Transcription
University of South FloridaScholar CommonsGraduate Theses and DissertationsGraduate School8-31-2010Design of a New Suturing and Knot Tying Devicefor Laparoscopic SurgerySinan OnalUniversity of South FloridaFollow this and additional works at: http://scholarcommons.usf.edu/etdPart of the American Studies Commons, Industrial Engineering Commons, OtherEnvironmental Sciences Commons, and the Sustainability CommonsScholar Commons CitationOnal, Sinan, "Design of a New Suturing and Knot Tying Device for Laparoscopic Surgery" (2010). Graduate Theses and 98This Thesis is brought to you for free and open access by the Graduate School at Scholar Commons. It has been accepted for inclusion in GraduateTheses and Dissertations by an authorized administrator of Scholar Commons. For more information, please contact scholarcommons@usf.edu.
Design of a New Suturing and Knot Tying Device for Laparoscopic SurgerybySinan OnalA thesis submitted in partial fulfillmentof the requirements for the degree ofMaster of Science in Engineering ManagementDepartment of Industrial and Management Systems EngineeringCollege of EngineeringUniversity of South FloridaMajor Professor: Susana Lai-Yuen, Ph.D.Stuart Hart, M.D.Patricia Zarate, Ph.D.Date of Approval:June 30, 2010Keywords: suturing device, laparoscopy, hysterectomy, medical device design, prototypeCopyright 2010, Sinan Onal
AcknowledgmentsI would like to express my heartfelt gratitude to my advisor, Dr. Susana Lai-Yuenfor her supervision, and guidance from the very early stages of this research. She hasalways provided me constant encouragement and support in various ways in my journeyof growing into the researcher and scientist that I want to be. I am indebted to her morethan she knows. My sincere thanks also go to Dr. Stuart Hart for his advice and crucialcontribution to this study, which made him a backbone of this research. His involvementwith his expertise in this area has triggered and nourished mine. Above all, this thesiswould have not been possible, had he not given me the opportunity to observe hisoperations. Likewise, Dr. Patricia Zarate deserves special thanks as another member ofmy committee. Her being accessible and approachable as well as her instant supportwhen I am in need have helped me experience a smoother and more fruitful processthroughout this study. I would also acknowledge my friends Issa Ramirez, GokmenDemirkaya, Ricardo Vasquez Padilla and Humberto Gomez for their willingness to sharetheir ideas with me. Last but not least, words fail me to express my appreciation to mywife Derya whose unconditional love and support, and persistent confidence in me, hastaken the load off my shoulder, and to my one-and-only daughter, Pera, the reason of mylife, for simply cheering it up and making it more meaningful with her presence everypassing day. I would not be here today without them and their love.
Table of ContentsList of Tables. iiiList of Figures . ivAbstract .viiChapter 1: Introduction . 11.1 Motivation. 11.2 Thesis Objectives and Contributions. 51.3 Thesis Outline . 6Chapter 2: Literature Review . 72.1 Conventional Laparoscopic Suturing and Knot Tying Process . 72.2 Commercially Available Suturing Devices . 122.2.1 Endo Stitch 10 mm Suturing Device . 122.2.2 Capio Open Access and Standard Suture Capturing Device . 14Chapter 3: Case Study on Conventional Suturing Process . 183.1 Human Factors Engineering . 183.2 Introduction to Case Study . 193.3 Laparoscopic Instruments Used for Suturing and Knot Tying . 193.4 Task Analysis . 213.5 Failure Mode and Effect Analysis (FMEA) . 25Chapter 4: Design Process of the Proposed Laparoscopic Suturing Device . 294.1 Definition of Medical Device and Design Process . 294.2 Analysis Stage. 314.2.1 Analysis of the Problem . 324.2.2 Product Design Specifications . 334.3 Synthesis Stage . 364.3.1 Developing Alternative Solutions. 364.3.2 Choosing a Solution . 384.4 Evaluation Stage . 404.4.1 Modeling and Engineering Analysis. 414.4.2 Prototyping and Evaluating . 58Chapter 5: Research Summary and Future Work. 65i
