Transcription
Documentation Goals: Organizing and communicating toensure comprehensive and quality care Distinguish between a Program Driven and an Individualizedcare plan Understand the process of and elements required fordeveloping a patient centered care plan that engages thepatient and meets stakeholders needs Describe the requirements and best practices for documentingservices rendered Identify how to document an authorization for continuingservices
Admission to TreatmentINTAKE/ASSESSMENT and ReviewsI just have a fewquestions and a littlepaperwork to do. . .
Admission to TreatmentINTAKE – ASSESSMENT (The ASAM)ASSESSMENT - Part of the intake process involves assessing the patient using a full ASAM assessment.This will be used as a part of determining medical necessity and to confirm level of care placement. Title 22requires the completion and review of a Personal, Medical, and Substance use history.Completed by Counselor or LPHA; reviewed by Physician or LPHAFull Continuum ASAM (Adult/Young Adult); Full ASAM Youth (Youth 12-17)The assessment is completed in a face-to-face session between Counselor or LPHAwith beneficiaryYou have 7 days from admission to treatment date for Adults, 7-14 days for youth*. Assoon as possible is advised.The Assessment should identify the patient’s strengths, needs, and preferences; any specifiers for thediagnosis; and, impairments which support medical necessity.*“THE PULSE”: Highlights and UpdatesChanges to Youth intake period: SAPC Provider Meeting held on November 2, se.pdf
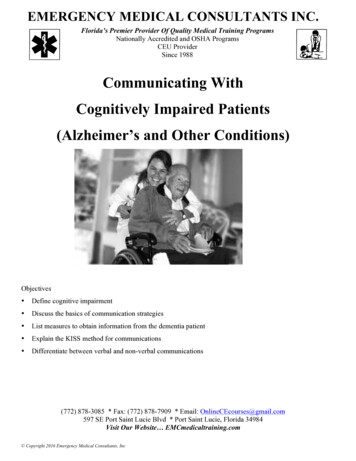
Complete all Six Dimensionsof MultidimensionalAssessment1. Acute Intoxication and/or WithdrawalPotential2. Biomedical Conditions andComplications3. Emotional, Behavioral, or CognitiveConditions and Complications4. Readiness to Change5. Relapse, Continued Use, or ContinuedProblems Potential6. Recovery and Living EnvironmentProvide “rationale” for risk ratings frominformation documented in each dimension4Utmost SeverityImminent Danger3Serious Issue, high risk ornear imminent danger2Moderate difficulty,with some persistentchronic Issues1Mild difficulty,Chronic issue likely toresolve soon0Non-issue, or very low-riskissue. chronic issues likelyto be mostly or entirelyresolved5
Admission to TreatmentINTAKE- Evaluation for DIAGNOSIS and MEDICAL NECESSITYPhysician or LPHAPerforms an Evaluation of patient for SUD Diagnosis by reviewingassessment informationThe evaluation must be performed through a review (of the Intakeassessment), face-to-face (in person or telehealth) with the counselor whoconducted the assessment (Notice #16-044). The ASAM Criteria is appliedto determine placement in the appropriate level of careYou have 7 days from the admission to treatment date. As soon aspossible is advised.The basis for the SUD diagnosis must be documented, with specifier(s) andthe basis for each specifier (reference to assessment)
Admission to TreatmentPHYSICAL EXAMFor Admission into a DMC SUD Treatment Program aPhysical Exam is required in one of the following ways:a. They have had a Physical Exam within the past 12months. Obtain copy and place in patient record;orb. Perform a new physical exam (by a physician, PA,or LNP)OR, if neither (a) or (b) has been performed,c. Include the goal of obtaining a physical exam inthe Treatment PlanPerinatal Treatment is limited to pregnant and postpartum women; medical documentation of pregnancyand the last day of pregnancy must be in the client record
Poll: Access to careOur agency received a referral from SASH last Friday afternoon. Wescheduled an assessment appointment, but we need to be sure it isconducted:a) Within 10 working days from the date it was scheduledb) Within 3 calendar days from the screening/referralc) Within 10 calendar days from the screening/referrald) On the date we scheduled it for or put the individual on a wait list
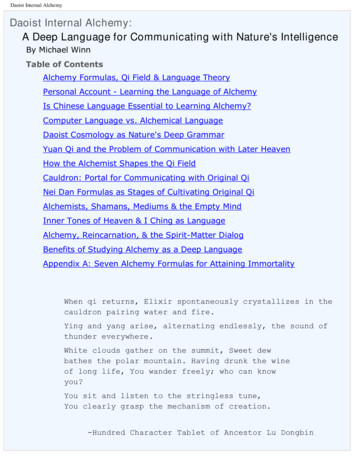
ObjectivesServicesGoalsDeveloping andImplementinga Person-Centered Care PlanASAM AssessmentOutcomesAdjust
Treatment Planning- GoalsImportant to be patient-centered, address MedicalNecessity, and always include1. Physician Exam (if necessary)2. Goal of obtaining treatment for an identified significantmedical illnessTreatment Plan is a Prescription. . .Problem: Patient has lost several teethrecently and experiences frequent,significant oral pain. Absence of dentalcare in over 7 yearsGoal: Get a dental check up and develop acare plan with dentist
LET’S START Treatment PlanningTHE TREATMENT PLAN is really the creation of a map which:1. SUMMARIZES the important CHALLENGES identified in theassessment process and GOALS and OBJECTIVES for the treatmentto be provided2. DESCRIBES services or interventions provided and responsibilities ofall parties3. Clinically ORGANIZES treatment-- the quality and continuity of careTreatment plans are necessary for ethical andreimbursable practiceThey also MODEL SOLUTION-ORIENTATIONteach PROBLEM SOLVING SKILLS. . .model and
Treatment PlanPatient-Centered, with all the right stuff. . .1. Statement of problem(s) clearly linked to issues identified in theassessment (ASAM)2. Goals to be reached that address each problem3. Action steps- Specific activities and interventions4. Target dates to complete action steps/interventions5. Description of services- type and frequency6. Assignment of Primary counselor- name7. DSM diagnosis (Both DSM-V and ICD-10 codes should be in the clinicalrecord)8. Signatures- counselor, patient, and LPHA (Typed/Printed names)—remember date(s) and signatures.
