Transcription
1Clinical operations excellence:Unlocking a hospital’s true potentialA multiprong approach that puts physicians—and clinical care—at theheart of performance transformation efforts can help hospitals andhealth systems deliver more financially sustainable, patient-oriented,and physician-friendly care.Growing financial pressures are forcing moston nonclinical operations and did not seekUS hospitals to lower their total cost of care—the active involvement of physicians. Yetespecially for the most complicated and ex-clinical care accounts for a significant portionpensive Medicare and Medicaid patients—of operational expenditures at most hospitals.while simultaneously decreasing their relianceWithout significant changes to how clinicalon cross-subsidization from commerciallycare is delivered, hospitals will not be ableinsured patients. The reasons are well-known:to achieve the 5- to 10-percent reductionemployers, payors, and consumers arein operational costs that most expertsdemanding greater cost controls. Growthbelieve is needed to cope with today’sin Medicare and Medicaid reimbursementeconomic challenges.Bede Broome,MD, PhD; KurtGrote, MD;Jonathan Scott,MD; SaumyaSutaria, MD;and Pinar Urbanrates has slowed. Further pressure is beingplaced on hospital economics by the shiftInvolving physicians in operational perfor-in payor mix from commercially insuredmance improvement efforts is thereforepatients toward more government-sponsoredcrucial. A provider that wants to lower itspatients, as well as by the ongoing migrationoperational costs by 5 to 10 percent wouldof procedures from the inpatient to thehave to reduce its nonclinical variable costsout patient setting. In addition, there is anby an average of about 30 percent if it leftincreasing move toward the use of innovative,clinical operations off the table.1 This levelvalue-based payment models as a way toof savings is unrealistic for most hospitals.incentivize reductions in the total cost ofHowever, most providers are reluctant tocare. Most providers have come to acceptaddress clinical operations, primarily for twothat these trends are not transient but ratherreasons. First, many administrators and per-have created a “new normal.”formance improvement staff members lacka clinical background and thus often shy awayAs a result, many hospitals (and the healthfrom changes that disproportionately affectsystems they are often part of) have under-clinicians and care delivery (because theytaken operational improvement programs,either do not fully understand clinical pro-such as lean transformations, Six Sigmacesses or are intimidated by the cliniciansprojects, and rapid improvement events.who carry them out). Second, many providersAlthough some of these programs havebelieve that addressing clinical operationshelped the hospitals reduce costs, few havewould alienate high-volume physicians, whoachieved substantial or long-term impact—might then take their patients to competingin large part because most of them focusedhospitals. Although this concern may once1 his estimate is based onTour experience in 150 community and academichospitals nationwide.
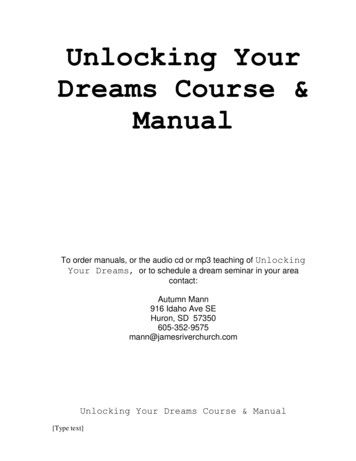
2The post-reform health system: Meeting the challenges ahead May 2013What is clinical operationsexcellence?have been justified, McKinsey researchsuggests it is no longer valid. In a surveywe recently conducted of more than 1,400US physicians, most respondents said thatClinical operations excellence includes ele-they are willing to change their practice toments of traditional hospital performancehelp control costs.improvement efforts (especially lean trans 2formations), but it goes beyond them becauseOur experience “in the field” confirms thatof the emphasis it places on improving carephysicians can be actively engaged in per delivery as well as nonclinical operationsformance improvement efforts and are willing(Exhibit 1). It uses a variety of process improve to make changes in care delivery. Theirment and change management concepts andinvolvement increases the likelihood not onlyapproaches to increase operational efficiencythat operational performance will increaseand reduce clinical variability; the ultimatebut that care quality, patients’ satisfaction,objective is to drive down the total cost of careand physician/staff satisfaction will also rise.while maintaining or improving care quality.Our “clinical operations excellence” approachIn our experience, most hospitals have signi enables hospitals to achieve all of theseficant, unintentional variability in how clinicalgoals. It is quite different from the conven-care is delivered. Most hospital executivestional change management programs mostwould agree that this variability drives up theThepost-reformhealthsystem:Meeting— Aprilhospitals2013 less competitiveprovidershave beenusing,becauseit putsthe challengescost of aheadcare, makingphysicians—and clinical care—at the heartand less likely to survive in a world of value-ClinicalOperationsof the changeeffort.ExcellenceBy doing so, providersbased payment. Reducing clinical variabilitycan make transformative changes that im-would release working capital (e.g., throughExhibit1 of 4quality, and satisfaction simultaprove costs,inventory reduction), lower supply costs (e.g.,neously, and ensure that those changes areby shifting to one or two vendors), increase thesustained over the long term.pace of care delivery (e.g., by reducingEXHIBIT 1 Clinical operations excellence encapsulates a broader rangeof initiatives than many health systems typically use2 or more informationFabout this survey, see theaccompanying article,“Engaging physicians totransform operationaland clinical performance,”on p. zation