5.1 Research Summary. 655.2 Future Research Work . 66References . 67ii
List of TablesTable 3.1:Task analysis for conventional suturing process . 22Table 3.2:Failure mode and effect analysis for conventional suturing process. 26Table 3.3:Severity ranking criteria . 28Table 3.4:Probability ranking criteria . 28Table 4.1:Product design specifications . 35Table 4.2:Pugh chart . 40Table 4.3:Types of material . 44iii
List of FiguresFigure 1.1:Minimally invasive surgery [drawing] . 2Figure 1.2:2D monitoring during minimally invasive surgery [drawing] . 2Figure 1.3:12-mm laparoscopic port [photograph] . 4Figure 2.1:Curved needle with surgical suture [photograph] . 8Figure 2.2:Laparoscopic needle driver [photograph] . 8Figure 2.3:Maryland grasper [photograph]. 8Figure 2.4:Extra-corporeal knot tying technique . 9Figure 2.5:Knot pusher [photograph] . 9Figure 2.6:Half- hitches knot techniques . 10Figure 2.7:Compound sliding knots . 11Figure 2.8:Intra-corporeal suturing and intra-corporeal knot-tying technique . 12Figure 2.9:Endo Stitch 10 mm suturing device [photograph] . 13Figure 2.10:Knot tying technique with Endo Stitch . 14Figure 2.11:Capio suture capturing device [drawing] . 15Figure 2.12:Partial schematic perspective views of distal portion of Capio [drawing] . 16Figure 2.13:Transvaginal and paravaginal defect repair using the Capio . 17Figure 3.1:Instruments used for conventional laparoscopic suturing and knottying . 20Figure 4.1:Product development process. 30iv
Figure 4.2:Product development process for the proposed device . 31Figure 4.3:Sub-steps of the analysis stage . 31Figure 4.4:Sub-steps of the synthesis stage . 36Figure 4.5:Alternative design 1 . 37Figure 4.6:Alternative design 2 . 37Figure 4.7:Alternative design 3 . 38Figure 4.8:Alternative design 4 . 38Figure 4.9:Alternative design 5 . 38Figure 4.10:Design decision factors . 39Figure 4.11:Sub-steps of the evaluation stage . 41Figure 4.12:3D CAD model of the proposed device . 42Figure 4.13:Mechanism for needle transporting of the proposed device . 43Figure 4.14:Arms at the tip of the proposed device . 46Figure 4.15:FEA results of stress distribution in the arms of the device . 47Figure 4.16:Displacement distribution in the arms and deformed shape of thearms . 48Figure 4.17:The flexible wire to control the needle carriers . 49Figure 4.18:Small plunger . 49Figure 4.19:Main plunger . 49Figure 4.20:Relationship between the main plunger and small plunger . 50Figure 4.21:Detailed view of the mechanism for changing the needle direction . 51Figure 4.22:Stress distribution on the small plunger and deformed shape of thepart . 53Figure 4.23:Displacement distribution on the arms of the small plunger . 53v
Figure 4.24:Stress distribution on the main plunger and deformed shape of thepart . 54Figure 4.25:Displacement distribution on the arms of the small plunger . 55Figure 4.26:Needle and needle carrier . 56Figure 4.27:Needle holder . 56Figure 4.28:Stress distribution on the needle holder . 57Figure 4.29:Fused deposition modeling (FDM) machine, Dimension SST-768 . 58Figure 4.30:Prototypes of the first version of the handle . 59Figure 4.31:Prototype of the final version of the handle . 60Figure 4.32:Prototype of the first version of the arms . 61Figure 4.33:Prototype of the final version of the arms. 61Figure 4.34:Prototype of the final version of the arms-assembled . 62Figure 4.35:Prototype of the final version of the toggle lever . 63Figure 4.36:Prototype of the main plunger and small plunger . 63Figure 4.37:Prototype of the main plunger and small plunger-assembled . 63Figure 4.38:Prototype of the final flexible wire. 64Figure 4.39:Prototype of the final version of the proposed device . 64vi
