Transcription
A Medicare Approved Prescription Drug PlanEnvisionRx Plus Gold (PDP)2011 Formulary(List of Covered Drugs)PLEASE READ: THIS DOCUMENT CONTAINS INFORMATION ABOUT THE DRUGS WECOVER IN THIS PLANNote to existing members: This formulary has changed since last year. Please review this document tomake sure that it still contains the drugs you take.Beneficiaries must use network pharmacies to access their prescription drug benefit. Benefits, formulary,pharmacy network, premium and/or copayments/coinsurance may change on January 1, 2011.Beneficiaries who wish to receive materials in an alternate format or language please call: 1-866-250-2005.HPMS Approved Formulary File Submission ID 11248, Version Number 12OFFERED BY ENVISION INSURANCE COMPANY, A MEDICARE-APPROVED PART D SPONSORPO BOX 1298, TWINSBURG, OHIO 44087-1298S7694 2011 CF File & Use 09062010
What is the EnvisionRx Plus Formulary?A formulary is a list of covered drugs selected by EnvisionRx Plus in consultation with a team of health careproviders, which represents the prescription therapies believed to be a necessary part of a quality treatmentprogram. EnvisionRx Plus will generally cover the drugs listed in our formulary as long as the drug ismedically necessary, the prescription is filled at an EnvisionRx Plus network pharmacy, and other plan rulesare followed. For more information on how to fill your prescriptions, please review your Evidence ofCoverage.Can the Formulary change?Generally, if you are taking a drug on our 2011 formulary that was covered at the beginning of the year,we will not discontinue or reduce coverage of the drug during the 2011 coverage year except when anew, less expensive generic drug becomes available or when new adverse information about the safetyor effectiveness of a drug is released. Other types of formulary changes, such as removing a drug fromour formulary, will not affect members who are currently taking the drug. It will remain available atthe same cost-sharing for those members taking it for the remainder of the coverage year. We feel it isimportant that you have continued access for the remainder of the coverage year to the formulary drugsthat were available when you chose our plan, except for cases in which you can save additional moneyor we can ensure your safety.If we remove drugs from our formulary, or add prior authorization, quantity limits and/or step therapyrestrictions on a drug or move a drug to a higher cost-sharing tier, we must notify affected members ofthe change at least 60 days before the change becomes effective, or at the time the member requests arefill of the drug, at which time the member will receive a 60-day supply of the drug. If the Food andDrug Administration deems a drug on our formulary to be unsafe or the drug’s manufacturer removesthe drug from the market, we will immediately remove the drug from our formulary and provide noticeto members who take the drug. The enclosed formulary is current as of August 1, 2011. To getupdated information about the drugs covered by EnvisionRx Plus, please visit our Web site atwww.envisionrxplus.com or call Member Services at1-866-250-2005, 24 hours a day, 7 days a week.TTY/TDD users should call 1-866-763-9630. If we make certain non-routine changes to coverage fordrugs, we will send members an errata sheet to update the formulary they received.How do I use the Formulary?There are two ways to find your drug within the formulary:Medical ConditionThe formulary begins on page 1. The drugs in this formulary are grouped into categories depending onthe type of medical conditions that they are used to treat. For example, drugs used to treat a heartcondition are listed under the category, “cardiovascular agents”. If you know what your drug is used for,look for the category name in the list that begins on page number 1. Then look under the category namefor your drug.S7694 2011 CF File & Use 09062010ii
Alphabetical ListingIf you are not sure what category to look under, you should look for your drug in the Index that begins onpage 43. The Index provides an alphabetical list of all of the drugs included in this document. Bothbrand name drugs and generic drugs are listed in the Index. Look in the Index and find your drug. Nextto your drug, you will see the page number where you can find coverage information. Turn to the pagelisted in the Index and find the name of your drug in the first column of the list.What are generic drugs?EnvisionRx Plus covers both brand name drugs and generic drugs. A generic drug is approved by theFDA as having the same active ingredient as the brand name drug. Generally, generic drugs cost lessthan brand name drugs.Are there any restrictions on my coverage?Some covered drugs may have additional requirements or limits on coverage. These requirements and limitsmay include:Prior Authorization: EnvisionRx Plus requires you or your physician to get prior authorization forcertain drugs. This means that you will need to get approval from EnvisionRx Plus before you fillyour