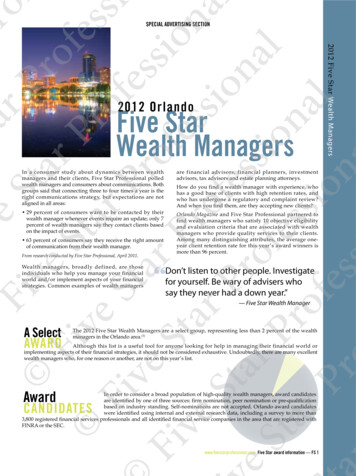
Transcription
2012 STANDARD Medicare Supplement/Life Insurance PlansIssued by Forethought Life Insurance CompanyINDIANAMS3000-01IN 0112
2012 Forethought Standard Medicare SupplementInsurance Plans You can rely on Forethought Standard Medicare Supplement Plans to help pay yourMedicare Part A and Medicare Part B charges that Medicare doesn’t cover.What’s more, you have: Five plans from which to select the coverage that best meets your needs. 30 days to review your Policy; if you’re not happy with it, we’ll refund your premium. Virtually no claims paperwork to file.et rid of glyphsThe Forethought Standard Medicare Supplementinsurance is underwritten by:Forethought Life Insurance CompanyAdministrative officePO Box 14659Clearwater, FL 33766-4659Choose the Forethought Standard MedicareSupplement Plan that’s right for you.1
Choose the Forethought plan that best fits your needs! MEDICARE PAYS PLAN A PAYS PLAN C PAYS PLAN F PAYS PLAN G PAYS PLAN N PAYSMedicare Part AHospital CoverageDeductible 1,156 1,156 1,156 1,156First 60 days100%Coinsurance61–90 daysAll but 289a day 289a day 289a day 289a day 289a day 289a dayCoinsurance91–150 days(Lifetime Reserve)All but 578a day 578a day 578a day 578a day 578a day 578a sEligibleexpensesEligibleexpenses3 pints3 pints3 pints3 pints3 Up to 144.50a dayUp to 144.50a dayUp to 144.50a dayUp to 144.50a day 140 140Generally 20%Generally 20%Generally 20%Generally 20%†Extended hospitalcoverage (up toan additional365 daysin your lifetime)Benefit for bloodAll but 3 pintsHospice CareAll but limitedcoinsurance foroutpatient drugsand inpatientrespite careSkilled NursingFacility CareFirst 20 daysCoinsurance21–100 days100%All but 144.50a dayMedicare Part BPhysician’s Servicesand SuppliesDeductibleCoinsuranceGenerally 80%Generally 20%Excess benefitsBenefit for bloodAll but 3 pints3 pints100% up to100% up toMedicare’s limit Medicare’s limit3 pints3 pints3 pints3 pints80% tolifetime maxof 50,00080% tolifetime maxof 50,00080% tolifetime maxof 50,00080% tolifetime maxof 50,000Other Benefits*Emergency carereceived outsidethe USA*Refer to the next page and your Outline of Coverage for more information.†Subject to copayment for office and emergency room visits.2
Your care benefitsMedicare Part A hospital coverageMedicare Part B physicianservices and suppliesThe Forethought Standard Medicare SupplementPlan pays the 1,156 Part A (inpatient) deductible forPlans C, F, G and N for each benefit period.Deductible – Plans C and F pay the 140 calendaryear deductible.First 60 days – After the Part A deductible, Medicarepays all eligible expenses for services from your firstthrough 60th day of hospital confinement. Servicesinclude semi-private room and board, general nursingand miscellaneous hospital services and supplies.Coinsurance – After the Part B deductible, Plans A,C, F and G generally pay 20% of eligible expenses forphysician’s services, supplies, physical and speechtherapy, and ambulance service.After the Part B deductible, Plan N generally pays 20%of the eligible expenses for physician’s services, supplies,physical and speech therapy, and ambulance servicesexcept up to a 20 copayment for office visits and upto a 50 copayment for emergency room visits.Coinsurance – Plans A, C, F, G and N pay 289 aday when you are hospitalized from the 61st daythrough the 90th day. When you are hospitalizedfrom the 91st day through the 150th day, the Planspay 578 a day for each Lifetime Reserve day used.For hospital outpatient services, the copaymentamount will be paid under a prospective paymentsystem. If this system is not used, then generally20% of eligible expenses will be paid.Extended hospital coverage – If you are in thehospital longer than 150 days during a benefit periodand you have exhausted your 60 days of Medicarelifetime reserve, Plans A, C, F, G and N pay the Part AMedicare eligible expenses for hospitalization, paidat the Diagnostic Related Group (DRG) day