Design of a New Suturing and Knot Tying Device for Laparoscopic SurgerySinan OnalAbstractMinimally invasive or laparoscopic surgery has completely changed the focus ofsurgery becoming an alternative to various types of open surgery. Minimally invasivesurgery avoids invasive open surgery as the operation is performed through one or moresmall incisions in the abdomen and using a small camera called laparoscope. Throughthese incisions, surgeons insert specialized surgical instruments to perform the operationresulting in less postoperative pain, shorter hospital stay, and faster recovery. However,the main problems during minimally-invasive surgery are the limited space for operatinginstruments and the reduced visibility and range of motion inside the patient’s body.During minimally-invasive surgery, one of the most difficult and time consumingsurgical procedures is suturing and knot tying. This procedure significantly increases theoperation time as it requires advanced techniques and extensive experience by surgeons.The main goal of this research is to investigate, design, and develop a new suturinginstrument to facilitate suturing procedures during minimally invasive surgery.Qualitative research data was collected through interviews with a surgeon and six indepth observations of minimally invasive surgeries at Tampa General Hospital. Differentdesign concepts and mechanisms were created using SolidWorks CAD software, andtested using SimulationXpress in order to identify dimensions, materials and expectedvii
performance of the design and its components. The prototypes of the device were madeusing a Dimension SST 768 FDM machine and tested by the surgeon to ensure that thefinal design meets the specified needs and criteria. This new device will eliminate the useof many different devices during the operation and allow the use of any type of suture.The proposed suturing device aims to benefit both patients and surgeons. For surgeons,the new device aims to decrease the number of steps for laparoscopic suturing through anintuitive and ergonomic design. For patients, the proposed device will reduce time duringsurgery and under general anesthesia leading towards improved health care.viii
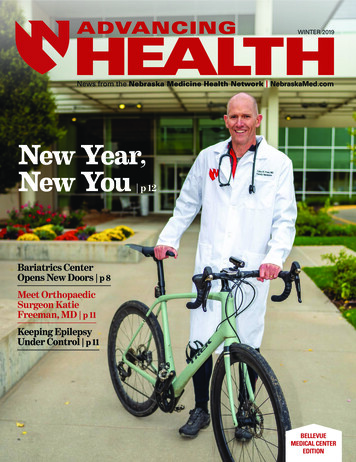
Chapter 1IntroductionThis chapter introduces the motivation underneath this research work and thecurrent challenges in minimally-invasive surgical procedures. The research objectives arepresented followed by the thesis outline.1.1MotivationMinimally invasive surgery (MIS) or laparoscopic surgery has changed the focusof surgery becoming an alternative to various types of open surgery. Minimally invasivesurgery is a new surgery technique that avoids invasive open surgery by operatingthrough small incisions in the abdomen and using a small camera called laparoscope asshown in Figure 1.1. The small incisions measure about 6.5 – 12.7 mm in size comparedto the minimum incision size of 20 cm required for traditional open surgery techniques("Minimally invasive", 2010). Through these incisions, surgeons insert specializedsurgical instruments to perform the operation while observing the working space througha video monitor as shown in Figure 1.2. For this reason, minimally invasive surgeryresults in less tissue trauma, less scarring, and faster post-operative recovery time.1
Figure 1.1: Minimally invasive surgery [drawing]. Retrieved January 10, 2010 fromwww.rfay.com.au/laparoscopicFigure 1.2: 2D monitoring during minimally invasive surgery [drawing]. RetrievedJanuary 10 from www.rfay.com.au/laparoscopicAccording to the U.S. Department of Health and Human Services, it is estimatedthat in 2008 there were around 220,000 gastric bypass procedures and more than 250,0002
appendectomies performed in the United States. Also, about 50,000 patients in the UnitedStates are diagnosed each year with liver metastases that require a liver resectionprocedure. Furthermore, hysterectomies are the second most common surgery performedamong women in the United States, with over 600,000 operations carried out each yearand while up to 75% of hysterectomies are performed through open surgeries (Dunitz,Sheth, & Studd, 2002). The percentage of laparoscopic hysterectomies is increasing andwill greatly benefit from new improved instruments that facilitate this type of surgeryThere are several benefits of minimally invasive surgery over