Transcription
The Patient Aligned Care Team and the2010 VA/DOD Diabetes Practice GuidelinesLen Pogach MD, MBA , FACPNational Director Endocrinology and DiabetesActing National Director, Medical Serviceon behalf of the VHA-DOD Diabetes Working Group11th Annual Advances in Indian HealthMay 4, 2011
DisclaimerThe opinions expressed in the followingpresentation are solely those of thepresenter, and do not represent those of anyagency or organization
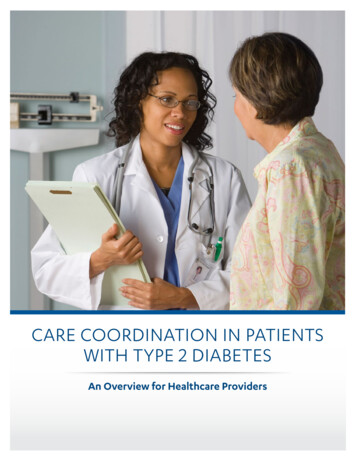
The Chronic Care ModelCommunityResources and PoliciesFamily Education &Self- iverySystemDesignHealth SystemHealth Care OrganizationDecisionSupportInformed,Activated PatientProductive activePractice TeamFunctional and Clinical OutcomesEd Wagner et al.
Evidence as the Basisfor Clinical Policy linesClinicalProcesses & SystemsClinicalRemindersadapted from J. Francis MD, MPHOQP
Objectives Provide a broader understanding aboutthe process of evidence development ingeneral and for the VHA-DOD Guideline Key points of the 2010 VHA DiabetesGuidelines– Glycemic Target Setting (Individualized usingAbsolute Risk Reduction approach)– A1c Laboratory Result Interpretation– Diagnosis of pre-diabetes and diabetes Implementation in the VHA PatientAligned Care Team (PACT)– Shared Decision Making– Provider Tools
Why is Evidence Critical for DiabetesManagement? Different Needs 26 million persons with DM; 11 MillionSeniorsDifferent populations:– 95% type 2, 5% type 1– Gestational DM– DM in pediatric populations– Younger, healthier adults– Healthier seniors– Major Co-morbid conditions—othermedical conditions, mental healthconditions, diabetes relatedcomplications: advanced, end stage
Veteran Population with DiabetesAbout one in four veterans ( 1.4 million)High Illness BurdenSF36v Low Physical Component Score 36.9– CVD 32.4%– HBP 66%– CKD 30%;Low Mental Component Score /45.1– Mental Health Disorders 25%-40%Even half of veterans less than 65 years of agehave decreased life expectancy or majorcomorbiditiesIn 1999,One in seven veterans reported food insufficiency31% did not complete high school
Key Concepts in Evidence BasedMedicine Strength of Evidence– Randomized clinical trials (including evaluation ofquality)– Observational Studies (including pooled data andepidemiological studies)– Meta-analyses– Expert Opinion Strength of Recommendation– Balancing benefits (absolute risk reduction) withrisk of harms– Generalizability
Clinical Randomized Trials Considered gold standard Factors to consider: design (randomized,masked; intention treat); population; primaryvs secondary endpoints, primary analysis,secondary analysis, post-hoc analysis Strengths: Discern effects of experimentalintervention versus control Weaknesses: homogeneous population;extrapolation from study population to clinicalpractice
Epidemiological Research Population studies; case cohort studies Strengths: Large and diverse populations,long time frames; multiple factors Weaknesses: selection biases; failure toidentify unspecified covariates; provessignificant association, not causality
How does VA/DOD developguidelines? Strict approach to conflicts of interestMultidisciplinary teamsIdentification of key questionsEvidence review for key questionsGroups review evidence, apply gradingDevelopment of text, treatmentalgorithmsReview from trained subject matterexpertsTransparency of strength of evidenceRevisions based on reviewFinal CPG reviewed by VA/DoD council
Attributes of VA-DOD Guidelines Evidence based: Transparent about the strength ofevidence and the strength of recommendation Use of numeracy : Emphasizes absolute riskreduction, number needed to treat rather thanrelative risk reduction Risk stratification: Classification of patients intolow, medium and high risk categories for eachmodule for case management and treatmentstrategies Flexibility: Provider makes recommendations basedevidence & clinical judgment and then incorporatespreferences of patient using shared decision makingto arrive at patient’s target goal