prescriptions. If you don’t get approval, EnvisionRx Plus may not cover the drug.Quantity Limits: For certain drugs, EnvisionRx Plus limits the amount of the drug that EnvisionRxPlus will cover. For example, EnvisionRx Plus provides 240 tablets per prescription for Tramadol50mg. This may be in addition to a standard one month or three month supply.Step Therapy: In some cases, EnvisionRx Plus requires you to first try certain drugs to treat yourmedical condition before we will cover another drug for that condition. For example, if Drug A andDrug B both treat your medical condition, EnvisionRx Plus may not cover Drug B unless you tryDrug A first. If Drug A does not work for you, EnvisionRx Plus will then cover Drug B.You can find out if your drug has any additional requirements or limits by looking in the formulary thatbegins on page 1. You can also get more information about the restrictions applied to specific covereddrugs by visiting our Web site at www.envisionrxplus.com.You can ask EnvisionRx Plus to make an exception to these restrictions or limits. See the section, “How do Irequest an exception to the EnvisionRx Plus’s formulary?” on page iv for information about how to requestan exception.S7694 2011 CF File & Use 09062010iii
What if my drug is not on the Formulary?If your drug is not included in this formulary, you should first contact Member Services and confirm thatyour drug is not covered. If you learn that EnvisionRx Plus does not cover your drug, you have two options:You can ask Member Services for a list of similar drugs that are covered by EnvisionRx Plus. Whenyou receive the list, show it to your doctor and ask him or her to prescribe a similar drug that iscovered by EnvisionRx Plus.You can ask EnvisionRx Plus to make an exception and cover your drug. See below for informationabout how to request an exception.How do I request an exception to the EnvisionRx Plus’s Formulary?You can ask EnvisionRx Plus to make an exception to our coverage rules. There are several types ofexceptions that you can ask us to make.You can ask us to cover your drug even if it is not on our formulary.You can ask us to waive coverage restrictions or limits on your drug. For example, for certain drugs,EnvisionRx Plus limit the amount of the drug that we will cover. If your drug has a quantity limit,you can ask us to waive the limit and cover more.You can ask us to provide a higher level of coverage for your drug. If your drug is contained in ournon-preferred tier, you can ask us to cover it at the cost-sharing amount that applies to drugs in thepreferred tier instead. This would lower the amount you must pay for your drug. Please note, if wegrant your request to cover a drug that is not on our formulary, you may not ask us to provide ahigher level of coverage for the drug. Also, you may not ask us to provide a higher level of coveragefor drugs that are in the Specialty Drug tier (Tier 5).Generally, EnvisionRx Plus will only approve your request for an exception if the alternative drugs includedon the plan’s formulary, the lower-tiered drug or additional utilization restrictions would not be as effectivein treating your condition and/or would cause you to have adverse medical effects.You should contact us to ask us for an initial coverage decision for a formulary, tiering or utilizationrestriction exception. When you are requesting a formulary, tiering or utilization restriction exceptionyou should submit a statement from your physician supporting your request. Generally, we must makeour decision within 72 hours of getting your prescriber’s or prescribing physician’s supporting statement.You can request an expedited (fast) exception if you or your doctor believe that your health could beseriously harmed by waiting up to 72 hours for a decision. If your request to expedite is granted, we mustgive you a decision no later than 24 hours after we get your prescriber’s or prescribing physician’ssupporting statement.S7694 2011 CF File & Use 09062010iv
What do I do before I can talk to my doctor about changing my drugs or requesting anexception?As a new or continuing member in our plan you may be taking drugs that are not on our formulary. Or, youmay be taking a drug that is on our formulary but your ability to get it is limited. For example, you may needa prior authorization from us before you can fill your prescription. You should talk to your doctor to decideif you should switch to an appropriate drug that we cover or request a formulary exception so that we willcover the drug you take. While you talk to your doctor to determine the right course of action for you, wemay cover your drug in certain cases during the first 90 days you are a member of our plan.For each of your drugs that is not on our formulary or if your ability to get your drugs is limited, we willcover a temporary 30-day supply (unless you have a prescription written for fewer days) when you go to anetwork pharmacy. After your first 30-day supply, we will not pay for these drugs, even if