START WITH A PROBLEM STATEMENTProblem statements relate to the problems identified in theassessment. In general, Problem Statements::Accurately describe an important issue for the client- definethe problem in a clear but concise manner.Reflect client’s perception--may use client’s own wordsProblem statements should be concerned with impairment(s)or barriers to recovery (MEDICAL NECESSITY)May be broadly stated, however avoid “one-word” problems(Dependence) or addictions jargon (Denial, etc.)ASAMAssessmentProblemStatementGoals
GOAL STATEMENTSGoals statements answer the question, “What does the client need toestablish/restore healthy functioning?”It is important that goals: Promote recovery: Address identified impairments and barriers Reflect the individual’s strengths, abilities, and preferences,especially values, and cultureReaching agreement on the goal(s) is critical—if you areunable to appreciate, and capture the clients’ goals, then theplan is inherently flawed.For Example: Counselor says: “Maintain sobriety”; the Patient says: “Getmy kids back!”. . . .how could this reflect collaboration?
Can you identify an “impairment” and possible goal from the responsesbelow (from an ASAM, Dimension 5)?31. In the last 30 days, how often have you experienced cravings,withdrawal symptoms, or disturbing effects of your use?Response: I can go a couple of hours then I start to get sick and reallyhave to have get something. The buprenorphine is helping, I’m notcraving so bad. But, it doesn’t stop all of the thougths about using33. Do you feel you will continue to either relapse or continue to usewithout treatment or additional support? Yes NoResponse: I think I can do good on the buprenorphine but I was on itbefore and started thinking I could do it on my own. I’ve got to watchout and not do that again.
Identifying Problem Areas and GoalsWhich statement below best describes a problem in Dimension 5 (seeprevious slide—think medical necessity and patient centered)a) Problem: Opioid dependencyGoal: Sobrietyb) Problem: Patient lacks recovery skillsGoal: Develop recovery skillsc) Problem: Patient’s relapse risk only marginally managed by medicallyassisted treatmentGoal: Increase patient’s skill set for managing relapsed) Problem: Patient reliant on buprenorphine to manage addictionGoal: Get off buprenorphine and stay sober
GOALS NEED OBJECTIVES and INTERVENTIONSOBJECTIVES are THE ACTIONS that help to achievethe Goal.Objectives define in measurable terms the behaviors thatdemonstrate, or interventions that support, progresstoward the goal.Objectives are Behavioral interventions which are:It’s really smartSimple or straightforwardif they lead to theMeasurablePlanned outcomesAttainableRealisticTime-framedIn other words, SMART!
Timely Treatment Plans- OP/IOT Signed by Patient within 30 days of signature by counselorInitial Treatment Plan- Complete within 7 days ofadmission and signed by Counselor and Patient Reviewed and signed by LPHA within 15 days of counselorsignatureReviews- Every 30 days (min), document in client recordUpdates- Every 90 days (minimum or as needed) The LPHA must review, approve and sign within 15 calendardays of the signature by the counselorNames must be printed or typed and then signed
Timely Treatment Plans- Withdrawal Management/ResidentialWithdrawal Management- Completed at intake, signed bypatient and LPHA during treatment episodeResidentialInitial Treatment Plan- Complete within 7 days ofadmission, signed by Counselor and Patient Reviewed and signed by LPHA within 15 days of counselorsignatureReviews- Every 15 days (min), document in client recordUpdates- Every 30 days (minimum or as needed) The LPHA must review, approve and sign within 15 calendardays of the signature by the counselor Signed by Patient within 30 days of signature by counselor
Do you list all of the “problems” identified throughthe intake/assessment process on the treatmentplan? Is “As Needed” for frequency of group servicesadequate or does it need to be more specific?Whatcould Must frequency of collateral services be listed? Do you have to document anything if thepatient refuses to sign the treatment plan?PossiblyGo Wrong?