traditional methods.The most important benefit is that post-operative scars are much smaller than those thatoccur as a result of conventional "open" surgery thus resulting in less pain for the patient.Single-incision minimally invasive surgery leaves minimal scar because the surgery isperformed through a single incision in the belly button. Patients require less painmedication and recover faster, normally returning home within 24 hours after theirsurgery. This is a major advantage when compared with hospital stays of 2 to 5 days fromopen surgery patients.In recent years, minimally invasive surgery has developed in a way that it is nowbeing used to perform a variety of procedures such as gastric bypass, appendectomy, liverresection, hysterectomy, and more. Although minimally invasive surgery has becomeincreasingly popular, the problems pertaining to it, such as limited visibility, constrainedworking space, and the use of high-end technological tools, still complicate the surgery.Surgeons need to obtain extensive training to be qualified to perform minimally-invasivesurgeries and not all hospitals have the special equipment necessary to perform suchsurgeries. In addition, the design of medical tools for minimally-invasive surgery is3
constrained by the size of the ports used to insert the surgical instruments. These portsnormally have an opening of 5-12 mm in diameter where the surgical instruments areinserted to perform a laparoscopic surgery. Therefore, surgical tools need to be smallenough to fit through these ports making the design of these tools a challenge.Figure 1.3: 12-mm laparoscopic port [photograph]. Retrieved February 6, 2010from: age/3/During a laparoscopic surgery, suturing and knot tying are among the mostdifficult and most time consuming procedures. These procedures significantly increasethe operation time as they require advanced techniques and extensive experience bysurgeons due to the limited operating space and motion range (Pattaras, Smith, Landman,& Moore, 2001). The most common suturing approach is the conventional technique,which consists of using a curved needle and two needle drivers to perform the task.According to Adams et al., the time for each suturing placement through the conventionalmethod averages 151 24 seconds and each knot tying time of conventional technique ison average 197 70 seconds (Adams, Schulam, Moore, Partin, & Kavoussi, 1995). If weconsider that a surgeon has to knot six times on average, the duration of the operationincreases considerably due to suturing. Although suturing devices for minimally-invasive4
surgery are commercially available and currently being used, surgeons still indicate theneed for better devices that can facilitate the suturing and knot tying procedures duringminimally-invasive surgeries. The main limitations for designing devices for this type ofsurgery are the limited space and motion range, which greatly constraint the dimensionsand mechanisms of the device.1.2Thesis Objectives and ContributionsThe proposed research aims to address the main laparoscopic suturing challengesand current literature limitations in the market. The main goal of this research is toinvestigate, design, and develop a new medical device system for facilitating suturing andknot tying procedures during minimally-invasive surgery. The device will also enable theuse of any type of suture on the needle.The major objectives of this thesis are:1. To investigate and design a new suturing device to minimize the suturing risksand difficulties during minimally invasive surgery. This device aims to decreasethe suturing operating time while being intuitive for surgeons to use.2. To implement a physical prototype of the design to analyze and test theeffectiveness of the device.This research focuses on the suturing and knot tying procedures duringhysterectomies, which is the second most common surgery among women in the U.S.according to the U.S. Department of Health & Human Services. However, the proposedresearch can be applied to any minimally-invasive surgical procedure that requiressuturing and knot tying. The hysterectomy procedure consists of removing the women‟s5
