Transcription
A Comparison of the Talk Testand Percent Heart-rateReserve for ExerciseProgrammingJOHN P. PORCARI, PH.D.,KATELYN FALCK-WIESE,M.S., SAMANTHA SUCKOWSTENGER, M.S., JILLIAN TUREK,M.S., ANNA WARGOWSKY,M.S., MARIA L. CRESS, M.S.,SCOTT T. DOBERSTEIN, M.S.,CHELSEA J. HAHN, M.S.,ABIGAIL L. RYSKEY, M.S. ANDCARL FOSTER, PH.D., WITHDANIEL J. GREENEXCLUSIVEACESPONSOREDRESEARCH TRADITIONALLY, EXERCISE PROGRAMS have been developed using range-basedprotocols. For example, commonly accepted fitness-industry guidelines are typicallybased on exercisers working at a percentage of their heart-rate reserve (HRR), oxygen consumption reserve (VOR), maximal heart rate (MHR) or maximal oxygen consumption (VO2max). Unfortunately, the ranges provided are often so broad thatthey provide very little real guidance to health coaches and exercise professionals.Additionally, to compound the problem, you would have to conduct a maximal exercise test with each client in order to program exercise using HR or VO2 guidelines,which is impossible in most settings due to both cost and time. Because of this,for some time researchers have tried to develop an equation that can accuratelypredict maximal heart rate in lieu of doing the maximal exercise test. While theyhave improved somewhat since the early days of “220 – Age,” these equations arestill pretty unreliable. For instance, if a trainer is using %HRR to program exercise forclients, even if two individuals have the same MHR (whether measured via testingor estimated using an equation), and therefore the same target heart rate duringexercise, the metabolic overload may be very different depending on whether thetarget heart rate is above or below the individual’s ventilatory threshold.ACE CERTIFIED May 2018 1
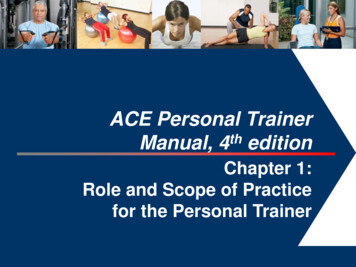
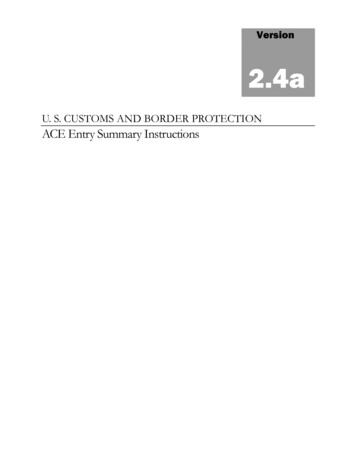
Is there a better way to individualize a client’s exerciseintensity from the outset so that you’re not wastingvaluable time in the beginning of a program when mostclients are so prone to dropout?ACE enlisted the help of John Porcari, Ph.D., and his team ofresearchers in the Department of Exercise and Sport Scienceat the University of Wisconsin–La Crosse to investigatewhether the Talk Test provides a suitable alternative torange-based programming and provokes training responsesthat are comparable to traditional guidelines.The Talk Test and the FirstVentilatory ThresholdVentilatory threshold testing, including the Talk Test,is based on what happens to ventilation during anincremental exercise test. As exercise intensity increases,ventilation increases in a somewhat linear manner. Thedeflection points seen in Figure 1 are associated withmetabolic changes within the body. The first notablepoint is called the “crossover” point and represents alevel of intensity where the body can no longer supplyits energy needs aerobically, so it needs to beginsupplementing that with anaerobic metabolism.Figure 1Ventilatory effects during aerobic exerciseTIDAL VOLUMEMINUTE VENTILATION (V E)VT2BREATHING RATEEXERCISE INTENSITYNote: VT1 First ventilatory threshold; VT2 Second ventilatory thresholdA byproduct of anaerobic metabolism is lactic acid,which begins to accumulate in the blood. That lactic acidis buffered by bicarbonate, which results in an excessproduction of carbon dioxide. This excess carbon dioxidestimulates ventilation further, resulting in the first nonlinear The StudyThe researchers recruited 44 university-aged individuals,17 male and 27 female, all of whom were sedentary. Theparticipants were randomly divided into two groups that were matched in terms of age, height, weight and VO2max,which was determined prior to the beginning of the study.Both groups completed a 10-week progressive exerciseprogram consisting of three 40-minute sessions per weekusing a cycle ergometer (30 minutes of exercise, plus a5-minute warm-up and a 5-minute cool-down). A consistentpedaling rate of 60 rotations per minute (rpm) was used,with adjustments in power output (PO) accomplished byincreasing the resistance on the bike’s flywheel.The HRR Group exercised at 40 to 59% HRR (moderateexercise) for weeks 1 through 4. For weeks 5 through8, they exercised at 50 to 69% HRR (the high end ofmoderate exercise), and then progressed to 60 to 79%HRR (the low end of the vigorous exercise range) forweeks 9 and 10.The TT (Talk Test) Group exercised at the highest POthat still allowed for comfortable speech, meaningthat they consistently exercised at or just below theirindividualized VT1.VT12increase in ventilation. This first