outlier perdiem or other appropriate standard of payment,subject to a lifetime maximum benefit of an additional365 days.Excess benefits – Your bill for Part B services andsupplies may exceed the Medicare eligible expense.When that occurs, Plan F and G will pay 100% up tothe charge limitation established by Medicare.Benefit for blood – Medicare has one calendar yeardeductible for blood that is the cost of the first threepints. Plans A, C, F, G and N pay the deductible.Benefit for blood – Medicare has one calendar yeardeductible for blood that is the cost of the first threepints. Plans A, C, F, G and N pay the deductible.Other benefits*Skilled nursing facility care – Medicare pays alleligible expenses for the first 20 days.Emergency care received outside the U.S. – Afteryou pay a calendar-year deductible, Plans C, F, G andCoinsurance – Plans C, F, G and N pay up to 144.50N pay you 80% of eligible expenses incurred duringfrom the 21st through the 100th day during which you the first 60 days of a trip up to a lifetime maximum ofreceive skilled nursing care. You must enter a Medicare 50,000. Benefits are payable for medically necessarycertified skilled nursing facility within 30 days of being emergency care.hospitalized for at least three days.Hospice care benefit – Plans A, C, F, G and N paythe copayment/coinsurance amount for all Part AMedicare eligible hospice care and respite care expenses.* Refer to the next page and your Outline of Coverage for more information.3
Forethought Medicare Supplement Plans Coinsurance is the portion of the eligible expensenot paid by Medicare and paid by Standard MedicareSupplement Plans.A Forethought Standard Medicare Supplementinsurance policy helps pay eligible expenses notpaid for by Medicare Part A and Medicare Part B.There may be charges that exceed what Medicareand your Standard Medicare Supplement insurancepolicy will pay.Benefits are paid to you, your hospital or doctor.You have 31 days from your renewal date to payyour premium. Your policy will stay inforce duringthis 31-day grace period.“Medicare Eligible Expenses” means expensescovered by Medicare to the extent recognized asreasonable and medically necessary by Medicare.Your Policy is guaranteed renewable. Your policycannot be canceled. It will be renewed as long as thepremiums are paid on time and the information onyour application is correct.Forethought Standard Medicare Supplement Planswill not pay for: Any expense incurred before your Policy Date Services for which no charge is made Expenses paid by Medicare Hospital or skilled nursing facility confinementcharges incurred prior to the effective date ofcoverage of the policy Loss or expense that is payable under anyother Medicare Supplement insurance policyor certificateYou cannot be singled out for a rate increase nomatter how many times you receive benefits. Yourpremium changes only (a) each year on the renewaldate coinciding with or following the anniversaryof your Policy Date until you reach age 99; and (b)when the same premium change is made on allinforce Forethought Standard Medicare Supplementpolicies of the same form issued to persons of yourclassification in the same geographic area ofyour state.Medicare Part A Eligible Expenses for hospital/skilled nursing facility care includeexpenses for semi-private room and board, generalnursing and miscellaneous services and supplies.This is a brief description of your coverage. Thisbrochure must be accompanied by the Outline ofCoverage. For a complete description of benefits,exceptions and limitations, please read your Outlineof Coverage and your Policy.A Benefit Period begins the first full day you arehospitalized and ends when you have not beenin a hospital or skilled nursing facility for 60consecutive days.Not connected with or endorsed by the UnitedStates government or the federal Medicareprogram.Medicare Part B Eligible Expenses for medicalservices include expenses for physician’s services,hospital outpatient services and supplies, physicaland speech therapy, and ambulance service.This is a solicitation of insurance and an agent willcontact you by telephone.*Refer to the next page and your Outline of Coverage for more information.4