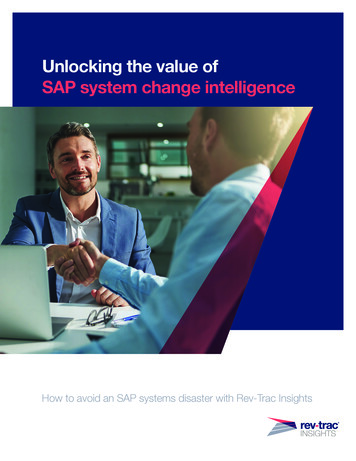
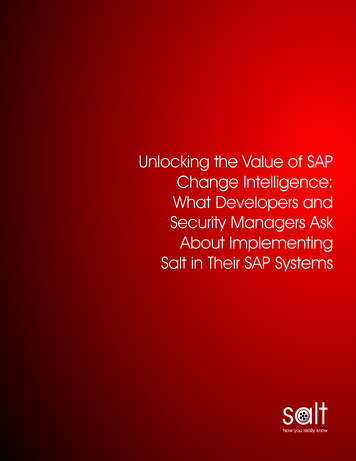
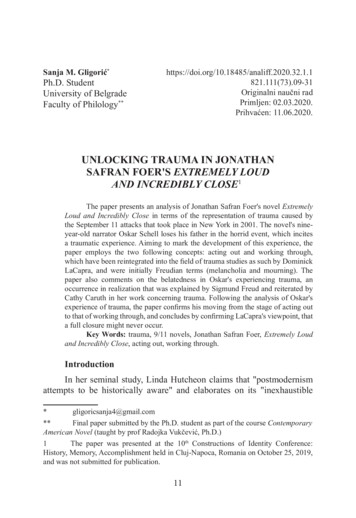
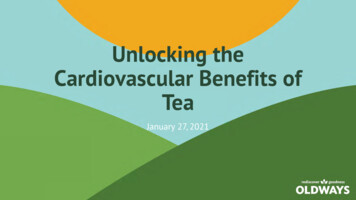
Clinical operations excellence: Unlocking a hospital’s true potentialthe number of potential paths of care), shortenImplementing the changes necessary toaverage length of stay (e.g., by initiating carereduce or eliminate unintentional variabilitysooner in the care pathway), and reduce thein care delivery in a sustainable way is farlikelihood of adverse events (e.g., by standard from easy. It requires a complex combinationizing and error-proofing nursing workflows).of approaches to streamline processes(including those for patient admissionsPhysicians can be convinced to reduce theand discharges), standardize clinical pro amount of variability in care delivery if theytocols, and rationalize supply utilization.understand that the changes will not onlyOur experience suggests, however, thathelp control costs but also improve patientthis combination can have a significantoutcomes. By ensuring that all patients re-impact (Exhibit 2).ceive high-quality care in a reproducible andevidence-driven manner, a virtuous circle canAfter using this multiprong approach inThe post-reform health system: Meeting the challengesahead — April 2013more than 150 hospital transformationsbe created: as the quality and efficiency ofcare delivery rise, per-patient costs decrease,over the past few years, we have found thatoutcomes improve, patient and staff satisfac-it can significantly improve hospital perfor-tion increase, referral streams expand, andmance. On average, most hospitals see ahigh-volume physicians become less likelyreduction of 5 percent or more in operatingto migrate to other hospitals.costs (Exhibit 3).Clinical Operations ExcellenceExhibit 2 of 4EXHIBIT 2 Achieving ‘best-in-class’ performance can have compelling valueLever‘Best-in-class’ impact achieved1Improved patient outcomesImprove outcomes by service line(e.g., 25% reduction in severe sepsis mortality)2Operational efficiency(direct variable cost reduction)Achieve positive EBITDA across MedicareProduce 15% annual reduction in ED DVCs3Improved supply utilizationAchieve sustained cost trend of 3-4% annually4Cost and capital avoidanceDelay/avoid big capital investments to increase capacity5Ability to capture disproportionatepayor volume and priceCapture 90% of available PFP funds6Increased physician retention and abilityto integrate physiciansKeep site-specific physician turnover below 7%7Nursing satisfaction and retentionKeep site-specific nursing turnover below 10%DVC, direct variable cost; EBITDA, earnings before interest, taxes, depreciation, and amortization;ED, emergency department; PFP, pay for performance.3
4The post-reform health system: Meeting the challenges ahead May 2013What prevents hospitalsfrom achieving clinicaloperations excellence?change at least some aspects of their practiceto remove waste from healthcare.3 We alsodiscovered that many physicians regard theopportunity to be involved in operationaldecision making and performance improve-In our experience, five key issues have pre-ment efforts as second only to financialvented many hospitals from achieving clinicalincentives as a way to derive satisfaction fromoperations excellence.their work. In hospitals that have achievedclinical operations excellence, strong clinicianThe first (as discussed above) is the beliefengagement is encouraged and embraced.that physicians, especially high-volume phy For example, physicians from a range ofsicians, are not willing to engage in perfor-departments collaborate in clinical councilsmance improvement efforts and will insteadto drive policy decisions and help reconcilemove their patients to other hospitals. Eventhe many different viewpoints that individualif this belief were true, hospitals would havephysicians may express.to consider whether their efforts to protectpatient volumes and profitability in the shortA second factor that can prevent hospitalsterm are hindering their longer-term pros-from achieving clinical operations excellencepects. However, our research supports ouris underestimation of the magnitude of changeexperience that this concern is unwarranted.required. Too often, hospital leaders giveIn late 2011, we surveyed 1,400 US physiciansthe change program no more time, attention,in a variety of specialties; 84 percent of theor resources than had been