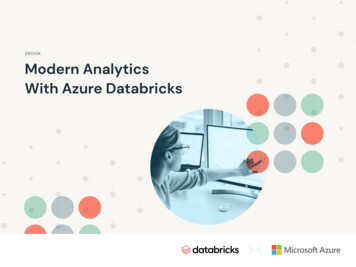
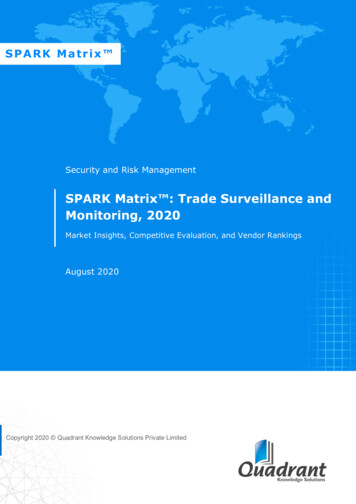
3. Executive SummaryData and advanced analytics offer an opportunity toimprove service delivery for the millions of PLHIVacross the globe, while using limited resourcesmore effectively. The first step toward harnessinganalytics toward the ultimate goal of reaching an AIDSfree generation is understanding where issues arise inHIV service delivery along the patient journey, acrossdiagnosis, treatment, and adherence. In this analysis, overtwo hundred pain points were gathered from stakeholderdiscussions, covering each step in the patient journey aswell as three cross-cutting categories: data management,operations management, and staff. From our discussions,we saw a concentration of pain points in early treatment,which is understandable considering the challenges facedin keeping PLHIV on treatment in the first few months,when the majority of patient loss to follow-up (LTFU)usually occurs. Across the patient journey, pain points canbe categorized into five key themes: Focusing, Tailoring,Touchpoints, Tracking, and Responsiveness, which mustbe addressed to achieve 95-95-95 in countries with ahigh HIV burden and are described in Section 4.As the overviews of the use cases provided in Section5.3 show, benefits to undertaking a use case vary but areprojected to be significant across multiple dimensions ofclinical outcomes improvement as well as cost reduction.For example, patient LTFU can be reduced by over 10%in some cases, and cost reductions of up to 15% in therelevant spend category can be achieved. Commonfeasibility challenges arose across the ten priority usecases relating mainly to change management and datarequirements. Mitigating actions to these challenges areparticularly important, such as reducing the numberof end users for the use case, centralizing the use caseand avoiding real-time processing, determining datarequirements early on, partnering with the owners ofpatient-level data sets, and avoiding input data from onthe-ground collection wherever possible. Overall, moreuse cases in the top ten qualify as “big bets”—high impactbut relatively lower feasibility—rather than “quick wins”—relatively higher feasibility but lower impact—which showsthe exciting potential of advanced analytics use cases butthe significant effort required to realize that potential.Advanced analytics use cases are proposed as a solutionto address many of these patient journey pain points.Around forty use cases were conceptualized in a longlist and prioritized by impact and feasibility. The resultingshortlist of ten priority use cases is shown in Figure 1.All use cases require quality data, particularly at thepatient level, and ensuring quality means ensuring timelyand accurate capturing and validation of patient-leveltreatment data, establishing clearer ownership and roledelineation, and creating streamlined programmatictools to support these improvements, among otherbest practices described in Section 6.1. Data outside thepublic health ecosystem can also play an important role inproviding insights into population behavior and trends, aswell as area-level events that could affect the populationand facility operations in an area. A wealth of populationand area data is available, as described in Section 6.2and the appendix, with data vendors offering purchase orsubscription packages and research institutions providingopen-access resources. In many instances, however, datapartnerships with other organizations that either own oraggregate private-sector data are necessary to unlockthe full potential of use cases. These partnerships requirerigorous adherence to data privacy regulations, strictdata governance processes, and a carefully consideredapproach toward establishing data-sharing agreements.Detailing the features and end-to-end processes ofthese ten use cases helped us to do a more in-depthimpact and feasibility assessment of them. Althoughthese use cases have global relevance for the HIVlandscape, specific priorities could differ based on acountry’s context, constraints, and 95-95-95 objectives.A key example of this is whether a country’s focus ison initiation or retention. Another growing focus areais retaining patients in less resource-intensive treatmentmodels, such as decentralized medicine pick-ups.1 Theconcentration of use cases around the early and stabletreatment steps of the patient journey reflects this.Please see the long list of use cases in the appendix tothis report for additional suggestions of relevant usecases for other treatment steps.5