deflection point is Theobjective of the Talk Test is to identify the point at whichtalking first becomes uncomfortable-to-challenging, but notimpossible. This point coincides with VT1. Stated simply,if the client can perform the exercise and talk comfortablyin sentences that are more than a few words in length, heor she is likely below his or her VT1. Once a client starts tohave difficulty, he or she is at or above VT1. The full protocolfor the Talk Test can be found in each of the ACE manuals.Note that the Talk Test can also be used to determine thesecond ventilatory threshold (VT2), but that was not thefocus of this study.May 2018 ACE CERTIFIEDFor both groups, intensity was assessed every five minutesduring each workout. For the HRR Group, the intensity wasadjusted as needed to stay within the target range. Thosein the TT Group recited the first 101 words of the RainbowPassage and were asked whether they could “speakcomfortably.” If they answer was a clear “yes,” then PO wasincreased by approximately 30 Watts (W). If the answerwas either “no” or a tentative “yes,” PO was decreasedby approximately 30 W. Heart rate and RPE were alsorecorded in this group to document the intensity of training,but this data was not used to regulate training intensity.
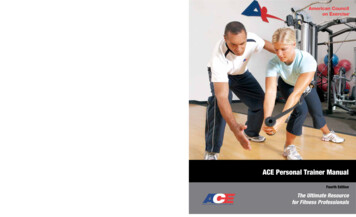
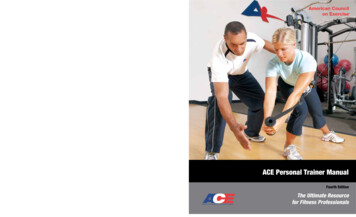
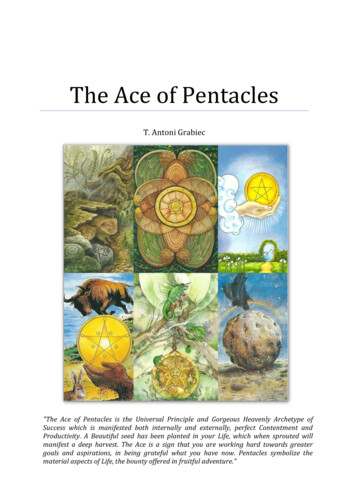
By the end of the 10 weeks, all 44 participants wereexercising at similar levels, as can be seen in Figure 2.“This proves that you don’t need an expensive maximalexercise test to identify an appropriate trainingintensity,” according to Dr. Porcari. “The Talk Test willget you and your clients to the same place.”Overall, the training intensity in both groups fell withinthe recommended training window for all measures.As expected, there was a progression of PO in bothgroups, which reflects the fact that a higher PO wasrequired to satisfy the monitoring criteria for trainingintensity. In other words, the participants workedharder over the course of the 10 weeks, denoting anincrease in physical fitness.When looking at the improvements in performance found in each group, peak PO, VO2max, PO and VO2 atVT1, and HR at VT1 improved similarly in each group,while maximal HR remained unchanged. What thismeans is that exercise capacity, no matter how andwhen it was measured, improved to the same extentregardless of whether the intensity of training wasguided by the Talk Test or %HRR (Figure 3).2.52.0**23**45*PO (w kg-1)According to Dr. Porcari, these findings clearlyillustrate the advantages of the Talk Test for exerciseprogramming, as those in the HRR Group were notworking nearly as hard as those in the TT Group forthe first eight weeks of the 10-week study. Think ofthat in a real-world scenario in which you’re workingwith a new client. If it takes you up to two months oftrial and error to find the intensity at which the clientwill derive the most benefit from the program, youare risking boring—and potentially losing—the clientduring that period when he or she is most vulnerableto dropout. In contrast, those in the TT Group wereworking at a higher, but still comfortable, intensityfrom the outset.Acute training responses in the Talk Test (TT) (closed symbols) andHeart Rate Reserve (HRR) (open symbols) groups across the 10 weeksof training. Data represent mean and standard deviation. Significantdifferences between the groups are represented by an asterisk (*).There were no significant interaction terms within the data analysis1.51.00.50.01678910910Training Weeks100%80%%HRRThe participants’ acute responses to the training arepresented in Figure 2. Training intensity, whetherexpressed in terms of PO (W/kg), %HRR or ratings ofperceived exertion (RPE), was significantly higher inthe TT Group during the first eight weeks of trainingas compared to the HRR Group. As the intensityprogressed in the HRR Group as described above, thedifferences between the two groups gradually declined.Figure 2*****4567860%40%20%0%123Training Weeks20181614RPEThe Results12108612345678910Training WeeksACE CERTIFIED May 2018 3
Figure 343321TT5040403020 125 1500420HRRVO2 at VT (mL kg-1 min-1) VO2max (mL kg-1 min-1)0HRmax (bpm)PO at VT (W/kg)4HR at VT (bpm)POmax (W/kg)Changes in maximal responses and responses at the ventilatory threshold (VT) consequent to the training in the Talk Test and HeartRate Reserve groups. The solid bars represent pretesting values and the open bars represent posttesting values. Data representmean and standard deviation.175150125TTMay 2018 ACE CERTIFIEDHRR100