allocated torespondents said that they were willing toprevious, smaller improvement efforts. TheseThe post-reform health system: Meeting the challenges ahead — April 2013Clinical Operations ExcellenceExhibit 1 of 4EXHIBIT 3 Benchmarking performance is a prerequisite for achievingthe level of financial impact requiredExamples of high-impact effortsAverage across more than 30 acute-care facilities, expressed as percentage of inpatient operating costs)131The 011 McKinsey Physician2Survey.Improvement effortsImpactLean operations ED throughput/registration OR throughput/pre-admit testing Inpatient discharge 1–3%Clinical standardization ICU protocols LOS reduction IP vs. OBS determination 3–4%Combined impactfor a multifacetedimprovement effortshould be 5–10%of operating costsSupply utilization OR/procedure supply use 1–3%A comprehensiveprogram will berequired to achievethese results30 hospitals referenced here are only a fraction of the 150 hospitals in which McKinsey has led transformation efforts.ED, emergency department; ICU, intensive care unit; IP, inpatient; LOS, length of stay; OBS, observational status;OR, operating room.
Clinical operations excellence: Unlocking a hospital’s true potentialleaders fail to recognize the potential of thedepartments, and too often leaders devolvefrontline staff to implement changes andmost or all performance improvement effortshence do not invest sufficiently in frontlineto them. The staff in these departments arecapability building. Furthermore, they doleft with “accountability without authority”—not take the steps necessary to ensure thatthey are asked to drive change and holdphysicians are comfortable with the proposedclinicians and departments to specific perfor-changes and that evidence-based medicinemance targets without direct line reportingprinciples are being applied appropriately.authority to do so. To achieve strong resultsLeaders of successful programs understandwith a performance improvement program,that continuous improvement efforts do notleaders at all levels of the organization needspring up across an organization overnight,to champion and drive the effort, “role model”nor are they self-sustaining. Instead, thethe behavior they want to see, and use theirefforts require constant and significantperformance improvement group to facilitateengagement from senior leaders to setthe program.expectations, nurture new ideas, and removeroadblocks (both structural and human).Fifth, many internal performance improvementgroups have a tendency to “cut and paste”A third barrier to success is a failure to useapproaches that work in manufacturinga pragmatic, rigorously quantifiable approachdirectly into healthcare settings. However,to value creation in the clinical setting. Toomanufacturing environments are awash withoften, the improvement efforts lack carefulindustrial engineers who are comfortable usingassessments of where the value (both clini-the hardcore tools of performance improve-cal and financial) can be created and howment (e.g., variance graphs with control limits,feasible it will be to capture. Also absent isdetailed value stream maps, and fishbonea cascading approach to performance man-diagrams). Hospitals, on the other hand,agement that starts with senior leadershipemploy individuals who are very different fromand extends to the front line. In hospitalsengineers. Physicians and other clinicianswith best-in-class clinical operations pro-are trained differently than engineers are;grams, hospitals’ executives ensure thethey also think differently and use a differentsustainability of these efforts by makinglanguage. Physicians do not typically see pro-ongoing investments to build capabilitiescess measurement or improvement as a coreand strengthen performance managementpart of their role. If performance improvementsystems. By using these systems to closelyprograms are to succeed in hospitals, thetrack their performance on a range of metrics,concepts, approaches, and language musthospital leaders can begin to quantify thebe tailored to the healthcare environment andvalue they have created through decreasedthe clinical staff. Although clinicians will besupply costs, shorter length of stay, andthe critical change agents in these efforts, theyincreased payor reimbursement.are not industrial engineers, and most of themwill never achieve lean or Six Sigma certifica A fourth barrier centers around lack of leader-tion. Their training must therefore be straight-ship and role-modeling. Many health systemsforward, relevant, practical, and memorable,have built internal performance improvementand the tools they are given must be simple.5