Case NotesProgress notes serve three major functions:1. They document all services rendered during the courseof treatment.2. They provide a record of all significant, individualizedClinical Treatment data.3. They indicate the degree of goal attainment (progressin treatment) made by the client.Information in the progress notes are primarily usedto evaluate progress or lack of progress in treatment. Source for reviewing and adjusting treatment plans.SAPC requires that progress notes for both groupand individual sessions follow one of 4 formats.
S.O.A.P. Method of DocumentationSubjective - client’s observations orthoughts, client statementObjective – counselor’s observations duringsessionAssessment - counselor’s understanding ofproblems and test resultsPlan – goals, objectives, and interventionsreflecting identified needs22
Other FormatsGIRPSIRPBIRPGoal: Patient’s current focus and/orshort-term goal, based on theassessment and treatment plan.Situation: Patient’s presenting situationat the beginning of interventionBehavior: Patient statements thatcapture the theme of the session andprovider observations of the patient.Quotes or paraphrase.Intervention: Methods used to addressthe patient’s goal, provider’sobservations, and treatment goals andobjectives.Intervention: Methods used to addressthe patient’s goal, provider’sobservations, and treatment goals andobjectives.Intervention: Methods used to addressthe patient’s goal, provider’sobservations, and treatment goals andobjectives.Response: Patient’s response andprogress made toward goals andobjectives.Response: Patient’s response andprogress made toward goals andobjectives.Response: Patient’s response andprogress made toward goals andobjectives.Plan: The treatment plan movingPlan: The treatment plan movingPlan: The treatment plan movingforward, based on the clinicalforward, based on the clinicalforward, based on the clinicalinformation acquired and the assessment information acquired and the assessment information acquired and the assessment
Documentation- Progress NotesOutpatient, Naltrexone Treatment , and Recovery ServicesFor each individual or group session, the counselor who conducted thatsession shall record a progress note for each participant. Must be a legible,individual narrative summary and include the following information:Topic of SessionDescription of progress toward goalsDate, Start, and End Time of each ServiceDocument location of service and if in community,how confidentiality was ensuredTyped/Printed Name of LPHA or Counselor, signature,and date note written – MUST BE WITHIN 7 DAYS OFTHE SESSION
Documentation- Progress NotesIntensive Outpatient Treatment and Residential TreatmentThe counselor shall record one progress note (at a minimum) per calendarweek for each participant. Must be a legible, individual narrative summaryand include the following information:Topic of each SessionDescription of progress toward goalsDate, Start, and End Time of each Service;Record of participant’s attendanceDocument location of service and if in community,how confidentiality was ensuredTyped/Printed Name of LPHA or Counselor, signature, and date notewritten – MUST BE WITHIN the following calendar week
Let’s talk about writing chart notes. .How do we consistently chartPROGRESS TOWARD TREATMENTPLAN GOALS AND OBJECTIVES?
Continuing Services- Level of CareASAM Reassessments- Initial and continuing assessments based on theASAM Criteria ensure that a standardized clinical structure is used tomake appropriate SUD level of care determinations.Assessments need to be appropriately documented, reviewed, andupdated on a regular basis, including at every care transition. Adequate Progress- If the provider determines that adequate progresstoward goals has been made, plans to build upon these achievementsincluding transitions to other services and recovery-focused strategiesneeds to be made. Poor Progress- Similarly, reassessments of the diagnosis, treatmentmodalities/intensity/goals need to be performed if progress towardagreed upon goals is not being made within a reasonable time.
Continuing Services Justification- DocumentationTo extend treatment past the 6-month limit the counselor mustreview the progress and eligibility of the beneficiary and make arecommendation for the client to continue or not continuereceiving services.Review by Who: LPHA (DMC-ODS)When: After 5thmonth; before 6thmonthWhat must be Documented beforeContinuing Services can beauthorized: A Review of: Beneficiary’s personal, medical,SUD history Most recent physical exam Progress notes and TP Goals Counselor’s recommendation Beneficiary’s prognosisThe patient must be discharged; there is no medical necessity
Discharge/Transfer PlanningNarrative summary of the treatment episode. Describe servicesreceived and the patient’s response by ASAM Dimensions Indicate patient’s prognosis: “Good”, “Fair”, or “Poor”, andprovide an explanation. Describe relapse triggers ; the patient’s planto avoid relapse when confronted with eachtrigger; and, support system List all patient’s medications. Include dosage and response. Indicate the reason for the discharge/referral or level of caretransferred to if appropriate. Describe recommendations for follow up.
Case Notes Progress notes serve three major functions: 1. They document all services rendered during the course of treatment. 2. They provide a record of all significant, individualized Clinical Treatment data. 3. They indicate the degree of goal attainment (progress in treatment) made by the client. I