Comparison of Diabetes Guidelines Qaseem, Annals Int Med 2007;147:417-22. Process of development of VHA DOD Guidelines (2003) wasrated significantly higher than specialty professionalsocieties using GRADE VHA-DOD Guidelines promote understanding the evidence,and treating veterans based upon absolute benefit and risk,rather than relative risk reduction
Use of Evidence for VHA PolicyDecisions Life expectancy, co-morbid condition approach riskstratified management using shared decision firstproposed 1997, updated 2000, 2003, 2010. Every other year eye examinations for low riskpatients incorporated into DQIP-HEDIS (1998) VHA did not implement NCQA 7% A1c and 130mmHg measures for accountability (2007) ―Tight‖ glucose control in ICUs not mandated (ESP2007) SMBG recommendations reaffirmed (ESP 2006) PBM Criteria for Use antedated ―ADA ConsensusRecommendations‖ Rosiglitazone removed from formulary (2007 PBMSafety Study)
Population-based Healthcare is acritical part of PACT Encompasses the ability to:– Identify & assess high risk states within the targetpopulation Health/clinical Behavioral Socio-demographic Genomic Preference– Implement and evaluate interventions that aredesigned to improve the health of that populationthat are– Consistent with the community’s cultural, policyand health resource values
(Non-)Integration of Research andClinical Practice Long lag time betweendevelopment ofscientific knowledgeand introduction intopractice–Antmann et al. Comparison of results of metaanalyses of randomized control trials andrecommendations of clinical experts. JAMA1992;268:240-8. There is also a longtime betweenintroduction and broadimplementation.
Where does the evidence fit in and howcan it get there?Primary reVA/DOD Guidelines ModelRegistriesDecision SupportServiceAgreementSpecialtyCareFace to Face orVirtual Consults 10%Not managedin PCSpecialtyCareLeadershipGordon Schechtman, MDActing Chief Consultant, Primary Care, PCS
What do the 2010 VA-DODDiabetes Guidelines sayabout Diagnosis of Pre-Diabetes andDiabetes Self Monitoring of Blood Glucose A1c targets Estimated Average Blood Glucose
Diagnosis of Pre-Diabetesand Diabetes
Diagnosis of Pre-DiabetesA diagnosis of pre-diabetes is made witheither of the following: Fasting plasma glucose (FPG) 126 mg/dLbut 100mg/dL on two occasions. A1c readings with result 5.7% but 6.5%and confirmed with a FPG 100 mg/dLand 126 mg/dl.– The FPG can be obtained at the same time asthe A1c
Diagnosis of DiabetesA diagnosis of DM is made with any of thefollowing: A1c 7% on two occasions using a clinicallaboratory methodology standardized tothe NSGP (not Point of Care testing A1c 6.5%, confirmed with a FPG 126mg/dL. These tests can be done on thesame or different days; or FPG 126 mg/dL on at least two occasions Random blood glucose not recommendedfor screening
Self Monitoring ofBlood Glucose
Self Monitoring ofBlood Glucose SMBG is indicated for patients taking insulin No evidence for routine SMBG in patientsnot on insulin Patients must be instructed on procedures,importance of recording, and how tointerpret results SMBG can be used to adjust treatment Frequency of testing based on type oftreatment, hypoglycemia, goals of treatment SMBG is not recommended for pre-diabetes
A1c Targets and SharedDecision-Making
A1c Targets: Risk Stratification A1c target 7%, if achievable without risk– Mild or no microvascular complications, no majorconcurrent illnesses and with reasonable lifeexpectancy ( 10-15 years) A1c target 8% Longer duration diabetes ( 10 years) or with co-morbiditiesand requiring combination medication regimens includinginsulin A1c target 8-9%– Patients with advanced microvascularcomplications and/or major comorbidities or lifeexpectancy 5 years are unlikely to benefit fromaggressive glucose lowering
Risk of Progression ofComplications by A1c*Relative risk set to 1 for HbA1c of 6%.