raising the intensity of exercise performed at VT1, and toimprove the client’s ability to utilize fat as a fuel source.EXERCISE ENJOYMENTOnce each week for the duration of the study, theresearchers assessed participants’ enjoyment of theworkout five minutes before, at the midpoint, and fiveminutes after the training session. What they foundwas that members of both groups reported a steadydecline in how much they enjoyed the workouts(Figure 4). Part of this may be due to the fact that all30 workouts performed were exactly the same andwere of a moderate intensity, which is typically not themost exciting type of exercise. That said, Dr. Porcarihighlights the importance of variety in a trainingprogram, in terms of intensity, modality, setting and ahost of other variables. Keeping your clients interestedand happy with a program is a major key to long-termsuccess and adherence.HRR7Talk TestEnjoyability Score6543210012345678910Training WeeksFigure 4Changes in exercise enjoyability during exercise in the Talk Test(closed symbols) and Heart Rate Reserve (open symbols) groupsacross the 10 weeks of training. Data represent mean andstandard deviation.The Talk Test and the ACEIntegrated Fitness Training(ACE IFT ) Model The ACE IFT Model is featured in the ACE PersonalTrainer Manual and summarized in other ACE texts andcontinuing education offerings. The CardiorespiratoryTraining component of the ACE IFT Model was built uponthe utilization of the Talk Test, which is first introduced inPhase 1: Aerobic-base Training. In that phase, clients areencouraged to exercise at an intensity that allows them totalk comfortably, meaning that they are below their VT1.During Phase 2: Aerobic-efficiency Training, aerobic intervalsare introduced at a level that is at or just above VT1. Thegoal of these intervals is to improve aerobic endurance byDuring Phase 3: Anaerobic-endurance Training and Phase4: Anaerobic-power Training, higher-intensity intervals areintroduced that load the cardiorespiratory system enough todevelop anaerobic endurance. The key is to balance trainingtime spent below VT1 (70 to 80%), between VT1 and VT2( 10%), and at or above VT2 (10 to 20%). In Phase 4, thoseintervals performed at or above VT2 will be at a higherintensity, of a shorter duration, and with a longer recoveryperiod than those performed in Phase 3.In ConclusionThis study provides evidence that supports the efficacy ofTalk Test–based exercise programming and, therefore, of theACE IFT Model. By eliminating the need for cost-prohibitiveand time-consuming assessments, these findingsenable health and exercise professionals to offer trulyindividualized exercise programming to their clients, whichwill improve adherence and drive better results. Statedsimply, using the Talk Test allows you to train clients withouthaving to perform maximal exercise testing or rely on exerciseheart rates to guide intensity. Instead, you can have clientsexercise just below the intensity at which they lose the abilityto talk comfortably—this is VT1. The use of the Talk Testdramatically simplifies what has always been one of the mostcomplex elements of exercise programming—identifying theright intensity to effectively and safely drive results.“These findings truly revolutionize the concept of exerciseprogramming,” explains Dr. Porcari, “as they demonstratethat exercise professionals can provide individualizedintensity monitoring and exercise programming using afree and easy assessment that can be performed inalmost any setting.” Note: This study was first published in the peer-reviewedjournal Kinesiology.ReferencesAmerican College of Sports Medicine (2018). ACSM’s Guidelines for ExerciseTesting and Prescription (10th ed.). Philadelphia: Wolters Kluwer.American Council on Exercise (2014). ACE Personal Trainer Manual (5th ed.).San Diego: American Council on Exercise.Daniel J. Green is an editorial consultant and freelance writer basedin Asheville, N.C. In addition to his consulting work with organizationsincluding the American Council on Exercise, International Associationof Fire Fighters and Agriculture Future of America, Daniel writes anongoing blog series covering lifestyle change for NBCbetter.com.He has also written feature articles for local publications in WesternNorth Carolina (WNC), including WNC Parent and WNC Magazine.ACE CERTIFIED May 2018 5
The ACE IFT Model is featured in the ACE Personal Trainer Manual and summarized in other ACE texts and continuing education offerings. The Cardiorespiratory Training component of the ACE IFT Model was built upon the u