Forethought Life Insurance Company Administrative Office P.O. Box 14659, Clearwater, FL 33766-4659 (877) 492-5870Outline of Medicare Supplement Coverage – Cover PageBenefit Plans A, C, F, G and NBenefit Chart of Medicare Supplement Plans Sold for Effective Dates on or After June 1, 2010This chart shows the benefits included in each of the standard Medicare supplement plans. Every company must make Plan “A” available. Some plans may not beavailable in your state. Plans E, H, I and J are no longer available for sale.Basic Benefits:Hospitalization: Part A coinsurance plus coverage for 365 additional days after Medicare benefits end.Medical Expenses: Part B coinsurance (generally 20% of Medicare-approved expenses), or copayment for hospital outpatient services. Plans K, L and N requireinsured to pay a portion of Part B coinsurance or copayments.Blood: First three pints of blood each year.Hospice: Part A coinsurance.ABCDF*GBasic,including100% Part BcoinsuranceBasic,including100% Part BcoinsuranceBasic,including100% Part BcoinsuranceBasic,including100% Part BcoinsuranceBasic,including100% Part BcoinsuranceBasic,including100% Part BcoinsuranceSkilledNursing FacilitycoinsuranceSkilledNursing FacilitycoinsuranceSkilledNursing FacilitycoinsuranceSkilledNursing FacilitycoinsurancePart ADeductiblePart BDeductiblePart ADeductiblePart ADeductiblePart BDeductiblePart BExcess(100%)Part ADeductiblePart ADeductibleKHospitalization andpreventive care paidat 100%; other basicbenefits paid at 50%LNBasic, including 100%Hospitalization andBasic, Including Part B coinsurance, exceptpreventive care paidup to 20 copayment for100% Part Bat 100%; other basicoffice visit, and up to 50coinsurancebenefits paid at 75%copayment for ER50% SkilledNursing Facilitycoinsurance75% SkilledNursing FacilitycoinsuranceSkilledNursing FacilitycoinsuranceSkilledNursing Facilitycoinsurance50% Part ADeductible75% Part ADeductible50% Part ADeductiblePart ADeductibleForeign TravelEmergencyForeign TravelEmergencyPart BExcess(100%)ForeignForeignForeignForeignTravel Emergency Travel Emergency Travel Emergency Travel Emergency* Plan F also has an option called a high deductible Plan F. This high deductibleplan pays the same benefits as Plan F after one has paid a calendar year 2,070deductible. Benefits from high deductible Plan F will not begin until out-of-pocketexpenses exceed 2,070. Out-of-pocket expenses for this deductible areexpenses that would ordinarily be paid by the policy. These expenses includeMedicare deductibles for Part A and Part B, but do not include the plan’s separateforeign travel emergency deductible.MSOC10-01M1Out-of-Pocketlimit 4660paid at 100%after limitreachedOut-of-Pocketlimit 2330;paid at 100%after limitreached 2012 ForethoughtIN 0112
PREMIUM INFORMATIONYour premium will increase each year because of the increase in your attained age. We, Forethought Life Insurance Company, can alsoraise your premium if (a) we change the premium rates which apply to all policies of this form issued by us and in-force in your state; (b)coverage under Medicare changes; or (c) you move to a different ZIP code location.DISCLOSURESUse this Outline to compare benefits and premiums among policies.This outline shows benefits and premiums of policies sold for effective dates on or after June 1, 2010. Policies sold for effectivedates prior to June 1, 2010 have different benefits and premiums. Plans E, H, I and J are no longer available for sale.READ YOUR POLICY VERY CAREFULLYThis is only an Outline, describing your policy’s most important features. The Policy is your insurance contract. You must read the Policyitself to understand all of the rights and duties of both you and Forethought Life Insurance Company.RIGHT TO RETURN