Figure 1: Ten impact-generating use cases along the patient journey1st 95 DiagnosisPreventione.g.,MMC/PrEPCase findingTesting2nd 95 TreatmentCounselingABThe High-RiskHotspotterIdentifygeographichotpots of at-riskpeople andundiagnosedPLHIVThe Risk RaterPredict high-riskin-facility patientsfor testingLinkage3rd 95 Viral pressionThe Fall-OutThe MobilityForecasterMonitorPredict LTFU from Optimize patientearly treatmenttracking andbetterunderstandDpatient mobilityThe LTFU LocatorIdentify geographichotspots of rOptimise thenumber ofpatients onmultimonth anddecantedtreatment modelsEThe Better BookerOptimize patientexperience byimprovingschedulingof appointmentsH The Staff Supporter Optimize staff allocation across facilitiesIThe Stock Saver Predict demand-driven stock requirements at facility levelJThe Treatment Data Triangulator Triangulate treatment data against other sourcesWhere to from here? Although having a “portfolio”of priority use cases to choose from is helpful, mostorganizations will be able to roll out only one to two usecases successfully within a year. This is due to the intensityof the use case delivery model: the process of taking ause case from an idea to a fully deployed and scaledup product in use by everyday operations. Each phaseof the delivery model brings different considerations,but an overarching imperative is to ensure that thedelivery squad, the team responsible for the use casedevelopment, is fully dedicated to make it a success. Thisrequires strong governance, as well as dedicated capacityfrom the product owner, end-user representatives, andsubject-matter experts. Using an agile, sprint-basedapproach can allow impact to be seen on the groundin an earlier stage in the process rather than after fullrollout.Throughout this report, you will be accompanied by twoillustrative personas, Gift and Ruth. Gift is a young manwho was recently diagnosed with HIV, and Ruth is a casemanager working in a large public hospital. 2 Their painpoints are highlighted as examples of first-handexperiences with challenges in the HIV landscape. Wealso use instances in their daily lives to show what HIVservice delivery could look like with a few of our highestimpact use cases implemented. Although we providedetail to illustrate our analysis, please see the appendixfor the long lists of pain points and use cases referred toin the report.A user-centric, solution-driven approach has beenadopted to build use cases bottom-up that address thespecific issues faced by stakeholders in the HIV landscape.This approach also ensures that, once implemented, thesolutions have strong user pull. We chose not to focuson creation of digital tools or technologies, such as apps,websites, block chain, and the Internet of Things, butrather we focus the use case design on describing whatis the actual data insight or usage that creates value forthe system. Therefore, in some cases, an app or otherplatform may serve as the interface for how a userinteracts with the use case, but it is not the focus of theuse case. This definition was relevant for our work, butmay be too restrictive for different contexts, constraints,and objectives.Footnotes1. Decentralized models provide patients with a channel to receive ART outside a health care facility. Please see 4.1.3, “Touchpoints,” for more explanation.2. Please note that these personas are entirely fictional, and any resemblance to actual persons is coincidental.6
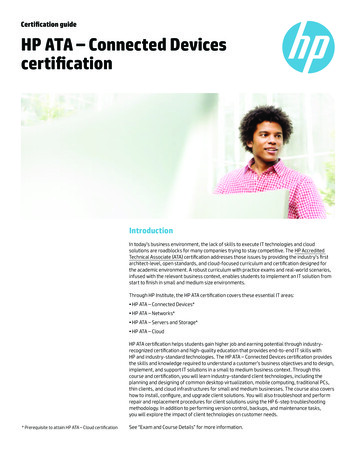
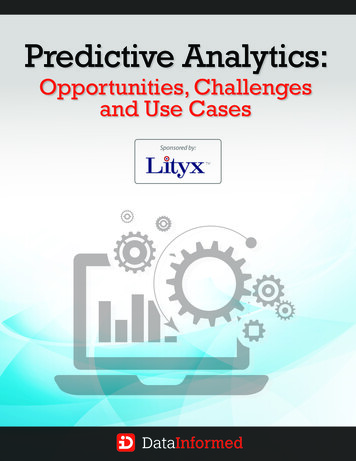
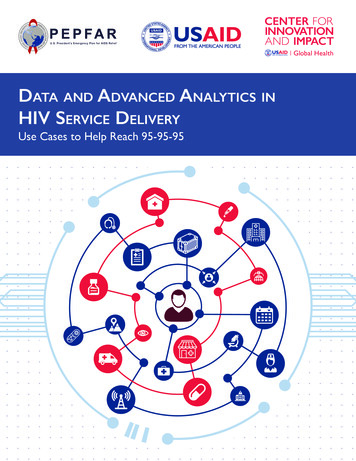