uterus and sometimes the ovaries and fallopian tubes. Suturing and knot tying is requiredafter the uterus is removed from the patient.This new instrument aims to benefit both patients and surgeons. For surgeons, thenew device aims to minimize the suturing difficulties encountered during minimallyinvasive surgery. This is expected to help surgeons in performing suturing faster andsafer. For patients, the proposed device will reduce the surgery time thus reducing thetime under general anesthesia. At the same time, the proposed suturing device contributesto patient‟s safety that can lead to improved health care.1.3Thesis OutlineChapter 2 discusses current research work and available devices for suturing andknot tying during minimally-invasive surgery. Chapter 3 examines the conventionalsuturing device and knot tying technique commonly used in minimally-invasive surgerythrough a human factors approach. This examination provides recommendations for thedevice design. Chapter 4 describes a new surgical suturing device and its design stages.Each design stage is introduced to understand the logic behind the new instrument.Chapter 5 provides a summary of the research methodologies presented and futureresearch work.6
Chapter 2Literature ReviewThis chapter provides the background of current research work in the area andintroduces suturing devices currently used in minimally-invasive surgery. Current designsare analyzed and their limitations identified.2.1Conventional Laparoscopic Suturing and Knot Tying ProcessThe conventional suturing technique has been performed for many years and it isstill the most common suturing technique used by surgeons even though it has manydifficulties. It is performed by using a curved needle and two elongated needle drivers.The curved needle and needle drivers are inserted through the laparoscopic ports andsuturing placement is performed manually inside body. Many types of needles exist thatare specifically designed for conventional laparoscopic suturing. In previous years,straight needles were used for laparoscopic suturing as they were easier to introduce intothe abdominal cavity; however, it was difficult to control them while suturing (Sanfilippo& Solnik). Curved needles are currently used for suturing in minimally-invasive surgery,as shown in Figure 2.1. They have become very popular but need to be handled usingelongated laparoscopic needle drivers and Maryland Graspers as shown in Figures 2.2and 2.3, respectively. For this reason, the first problem with curved needles is that handson experiences using these instruments are needed. The second problem is that curved7
needles can be difficult to insert in the correct location as the abdominal wall preventsfree movement of the needle driver (Sanfilippo & Solnik).Figure 2.1: Curved needle with surgical suture [photograph]. Retrieved February 10,2010 from www.wikisurgery.comFigure 2.2: Laparoscopic needle driver [photograph]. Retrieved February 10, 2010 fromwww.kenzmedico.co.jpFigure 2.3: Maryland grasper [photograph]. Retrieved February 10, 2010 fromwww.stryker.com8
To facilitate the conventional suturing and knot tying technique, various types ofsuturing and knot tying approaches have been introduced in previous years. The oldesttechnique is intra-corporeal suturing and extra-corporeal knot tying technique as shownin Figure 2.4 (Liu, 1993). Extra-corporeal knot tying is a method to avoid the difficultand time-consuming skill of intra-corporeal knot tying. Two elongated laparoscopicneedle drivers and a curved needle are used to suture. On the other hand, knot is tiedoutside the body and then the loop is pushed into the operating area by a knot pusher asshown in Figure 2.5. This technique also requires high level skills.Figure 2.4: Extra-corporeal knot tying technique. (Liu, 1993)Figure 2.5: Knot pusher [photograph]. Retrieved February 15, 2010 fromwww.calicutsurgicals.com9
