Transcription
Regional Local Health NetworksProtocol (Clinical)Title: Diabetic Ketoacidosis Management in Adults withType 1 DiabetesProtocol author: Diabetes Service, Rural Support ServiceProtocol sponsor: Drug & Therapeutics Advisor CommitteeApproved by: Drug & Therapeutics Advisory Committee on: 13/12/2019Next review due: 13/06/2021SummaryThis protocol outlines responsibilities and actions requiredby medical staff, nurses and midwives to ensure the safetyand quality of patient care.Policy/ProcedurereferenceThis protocol supports the SA Health Recognising andResponding to Clinical Deterioration Policy Directive andGuideline, Diabetes Service Plan and Diabetes InpatientModel of Care.KeywordsClinical, Protocol, medical, nursing, midwifery, emergency,safety, quality, standards.Document historyIs this a new LHN Protocol? NDoes this protocol amend or update an existing protocol? YDiabetic Ketoacidosis Management in Adults with Type 1Diabetes, 2019Does this protocol replace an existing protocol? NApplies toThis protocol applies to all hospital medical, nursing andmidwifery staff.2020-02587Objective File No.Version control and change 12/2019AmendmentOriginal versionNew TemplateReviewed with no changesAmended by:Jane GilesJane GilesJane Giles Department of Health, Government of South Australia. All rights reserved.Publication of this document in the Policy and Procedure Library confirms that this is a valid, endorsed documentInformal copy when printed or downloaded – check CHSALHN Hub for most current versionFor Official Use Only – I2 – A1Page 1 of 14
1. Attached DocumentsDocument NameIntravenous Actrapid Infusion DKA / TYPE 1 Protocol & Chart – Adult (MR-INF-A)Intravenous Actrapid Infusion HHS / TYPE 2 Protocol & Chart – Adult (MR-INF-B)Intravenous Insulin Infusion (MR-INF-A) & (MR-INF-B) - Clinical Support Guide2. ReferencesDocument NameNorthern Adelaide Local Health Network (2019) Protocol for The Management of DiabeticKetoacidosis in Adults. Northern Adelaide Local Health Network, Adelaide.Joint British Diabetes Societies Inpatient Care Group (2010) The Management of DiabeticKetoacidosis in Adults. March. National Health Service Diabetes, United Kingdom.Country Health SA Local Health Network (2015) Procedure for the use of intravenouspotassium chloride. CHSA LHN, Adelaide.3. Accreditation StandardsNational Safety and Quality Health Service Standards (NSQHSS)12345678910 Governancefor Safety andQuality inHealthcarePartneringwithConsumersPreventing onSafetyPatientIdentification &ProcedureMatchngClinicalHandoverBlood & BloodProductsPreventing & Recognising & PreventingManagingResponding to Falls & HarmPressurefrom FallsClinicalInjuriesDeteriorationEvaluation and Quality Improvement Program (EQuIP)1112131415 ServiceDeliveryProvision ofCareWorkforcePlanning andManagementInformationManagementCorporateSystems andSafety4. ConsultationVersionConsultation1.0Northern Adelaide Local Health Network, Diabetes and Endocrine ServiceCHSA Diabetes Specialist Nurse Network2.0Northern Adelaide Local Health Network, Diabetes and Endocrine ServiceCHSA Diabetes Specialist Nurse Network3.0Northern Adelaide Local Health Network, Diabetes and Endocrine ServiceRegional Diabetes Specialist Nurse NetworkPublication of this document in the Policy and Procedure Library confirms that this is a valid, endorsed documentInformal copy when printed or downloaded – check SharePoint for most current versionFor Official Use Only-I2-A1Page 2 of 14
Table of contentspageFlow Chart: Diabetic Ketoacidosis4Diabetic Ketoacidosis: Introduction5Assessment of severity6Goal of treatment6Principles7Nursing considerations7Treatment planPart A. Within first hour – Immediate management8Part B. 1 – 6 hours10Part C. 6 – 12 hours11Part D. 12 – 24 hours12After care12Appendix 1 – Intravenous Actrapid Infusion DKA/Type 1 Protocol - Adult13Notes page14AcknowledgementsDr Anthony ZimmermannHead of Diabetes and Endocrine Services, Northern Adelaide Local HealthNetworkA/Prof Peak Mann MahEndocrinologist and General Physician, Northern Adelaide Local HealthNetworkDr Parind VoraEndocrinologist and General Physician, Northern Adelaide Local HealthNetworkJane GilesAdvanced Nurse Consultant, Diabetes Service, Rural Support ServiceCollette HooperNurse Practitioner Diabetes, Diabetes Service, Rural Support Service2016 Development team past memberDr David JesudasonDirector of Endocrinology, Country Health SA Local Health NetworkRegional Local Health Networks do not accept any responsibility for the use of this material outside the scope forwhich it has been designed. This information is not intended to replace professional judgement or experience.Publication of this document in the Policy and Procedure Library confirms that this is a valid, endorsed documentInformal copy when printed or downloaded – check SharePoint for most current versionFor Official Use Only-I2-A1Page 3 of 14