Risk of Retinopathy Progressionby HbA1c and Years of Follow-upDCCT Research Group. Diabetes 1995;44:968-983.
Benefits of Glycemic Risk Reduction (7.9% to7.0%) over 10 yrs from the UKPDS(Budenholzer et al, BMJ 1245, 2001)OutcomeOR(95%CI)PNNT PerPYARR/1000PYRate per 1000PY - IntensiveControlAny 233.17.911.0DiabetesMortality0.90NS-------10.411.5
Glucose Control and CVDOutcomesStudyAcronymParticipants Follow- IntensiveupA1c(years)TargetStandardA1cTarget 6.0%7.0%-7.9%Achieved .5 6.5%Usual careNoAchieved Achieved difference6.4%7.0%VADT17005-7 intensivegroupDifferencenotsignificant
Outpatient RCT Diabetes TrialsUnited KingdomProspectiveDiabetes Study11 yearsAccordAdvanceVADT3.5 years5 years5.6 years7.0%6.4%6.4%6.9%7.9%7.5%7.0%8.5%Intensive Rx0.71*4.6*0.56*12.0*Standard utcomeDuration of studyHbA1c achievedIntensive RxStandard RxSevere hypoglycemia All-cause MortalityIntensiveStandardCardiovascular MortalityThanks to Dr. Farmaz-Ishmael Beigi ACCORD Coordinator for this slide.
Hypoglycemia Among Veterans: ObservationalData (Miller et al, QUERI 2010) From 2000-2004, ICD-9 codes for hypoglycemia iscommon in diabetes patients. 10% with an eventeach year (VA and CMS data) The strongest predictors are indictors of labile orbrittle diabetes: prior hypoglycemia, keto-acidosis,hyperosmolar coma, and high HbA1C; insulin orsecretagogue use. Strongly associated with recent insulininitiation or recent hospital stay, particularlyfor infection. Related to disability, poverty, being without aspouse or partner
A1C & Cr, On Insulin, Age 65
Should Clinicians be Made Aware ofVariability in A1c Measurement? Not a new concept Discussed at NGSP meetings since 2006 NGSP minutes note comments by some NGSPmembers that doctors likely think that thetest results are “accurate” because they are“standardized” Concerns by some NGSP members that thebroad range of accuracy and precision amongmethods is not acceptable
Sources of Error – A1c testingAssay Methodology Technician Within-observer Between-observers Instrument Within-instrument Between-instruments Between laboratories Artifact
ACCURACY AND PRECISION TARGET MOTIFONE WAY TO LOOK AT ACCURACY AND PRECISION IS TOVISUALIZE WHAT THEY MEAN. FOR EXAMPLE:RELIABLEINACCURATEMost of the measurements lieclose to each other and theirmean value lies close to theBull’s Eye – reference value.This provides a reliable resultwithout having to makeadjustments.Most of the measurements lieclose to each other but theirmean value lies far from theBull’s Eye – reference value.Recalibrating to the referencestandard provides moreaccuracy.High AccuracyHigh PrecisionLow AccuracyHigh PrecisionINPRECISEUNRELIABLEMost of the measurements liefar from each other but theirmean value lies close to theBull’s Eye – reference value.Making more measurementswill increase precision but isnot feasible in patient test.Most of the measurements liefar from each other and theirmean value lies far from theBull’s Eye – reference value.There is no easy way toobtain a reliable result fromthis system.High AccuracyLow PrecisionLow AccuracyLow Precision
Sources of Error – A1c testingMarch 11, 2011 DMICC Meeting– The critical difference (CD) is the change in apatient’s serial test results that can be consideredsignificantly different (e.g. at a probability of 95%).– 0.5% is a difference that many physicians use as asignificant difference in their patients’ HbA1c results.– In order for a 0.5% HbA1c change to be consideredsignificant the assay CV must be 3%, ideally 2%.Many, but not all, individual assay methods can meetthis criterion.– Point of Care test performance is unknown andshould not be used for treatment decisions