6The post-reform health system: Meeting the challenges ahead May 2013What must a changeprogram include to achievesustainable results?on experience with similar problems encoun-Hospitals vary in their starting points, andBecause it is virtually impossible to changethus the specific goals they want to achieveclinical processes and protocols withoutthrough a clinical operations excellencethe active participation of the medical staff,program can also vary. Furthermore, theit is crucial that the physicians who workapproach used to transform a single hospitalat each hospital (both employees and thoseis somewhat different from that requiredwho simply have admitting privileges) arefor a multifacility health system. Never the-engaged in and co-lead the change program.less, a core set of tools and capabilitiesTo ensure that alignment is as broad asis required if a hospital or health systempossible, the physicians should be givenwants to reach and sustain clinical opera-ample time to ask questions about thetions excellence.improvement effort and share concernstered in other institutions.Physician engagementwith hospital leadership and other staffMind-sets and capabilitiesmembers before the effort formally begins.The performance improvement programmust include a structured approach toSome physicians should then becomechange mind-sets and build capabilitiesclosely involved in the effort. They shouldthroughout the organization, includingwork with the non-physician staff to developfrontline and back-office staff. Experiencedsolutions and be responsible for updatingtrainers should be used to ensure that allhospital leadership on progress. For exam-staff members—both those involved inple, physicians from multiple disciplinescare delivery and those working in supportshould be invited to participate in thefunctions—learn operational improvementclinical councils that determine new policiesprinciples. A core curriculum is sufficientand oversee the changes made over thefor most staff members, but some shouldlong term. As part of this work, the physi-undergo an advanced program to becomecians should help develop “best-practiceexperts in continuous improvement.bundles” that define treatment standardsfor common diagnoses and the proceduresMost adults learn best by doing, and thusthe hospital(s) will use to ensure patientthe individuals given primary responsibilitysafety. In addition, some physicians shouldfor the performance improvement efforthelp develop the new practices that willshould be given the opportunity to directlybe used to streamline registration andapply what they were taught in training.collections, because it is important thatAs soon as possible, they should beginthey understand firsthand the interdepen-to develop solutions and implement opera-dencies that exist within the organization.tional improvement techniques, including“white-board” analysis of issues, stakeholderFurthermore, the physicians closely engagedassessment, coaching from stakeholdersin the effort should be encouraged to speakon solutions, and counsel from others basedoften with their peers and hold them ac-
Clinical operations excellence: Unlocking a hospital’s true potentialOperational change in actionOver a three-year period, a large national healthsystem with more than 25 hospitals in multiplestates undertook a broad transformation programto improve quality and efficiency in its facilities.Lean improvement techniques and various otherprocess redesign principles were applied to multipleclinical and support functions. In addition, both thefrontline staff and managers (hospital and corporate)were trained in process improvement techniques.To this day, the improvement infrastructure createdduring the transformation continues to promotepositive changes within the organization.to seek additional quality and efficiency improvements in their own units.In parallel with the efforts of the multidisciplinaryteams, key frontline staff members took part in abroad-based lean operations training program, whichhelped create institutional knowledgeabout process change within the health system.The training also empowered the staff membersAnother hallmark of the transformation was thesignificant effort put into developing a robust performance tracking system. This system now generatesreports that enable the frontline staff to regularlyreview and discuss their performance and worktoward shared goals. At the same time, it gives seniorleaders at both the individual hospital and organi zational levels strong insight into the quality andefficiency of care delivery as well as the impact onfinancial performance. Results the health systemhas achieved to date include a 20- to 30-percentreduction in emergency department length of stay,a three- to six-hour improvement in discharge timesfrom inpatient units, a roughly 25-percent improvement in turn-around time in the operating rooms,and a 100-percent increase in the number of firstcase on-time operation starts. Patients are givingthe health system higher satisfaction scores becausecare providers now spend more time with them andthere are fewer delays till treatment begins. In addition, the satisfaction of physicians, nurses, and otherstaff members has risen because the level of reworkhas dropped significantly an
Keep site-specific nursing turnover below 10% The post-reform health system: Meeting the challenges ahead — April 2013 Clinical Operations Excellence Exhibit 2 of 4 DVC, direct variable cost; EBITDA, earnings before interest, taxes, depreciation, a