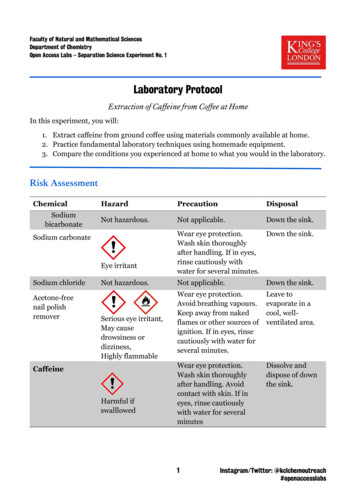
Diabetes Ketoacidosis Protocol in Adults with Type 1 DiabetesEarly consultation with appropriate regional or metropolitan hospital or MedStarDO NOT USE FORHYPERGLYCAEMICHYPEROSMOLAR STATEManagement of DKA – Consult with emergency physician/endocrinologistIV fluids and IV Actrapid Infusion DKA / Type 1 Protocol - AdultYesUp-transfer to anappropriate regional ormetropolitan hospitalSevereNoPart A - 0-60 minutesInitial investigations – vitals, 2 x IV cannula, urgent pathology (VBG, UEC, Osmolality, FBE, LFT,plasma glucose, capillary blood ketones, blood culture, ECG, CXR, urinalysis, CRP)IV fluidsIV insulinIV 0.9% sodium chloride1000ml/hourCommence IVActrapid Infusion DKA/ Type 1 Protocol AdultIV 0.9% sodium chloridePart B - 60 minutesBagno.2Time h613-19166ml/hMonitor blood glucose,bicarbonate, ketonesPotassium replacementCommence daily longacting insulin analogue(eg Lantus) at 2100hrsCommence potassiumreplacement as separateIV infusionSerum Potassium(mmol/L) 5.53.5-5.5 3.5Serum glucose 15.0 mmol/LOption 1 – change IV fluids to4% dextrose 0.18% sodiumchloride OROption 2 - commence 10%dextrose at 125 ml/hr ANDcontinue 0.9% sodium chloridesolutionPotassium replacementNilUp to 30 mmol consultation with emergencyphysician/endocrinologist.Transfer to a suitably equippedand staffed HDU or ED (mayrequire 10mmol/hr) Standard premixed potassium chloride solution, 10mmolpotassium chloride in 100ml mini bags are the preferred optionfor replacement on general ward.Cardiac monitoring if potassium replacement 10 mmol/hr(see p. 9)Check potassium before each bag of normal saline andreplace as aboveOnly use in conjunction withDKA clinical protocol guidePublication of this document in the Policy and Procedure Library confirms that this is a valid, endorsed documentInformal copy when printed or downloaded – check SharePoint for most current versionFor Official Use Only-I2-A1Page 4 of 14
Diabetic Ketoacidosis in Adults: IntroductionDiabetic Ketoacidosis (DKA) is a life-threatening complication of type 1 diabetes mellitusand needs to be treated as a medical emergency. DKA is associated with a significantmorbidity and mortality and must be diagnosed promptly and managed intensively. DKA is acomplex disordered metabolic state characterised by ketonaemia, hyperglycaemia and metabolicacidosis. This results from absolute or relative insulin deficiency accompanied by an increase incounter-regulatory hormones (glucagon, epinephrine, cortisol, growth hormone). In addition to thesignificant metabolic and electrolyte derangements, patients may have additional medical orsurgical co-morbidities, which may have triggered DKA such as sepsis, which must be diagnosedand appropriately managed. The clinical presentation of DKA may represent a new diagnosis oftype 1 diabetes or inadequate insulin in the patient known to have type 1 diabetes.Consultation with appropriate regional / metropolitan hospital / MedStar is requiredAt any point, if patient deteriorates, subsequent consultation is advised.Severe cases will mandate retrieval to appropriate regional or metropolitan hospital. Less severe cases may beable to be managed at larger country hospitals.Paediatric patients, treatment of DKA and intravenous fluid resuscitation requires a paediatrician.The following criteria must be met for local management;1) Availability of medical staff who are competent in managing thisdisorder and who can attend in person to review patient (atshort notice).2) Availability of nursing staff competent and confident inmanaging acute medical emergencies and who can provide 1:1or 1:2 nursing care.3) Availability of point of care testing.YesNo Each service to self-assess their capacity to manage this condition based on knowledge of their staff availability,qualification, experience and competency.The focus of management of DKA is on restoring hydration, clearing ketones, correcting electrolyte lossesand normalising blood glucose level.DEFINITION AND DIAGNOSIS OF DKATriad of1. Blood ketones 3.0 mmol/L or urine ketones 2 on dipsticks2. Blood glucose 11.0 mmol/L or known diabetes mellitus3. Bicarbonate (HCO3-) 15 mmol/L and/or venous pH 7.3Publication of this document in the Policy and Procedure Library confirms that this is a valid, endorsed documentInformal copy when printed or downloaded – check SharePoint for most current versionFor Official Use Only-I2-A1Page 5 of 14