4. Understanding pain pointsTo understand the potential impact of advancedanalytics use cases in HIV service delivery, itis important to determine where data-driveninterventions are the most necessary. The patientjourney, illustrated in Figure 2, describes the differentstages of HIV care and treatment for patients who remainon ART until they are virally suppressed and transferredto differentiated models.1 Although the illustration is toolinear to be an accurate representation of the varied andoften interrupted journeys that PLHIV take, it helps todifferentiate events and stages at which use cases can betargeted to address inefficiency. In addition, the patientjourney is a globally relevant representation of stepstoward 95-95-95.To identify pain points, stakeholders in the HIV landscapewere asked about the biggest challenges in their dayto-day work—the unanswered questions or missinginformation that, if addressed, could have the largestimpact on achieving 95-95-95. 2,3,4 The pain pointsheard were organized by the patient journey steps tounderstand where and how the pain points affect HIVservice delivery. To properly capture cross-cutting painpoints, three overarching categories were included: datamanagement, operations management, and staff.Pain points heard were most concentrated in earlytreatment. This is to be expected given the challengesPLHIV face when starting an intensive treatment regimen.However, pain points will differ based on where a countryexperiences the greatest gap to achieving 95-95-95. Forexample, in some sub-Saharan African countries, thegreatest gap is in the first 95: diagnosis. In 2018, the shareof PLHIV who knew their status was 72%in Mozambique, 42% in Angola, and only 24% in SouthSudan. 5 In some contexts, up to 80% of treatment LTFUis estimated to occur in the first six months of treatmentdue to lack of overall case management, side effects ofART, poor initial health, inconvenient treatment options/hours, and poor professional service or judgment fromhealth care workers (HCWs). 64.1 Key themesFive key themes emerged from our pain pointdiscussions: Focusing, Tailoring, Touchpoints, Tracking,and Responsiveness (see Figure 3).4.1.1 FocusingFocusing refers to identifying and locating those at highrisk of being HIV positive. In sub-Saharan African countrieswith high incidence rates outside of key populations,7case finding has become increasingly complex. Programmanagers face difficulty in segmenting vulnerablepopulations, 8 which are comparatively large, and whosehigh-risk individuals are often not easily identifiable.Information that could be used to identify high-riskindividuals is often sensitive and hard to come by, such astheir sexual history and incidence of sexually transmittedinfection. Similar concerns apply to undiagnosed andLTFU PLHIV. Although we have a general understandingof risk factors, we struggle to identify risk profiles basedon individuals’ unique combination of these factors. Inaddition, it is difficult to locate high-risk individuals andcommunities. If we could better understand risk andidentify risk pockets, we could better focus resourceswhere they are most needed.Figure 2: Linear illustration of a patient’s journey through HIV care and treatmentPreventione.g.,MMC/PrEP1st 95 DiagnosisCase findingTesting2nd 95 TreatmentCounselingLinkageEarlytreatment3rd 95 Viral tiatedmodels7
PAIN POINTDon’t know how toidentify or specificallylocate “at-risk” peopleCan’t tailor interventionsor treatment journeybased on an individualrisk profileFacility-basedtouchpoints need to beoptimized (by number,type, staffing, timing)Can’t track a patientacross the treatmentjourneyCan’t respond todemand/supply of ARVsor facility issues in realtimeRELEVANCEFigure 3: Key themes of pain points heardPrevention, LTFU(initiation & earlytreatment)Marketing, counseling,treatment (regime,appointment schedule)Prevention (PrEP), linkage& early treatment,decentralized pickupsLinkage, treatment (prev.history, across districts,etc.), differentiatedmodelsSupply chainmanagement, treatment(in-facility experience)4.1.2 Tailoring4.1.3 TouchpointsTailoring refers to personalizing interventions to reachthose at risk, or PLHIV, in the best and most effective waypossible. A recurring theme from
Boston Consulting Group (BCG) is a global management consulting firm and a leading advisor on business strategy. BCG works with organizations in the social, public, and private sectors to deliver solutions to the most complex problems in contemporary society. Launched in 2003, the U.