POLICYIf you find that you are not satisfied with your policy, you may return it to Forethought Life Insurance Company, P.O. Box 14659,Clearwater, FL 33766-4659. If you send the policy back to us within 30 days after you receive it, we will treat the policy as if it had neverbeen issued and return all of your premiums.POLICY REPLACEMENTIf you are replacing another health insurance policy, do NOT cancel it until you have actually received your new policy and are sure youwant to keep it.NOTICEThis policy may not fully cover all of your medical costs. Neither Forethought Life Insurance Company nor its agents are connectedwith Medicare. This Outline of Coverage does not give all the details of Medicare coverage. Contact your local Social Security Office orconsult Medicare and You for more details.COMPLETE ANSWERS ARE VERY IMPORTANTWhen you fill out the application for the new policy, be sure to answer truthfully and completely all questions about your medical andhealth history. The Company may cancel your Policy and refuse to pay any claims if you leave out or falsify important medical information.Review the application carefully before you sign it. Be certain that all information has been properly recorded.MSOC10-012IN 0112
FORETHOUGHT LIFE INSURANCE COMPANY - Monthly Premium Rates *These rates apply to ZIP codes starting with: 460, 461, 465 through 469, 472 through 479Standard Plans - NonsmokerPlan AN/A 77.91 80.58 84.17 86.93 89.60 92.15 94.57 96.85 98.90 100.68 103.21 106.73 108.11 110.45 111.66 112.88 114.01 116.16 117.12 117.99 119.94 120.75 121.57 122.38 123.21 125.23 126.10 127.00 127.93 128.88 131.04 131.95 132.78 133.59 134.41Plan CN/A 103.06 106.46 111.04 114.70 118.47 122.14 125.67 129.06 132.17 135.06 139.02 144.37 146.85 150.64 152.92 155.21 157.44 161.14 163.18 165.18 168.71 170.66 172.68 174.66 176.70 180.46 182.57 184.76 187.02 189.38 193.55 195.93 198.20 200.51 202.88FemalePlan FN/A 105.55 109.03 113.72 117.48 121.34 125.09 128.70 132.18 135.36 138.31 142.37 147.84 150.38 154.25 156.59 158.93 161.21 164.99 167.08 169.13 172.73 174.73 176.80 178.82 180.91 184.75 186.91 189.15 191.45 193.87 198.14 200.57 202.89 205.24 207.66Plan GN/A 85.49 88.29 92.07 95.11 98.26 101.32 104.28 107.13 109.75 112.19 115.54 120.04 122.16 125.36 127.32 129.29 131.20 134.35 136.11 137.85 140.86 142.56 144.33 146.06 147.83 151.10 152.99 154.96 156.98 159.10 162.74 164.88 166.92 169.01 171.15Plan NN/A 75.56 78.02 81.34 84.02 86.83 89.58 92.24 94.81 97.17 99.40 102.44 106.51 108.47 111.39 113.20 115.03 116.82 119.70 121.37 123.01 125.79 127.41 129.09 130.73 132.42 135.45 137.26 139.13 141.05 143.07 146.47 148.51 150.48 152.48 154.54AttainedAge 8990919293949596979899Plan AN/A 89.59 92.67 96.79 99.97 103.04 105.98 108.75 111.38 113.73 115.78 118.69 122.74 124.32 127.02 128.41 129.81 131.11 133.59 134.68 135.69 137.94 138.86 139.80 140.74 141.70 144.02 145.02 146.05 147.12 148.22 150.70 151.74 152.70 153.63 154.57Plan CN/A 118.52 122.43 127.70 131.91 136.25 140.46 144.52 148.42 152.00 155.31 159.87 166.03 168.88 173.23 175.86 178.50 181.06 185.31 187.65 189.96 194.01 196.26 198.58 200.86 203.21 207.53 209.96 212.48 215.07 217.79 222.59 225.32 227.93 230.58 233.31MalePlan FN/A 121.38 125.39 130.78 135.10 139.54 143.85 148.00 152.00 155.66 159.06 163.72 170.02 172.94 177.39 180.08 182.77 185.40 189.74 192.14 194.49 198.64 200.94 203.32 205.65 208.04 212.46 214.94 217.52 220.17 222.95 227.86 230.65 233.32 236.03 238.81Plan GN/A 98.31 101.53 105.88 109.38 113.00 116.52 119.92 123.20 126.21 129.02 132.87 138.05 140.48 144.17 146.42 148.68 150.88 154.50 156.53 158.53 161.99 163.95 165.98 167.96 170.01 173.76 175.94 178.20 180.52 182.96 187.15 189.61 191.96 194.36 196.82Plan NN/A 86.90 89.72 93.54 96.63 99.86 103.02 106.07 109.03 111.75 114.31 117.80 122.48 124.74 128.09 130.18 132.28 134.34 137.66 139.57 141.46 144.66 146.52 148.46 150.34 152.29 155.77 157.84 160.00 162.21 164.53 168.44 170.79 173.05 175.35 177.72* To obtain annual, semiannual, or quarterly premiums, multiply the Monthly Premium Amount by 12, 6, or 3, respectivelyMSOC10-013IN 0112