Assessment of severityRecommend up transfer to an appropriate regional or metropolitan hospital HDU/ICU if oneor more of the following is present; Blood ketones 6.0 mmol/L Bicarbonate 5 mmol/L Venous/arterial pH 7.1 Hypokalaemia ( 3.5 mmol/L) Glasgow Coma Scale (GCS) 12 or abnormal AVPU scale* Oxygen saturation 92% on air (assuming normal baseline respiratory function) Systolic blood pressure 90 mmHg Pulse 100 or 60 bpm Urine output 0.5 ml/kg/hr Serum creatinine 200 μmol/L Microvascular event such as myocardial infarction or stroke Other serious co-morbidity – eg end stage kidney disease, heart failure orconditions that would warrant admission it HDU/ICU in their own right hypothermia elderly patient pregnant patient.*AVPU – Alert / Voice / Pain / UnresponsiveGoal of treatmentThe goals of treatment for DKA include; restoration of circulatory volume clearance of ketones correction of electrolyte losses (mainly potassium) normalisation of blood glucose.Other goals include prevention of: hypokalaemia hypoglycaemia other potential complications eg cerebral oedema arterial or venous thrombosis.Publication of this document in the Policy and Procedure Library confirms that this is a valid, endorsed documentInformal copy when printed or downloaded – check SharePoint for most current versionFor Official Use Only-I2-A1Page 6 of 14
PrinciplesThis protocol is designed to be followed in a sequential manner. use IV 0.9% sodium chloride solution (fluid of choice) as the principal fluid to restore circulating volume andreverse dehydration. use IV insulin infusion (Intravenous Actrapid Infusion DKA / Type 1 Protocol - Adult). (Actrapid is the insulin ofchoice for IV infusion) Do not use a priming dose (bolus) of insulin unless there is significant delay ( 1 hour) in setting up an insulininfusion monitoring of potassium level and replacement via IV fluid metabolic treatment targets reduction of blood ketone concentration by 0.5 mmol/L per hour increase venous bicarbonate by 3.0 mmol/L per hour reduce capillary blood glucose by 3.0 mmol/L per hour potassium should be maintained between 4.0 – 5.0 mmol/L subcutaneous long-acting analogue insulin SHOULD be continued bicarbonate administration is not recommended routinely phosphate should not be supplemented routinely.If patient not responding, consult with regional or metropolitan hospital and consider up transferNursing considerationsLevel of nursing care and frequency of observations will be determined by patient stability and treatment intensity, ega patient will need a 1:1 or 1:2 nursing ratio as hourly observations are needed and an insulin infusion is used.Observations include;1) capillary blood glucose ketone monitoring2) fluid balance record (catheterisation and hourly measures) calculate and report deficit or positive fluid balancehourly3) pulse oximetry4) pulse, respirations and blood pressure5) cardiac monitoring if hyperkalaemia or hypokalaemia (continue to cardiac monitor for patients requiring IVpotassium replacement)6) level of consciousness - Glasgow coma scale (GCS)7) Two (2) intravenous access lines are required. One for the insulin infusion, the other for hydration and potassiumreplacement as required. Potassium chloride replacement via additional port on the hydration line (eg piggyback).Must not run potassium infusion via the insulin line.a. An infusion pump or other rate limiting device must always be used for both an IV insulin infusion and IVpotassium chloride.b. Standard premixed potassium chloride solution, 10mmol potassium chloride in 100ml mini bags are thepreferred option for replacement. Premix 30mmol potassium chloride in 1 litre 0.9% sodium chloride alsoin stock for use if needed.Publication of this document in the Policy and Procedure Library confirms that this is a valid, endorsed documentInformal copy when printed or downloaded – check SharePoint for most current versionFor Official Use Only-I2-A1Page 7 of 14
Treatment Plan – Part AWithin first hour: Immediate management upon diagnosis: 0 to 60 minutes(continuous on-site medical supervision is necessary)Time 0 when intravenous fluids are commenced. If there is a problem with intravenous access, critical careadvice should be sort immediately. Consultation with an appropriate regional or metropolitan hospital orMedStar should be requested immediately.The aim within this time period is to:Further assess and decide if transfer of the patient is required or if the patient can be man
Availability of nursing staff competent and confident in managing acute medical emergencies and who can provide 1:1 or 1:2 nursing care. 3) Availability of point of care testing. Each service to self-assess their capacity to manage this condition basedon knowledge of their staff availability, qualification, experience and competency. The focus of management of DKA is on restoring hydration .