Table 1: Estimated Average GlucoseHbA1c n Interval)(76, 120)(100, 152)(123, 185)(147, 217)(170, 249)(193, 282)(217, 314)DM Nathan et al. Diabetes Care. 31: 1473-8 2008
The A1c-Derived Average Glucose StudyHbA1c (study end) vs AG (over 3 months)Avg Glucose (3 months)How much is measurement variation?How much is biological variation?How much is glucose sampling timevariation?2005.97.5130357R2 0.84, P 0.0001911HbA1c (%; study end)DM Nathan et al. Diabetes Care. 31: 1473-8 20081315
Avg Glucose (3 months)Your Next Patient with HbA1c 6.5out of all of your patients:measurement variation?vs. biological variation?vs. time integration variation?3579DM Nathan et al. Diabetes Care. 31: 1473-8 200811
Patient Safety Concerns Generalization to individuals with multiplecomplex conditions who would have beenexcluded from studies Multiple medications in persons with co-existingillness No monitoring system for hypoglycemia A1c of 7 can represent range of 6.5 to 7.5% inpractice in commercial laboratories:– Is an all or none threshold be used to intensifytherapy, especially for insulin?– Should we disregard SMBG results?
Returning to the VeteranPatient – Centered Care: Explores patients’ reason for visit,concerns, and need for information Seeks an integrated understanding of thepatients’ world – life issues, emotionalneeds Finds common ground on the problem(s)and mutually agrees on management Enhances prevention and health promotion Enhances the continuing relationship withthe doctor
Patient Aligned Care mprovement Robert Petzel, MDVHA USHMarch 25, 2010Where Should We Go?TeamCare43
Glycemic Management is a perfectexample to illustrate these issues. Patient centered –– Shared decision making is an important aspect of carebecause nothing is simple anymore – tradeoffs betweenrisks and benefits, other conditions, J L Jordan,S J Ellis,R ChambersDefining shareddecision makingand concordance:are they one and thesame? PostgradMed J 2002;78:383384
Productive Interactions & SharedDecision Making Involves presentation-in an understandablemanner—the benefits and risks of theintervention individualized for the veteran andfamily. Requires that the veteran has skills of literacyand numeracy to understand the issues and askappropriate questions Requires that the clinician has communicationskills and takes into account cultural issues Final decision incorporates patient preferences Target ranges may better incorporatelaboratory variability and the continuousnature of risk factor reduction
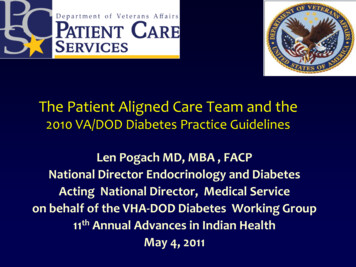
Stratified A1c TargetsMAJOR COMORBIDITYCardiovascular disease,severe chronic kidneydisease, severe chronicobstructive lung disease,severe chronic liver disease,recent stroke, and lifethreatening malignancyABSENTPRESENT(not end-stage andMICROVASCULAR COMPLICATIONABSENT ORMILDearly backgroundretinopathy, microalbuminuria, mild hy, orpersistent macroalbuminuria sensory loss.severe non-proliferative orproliferative retinopathy /serum creat 2.0 mg/dL insensate extremities orautonomic neuropathy 7%7-8%8-9%7-8%7-8%8-9%8-9%8-9%8-9%management achievable )MARKEDeither end-stage ormanagement is significantlychallenging