FORETHOUGHT LIFE INSURANCE COMPANY - Monthly Premium Rates *These rates apply to ZIP codes starting with: 460, 461, 465 through 469, 472 through 479Standard Plans - SmokerPlan AN/A 89.59 92.67 96.79 99.97 103.04 105.98 108.75 111.38 113.73 115.78 118.69 122.74 124.32 127.02 128.41 129.81 131.11 133.59 134.68 135.69 137.94 138.86 139.80 140.74 141.70 144.02 145.02 146.05 147.12 148.22 150.70 151.74 152.70 153.63 154.57Plan CN/A 118.52 122.43 127.70 131.91 136.25 140.46 144.52 148.42 152.00 155.31 159.87 166.03 168.88 173.23 175.86 178.50 181.06 185.31 187.65 189.96 194.01 196.26 198.58 200.86 203.21 207.53 209.96 212.48 215.07 217.79 222.59 225.32 227.93 230.58 233.31FemalePlan FN/A 121.38 125.39 130.78 135.10 139.54 143.85 148.00 152.00 155.66 159.06 163.72 170.02 172.94 177.39 180.08 182.77 185.40 189.74 192.14 194.49 198.64 200.94 203.32 205.65 208.04 212.46 214.94 217.52 220.17 222.95 227.86 230.65 233.32 236.03 238.81Plan GN/A 98.31 101.53 105.88 109.38 113.00 116.52 119.92 123.20 126.21 129.02 132.87 138.05 140.48 144.17 146.42 148.68 150.88 154.50 156.53 158.53 161.99 163.95 165.98 167.96 170.01 173.76 175.94 178.20 180.52 182.96 187.15 189.61 191.96 194.36 196.82Plan NN/A 86.90 89.72 93.54 96.63 99.86 103.02 106.07 109.03 111.75 114.31 117.80 122.48 124.74 128.09 130.18 132.28 134.34 137.66 139.57 141.46 144.66 146.52 148.46 150.34 152.29 155.77 157.84 160.00 162.21 164.53 168.44 170.79 173.05 175.35 177.72AttainedAge 8990919293949596979899Plan AN/A 103.03 106.57 111.31 114.96 118.50 121.87 125.07 128.08 130.79 133.15 136.50 141.15 142.97 146.07 147.67 149.28 150.78 153.62 154.89 156.04 158.63 159.69 160.77 161.85 162.95 165.62 166.77 167.96 169.19 170.45 173.30 174.51 175.60 176.67 177.76Plan CN/A 136.30 140.79 146.85 151.70 156.68 161.53 166.19 170.69 174.80 178.61 183.86 190.93 194.21 199.22 202.24 205.27 208.22 213.10 215.80 218.45 223.11 225.69 228.37 230.99 233.69 238.66 241.45 244.35 247.33 250.46 255.97 259.12 262.12 265.17 268.31MalePlan FN/A 139.59 144.20 150.40 155.36 160.47 165.43 170.20 174.80 179.01 182.91 188.28 195.52 198.88 204.00 207.09 210.19 213.21 218.20 220.96 223.67 228.44 231.08 233.81 236.49 239.25 244.33 247.18 250.15 253.19 256.39 262.03 265.25 268.32 271.43 274.64Plan GN/A 113.06 116.77 121.77 125.78 129.95 134.00 137.91 141.68 145.14 148.37 152.80 158.75 161.56 165.79 168.38 170.98 173.52 177.67 180.01 182.31 186.29 188.54 190.87 193.16 195.51 199.82 202.33 204.93 207.60 210.41 215.22 218.05 220.76 223.51 226.34Plan NN/A 99.93 103.18 107.57 111.12 114.84 118.47 121.98 125.38 128.51 131.45 135.47 140.86 143.45 147.31 149.71 152.13 154.49 158.31 160.51 162.68 166.36 168.50 170.72 172.89 175.13 179.14 181.52 184.00 186.54 189.22 193.70 196.41 199.01 201.66 204.38* To obtain annual, semiannual, or quarterly premiums, multiply the Monthly Premium Amount by 12, 6, or 3, respectivelyMSOC10-014IN 0112
FORETHOUGHT LIFE INSURANCE COMPANY - Monthly Premium Rates *These rates apply to ZIP codes starting with: 470, 471Standard Plans - NonsmokerPlan AN/A 82.58 85.42 89.22 92.14 94.98 97.68 100.24 102.66 104.83 106.72 109.40 113.13 114.59 117.08 118.36 119.65 120.85 123.13 124.14 125.07 127.14 127.99 128.86 129.73 130.61 132.75 133.67 134.62 135.61 136.62 138.90 139.87 140.75 141.60 142.48Plan CN/A 109.25 112.85 117.70 121.59 125.58 129.47 133.21 136.81 140.10 143.16 147.36 153.03 155.66 159.68 162.10 164.53 166.89 170.80 172.97 175.09 178.83 180.90 183.04 185.14 187.30 191.29 193.52 195.85 198.24 200.74 205.17 207.69 210.10 212.54 215.05FemalePlan FN/A 111.89 115.57 120.55 124.52 128.62 132.59 136.42 140.11 143.48 146.61 150.91 156.71 159.40 163.51 165.98 168.4
The Forethought Standard Medicare Supplement . insurance is underwritten by: Forethought Life Insurance Company Administrative office. PO Box 14659 Clearwater, FL 33766-4659 Choose the Forethought