There are two categories of knot tying techniques that are used in extra-corporealtying: half-hitches and compound sliding knots. As shown Figure 2.6, the half-hitchesknot is the simplest of all sliding knots formed and the basis for a multitude of otherknots used. The half-hitches technique is described in the medical dictionary asconsisting of “ one straight strand with the other thrown over, back over itself, underthe original strand and back through the loop created by the earlier steps. It is the basisfor square, granny and surgeon's knots, depending on how the hitches are thrown ("Halfhitches technique", 2010)Figure 2.6: Half- hitches knot techniques. (Khattab, 2008)The compound sliding knots technique is shown in Figure 2.7. This knottechnique has more than one turn of the wrapping limb around the post (i.e., any slidingknot other than a half hitch). It can be applied in situations where the suture slidessmoothly and freely through the tissue and anchoring device. The advantage of the10
compound sliding knots is that the knots can be made to slide down the post limb withoutunraveling or jamming prematurely. Theoretical disadvantages include abrasion of sutureagainst the anchor eyelet and suture cutting through tissue as it slides (Lo, 2008),(Gunderson, 1987), (De Beer, van Rooyen, & Boezaart, 1998), (Delimar, 1996), (Fleega& Sokkar, 1999), (Holmlund, 1974), (Hughes, Hagan, Fisher, Hold, & Frostick, 2001),(Ilahi, Younas, Alexander, & Noble, 2004).Figure 2.7: Compound sliding knots. (Khattab, 2008)Due to the difficulties to operate the intra-corporeal suturing and extra-corporealknot tying technique, another technique called intra-corporeal suturing and intracorporeal knot tying technique was introduced as shown in Figure 2.8 (Topel, 1996). Inthis technique, a curved needle with suture and two elongated laparoscopic needle driversare used for suturing and knot tying. As the operation is performed inside the body, thistechnique requires high level skills to manipulate the curved needle and to pass the needlefrom the first needle driver to the next. Another difficulty of this technique is the limitedworking space available to use the knot tying instruments inside the body11
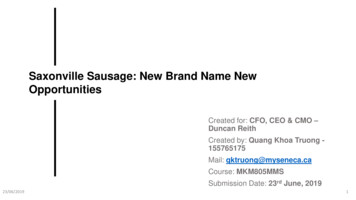
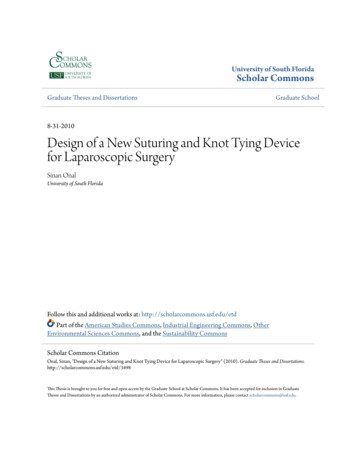
Figure 2.8: Intra-corporeal suturing and intra-corporeal knot-tying technique. (Topel,1996)2.2Commercially Available Suturing DevicesMany laparoscopic suturing systems have been developed in recent years(Kennedy, 1992), (Grace, P, & D., 1992.). However, most of them are not alwayssuccessful and sometimes cause new and different problems such as loss ofpneumoperitoneum, excess tension on the tissue that is being re-approximated, and suturebreakage during placement (Adams, et al., 1995). The most commonly used suturingdevices are Endo Stitch by Covidien and Capio by Boston Scientific, which aredescribed in the following sections.2.2.1 Endo Stitch 10 mm Suturing DeviceAs shown in Figure 2.9, Endo Stitch 10-mm ("Endostitch 10 mm suturing",2008) serviced by Covidien is one of the devices currently used for laparoscopic suturing.Endo Stitch single-use suturing device has two jaws and consists of four main parts: a12
handle, a toggle lever, a needle holder secured inside the jaws and a needle. The devicecan be operated through the handle and the toggle lever. Also, the suture is secured in themiddle of the needle so that the suture can pass through the tissue. After the needleholder is loaded with the needle and suture, the needle is passed from one jaw to the otherby closing the handles and flipping the toggle lever. Rotating the toggle lever andreleasing the handle enables the needle to stay on the opposite jaw. When this iscomplete, the needle is ready for the next maneuver. This device can also be used to tieknots as shown in Figure 2.10.Figure 2.9: Endo Stitch 10 mm suturing device [photograph]. Retrieved February 13,2010 from www.autosuture.comAdams et al.
University of South Florida Scholar Commons Graduate Theses and Dissertations Graduate School 8-31-2010 Design