For new onset diabetes, if A1clevels are targeted to be around 7% for the first 10 years82 alive with diabetes withoutmicrovascular disease 8 alive withdiabetes and microvascular disease10 dead from diabetesFor new onsetdiabetes, if A1clevels aretargeted to be around 8% for the first 10 years78 alive withdiabetes without microvascular disease11 dead fromdiabetes Person alive with diabetes andno microvascular complications Person alive with diabetes andwith microvascularcomplications Person dead from diabetes 11 alive withdiabetes andmicro-vasculardiseaseThe United Kingdom Prospective Study(UKPDS), conducted from the mid-1980s tolate 1990s with patients whose average A1cwas 9% at time of diagnosis, provides theprimary evidence base for tight control oftype 2 diabetes from onset of disease forindividuals with a life expectancy of around10 years - UKPDS 33 (sulfonylurea/insulintherapy compared to conventional therapy –Lancet 1998); Use of metformin may conferadditional benefit; UKPDS 34 (metformin vs.conventional therapy Lancet 1988). Microvascular complicationsinclude retinopathy,nephropathy, and neuropathy
ACCEPTABLE RISKWE CAN NEVER COMPLETELY ELIMINATE RISKWhen making a decision on how we use HgbA1c we need to determine if the overallbenefits out balance the potential risk for an adverse outcome.RISKBENEFITWHAT KIND OF RISK ARE WE FACING WITH DIABETES?Navigating a narrow path between two difficult clinical courses: Increased morbidity and mortality due to under treatmentVersus Risks associated with hypoglycemia due to over treatment.Therefore, it is critical that you know as much as possible about the risks associatedwith your clinical decisions and this means:KNOWING THE EXTENT OF LABORATORY ERROR AT YOUR FACILITY
A Value of A1c of 7.4% could be anything between 6.9and 7.9 in a assay with an overall error acceptable forclinical use (overall error 7%). If the assay has anoverall error of 3%, the range is narrower (7.2-7.6).Lab Report7.6 7.9 8.0Says:7.27.4%7.09.06.96.010.0
RECOMMENDATIONS – REPORTING HGBA1CBelow is a consensus recommendation for the reporting of HgbA1c test resultsincluding a 95% confidence interval to show intralaboratory precision as well as theconfidence interval adjusted for the laboratory’s accuracy against the NGSPreference standard through CAP proficiency testing.TESTHgbA1cRESULT6.5%PRECISION – 95% CI6.3 – 6.7%ACCURACY ADJUSTED 95% CI *6.57 – 6.97 *Confidence interval adjusted for bias of this facility's methodology whencompared to the National Glycated Hemoglobin Standardization Program referencestandard through CAP Proficiency Testing. Our ability to deliver this type of report format and content in the VA will depend onthe capacity of the VistA and CPRS system to do this so we may have to institutethe following alternate report:TESTHgbA1cRESULT6.5%95% CONFIDENCE INTERVAL /- 0.2%CI ADJUSTED FOR OUR METHOD* an additional 0.27%
What is evidence-basedmedicine? Where there is evidence of benefit andvalue, do it Where there is evidence of no benefit,harm, or poor value, don’t do it. When there is insufficient evidence toknow for sure, be conservativeDavid Eddy MD
In the end, it is about the Patient'sjourneyNon diabetesadmissionsPREVENTION85% of careInitial ContinuingDiagnosisManagement Carenewcomplicationsheartdiseaselife eventsstroketreatmentchange eginsulinEDEVENTSPregnancySevere blemsFootissues
Federal Practitioner April 2011Leonard Pogach, MD, MBA; Paul R. Conlin, MD;Curtis Hobbs, MD; Robert A. Vigersky, MD; andDavid Aron, MD, MS; for the VA-DoD DiabetesGuideline Working GroupVA-DoD Update of Diabetes Guidelines:What Clinicians Need to Know AboutAbsolute Risk of Benefits and Harms and A1cLaboratory Accuracy
ResourcesVA DoD Diabetes Practice Guidelineshttp://www.healthquality.va.gov/Diabetes Mellitus.aspDiabetes: Reports.htm
Objectives Provide a broader understanding about the process of evidence development in general and for the VHA-DOD Guideline Key points of the 2010 VHA Diabetes Guidelines –Glycemic Target Setting (Individualized using Absolute Risk Reduction approach) –A1c Laboratory Result Interpretation –Diagnosis of pre-diabetes