you have been amember of the plan less than 90 days.If you are a resident of a long-term care facility, we will cover a temporary 31-day transition supply (unlessyou have a prescription written for fewer days). We will cover more than one refill of these drugs for the first90 days you are a member of our plan. If you need a drug that is not on our formulary or if your ability to getyour drugs is limited, but you are past the first 90 days of membership in our plan, we will cover a 31-dayemergency supply of that drug (unless you have a prescription for fewer days) while you pursue a formularyexception.Current members experiencing level of care changes will follow the transition policy as outlined above.For more informationFor more detailed information about your EnvisionRx Plus prescription drug coverage, please review yourEvidence of Coverage and other plan materials.If you have questions about EnvisionRx Plus, please call Member Services at1-866-250-2005, hours a day,7 days a week. TTY/TDD users should call 1-866-763-9630. Or visit www.envisionrxplus.com.If you have general questions about Medicare prescription drug coverage, please call Medicare at 1-800MEDICARE (1-800-633-4227) 24 hours a day/7 days a week. TTY/TDD users should call 1-877-486-2048.Or, visit www.medicare.gov.EnvisionRx Plus’s FormularyThe formulary that begins on the next page provides coverage information about some of the drugs coveredby EnvisionRx Plus. If you have trouble finding your drug in the list, turn to the Index that begins on page43.S7694 2011 CF File & Use 09062010v
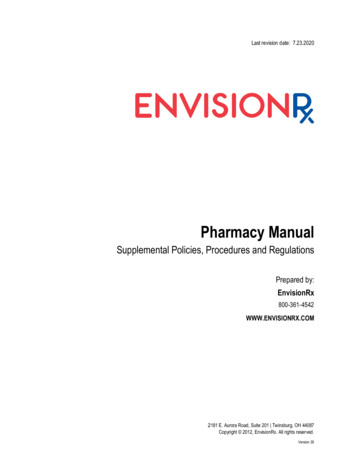
The first column of the chart lists the drug name. Brand name drugs are capitalized (e.g., CYMBALTA) andgeneric drugs are listed in lower-case italics (e.g., ibuprofen).The information in the Notes column tells you if EnvisionRx Plus has any special requirements for coverageof your drug.STStep TherapyPAPrior AuthorizationQLQuantity Limit per 30-day supplySPThis prescription may be available only at certain pharmacies. For more information consult yourPharmacy Directory or call Member Services at 1-866-250-2005, 24 hours a day, 7 days a week. TTY/TDDusers should call 1-866-763-9630.*We provide additional coverage of this prescription drug in the coverage gap. Please refer to our Evidenceof Coverage for more information about this coverage.All drugs in Tiers 1 through 4 are available via mail-order with a 90-day supply prescription. SpecialtyDrugs (Tier 5) are limited to a 30-day supply at mail-order.Below is a chart showing your co-payment/co-insurance by drug tier after you have met yourdeductible but prior to entering the coverage gap for the Gold Plan.Formulary Drug TierCo-payment/Co-insuranceretail pharmaciesTier 1 4 12Tier 225%25%Tier 3 25 75Tier 425%25%Tier 525%25%, limited to 30-day supplyS7694 2011 CF File & Use 09062010viat Co-payment/Co-insurance atMail Order and 90 day atretail pharmacies
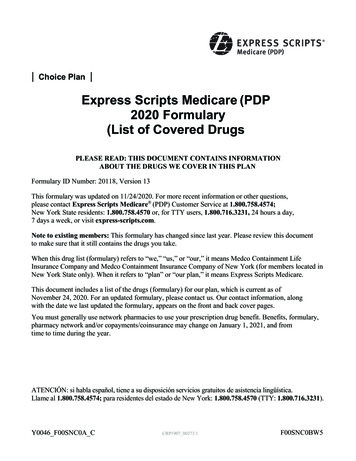
Drug NameANALGESICSTierNotesDrug Namehydrocodone/apap 5/325 mghydrocodone/apap 10/325 mghydrocodone/apap 10/500 mghydrocodone/apap 10/650 mghydrocodone/apap 10/660 mghydrocodone/apap 2.5/500 mghydrocodone/apap 5/500 mg thydrocodone/apap 7.5/ 750 mghydrocodone/apap 7.5/325 mghydrocodone/apap 7.5/500 mghydrocodone/apap 7.5/650 mghydrocodone/ibuprofen 7.5/200hydromorphone 10 mg/ml inj sohydromorphone 2 mg tablethydromorphone 4 mg tablethydromorphone 8 mg tabletKADIAN 10 MG ER CAPSULEKADIAN 100 MG ER CAPSULEKADIAN 20 MG ER CAPSULEKADIAN 200 MG ER CAPSULEKADIAN 30 MG ER CAPSULEKADIAN 50 MG ER CAPSULEKADIAN 60 MG ER CAPSULEKADIAN 80 MG ER CAPSULEmethadone 1 mg/ml solutionmethadone 10 mg tabletmethadone 10 mg/ml solutionmethadone 10 mg/ml inj solmethadone 2 mg/ml solutionmethadone 5 mg tabletmethadose 10 mgmethadose 5 mgmorphine 0.5 mg/ml inj *******Non-opioid Analgesicsdiflunisal 500 mg tablet1*meclofenamate 100 mg capsul1*meclofenamate 50 mg capsule1*Opioid Analgesicsapap/codeine solution1*apap/codeine tablet1*apap/codeine #3 tablet1*apap/codeine #4 tablet1*ascomp/codeine capsule1*astromorph 0.5 mg/ml inj sol1*astromorph 1 mg/ml inj sol1*buprenorphine 0.3 mg/ml inj s1*buprenorphine 2 mg sl tablet2buprenorphine 8 mg sl tablet2butal/apap/caff/codeine cap1*duramorph 0.5 mg/ml1*duramorph 1 mg/ml inj sol1*EMBEDA 100-4MG CAPSULE4EMBEDA 20/0.8 MG CAPSULE4EMBEDA 30/1.2MG CAPSULE4EMBEDA 50/2 MG CAPSULE4EMBEDA 60-2.4MG CAPSULE4*EMBEDA 80-3.2MG CAPSULE4*endocet /apap 10/650 mg tab1**endocet /apap 7.5/325mg tab1**endocet/apap 5/325 mg tabl1**endocet/apap 10 /325mg tabl1**endocet/apap 7.5 /500mg tab1**hydrocodone /apap 5 /500mg1**hydrocodone bit/apap 10/750 m1**hydrocodone/apap solution1**We provide additional coverage of this prescription drug in the coverage gap. Please refer to our Evidence of Coverage for moreinformation about this coverage. PA-Prior Authorization Required ST-Step Therapy Required QL-Quantity Limit per 30 days SPOnly Available through Specialty Pharmacy EnvisionRxPlus Gold 2011 Formulary last updated (07/26/2011)1
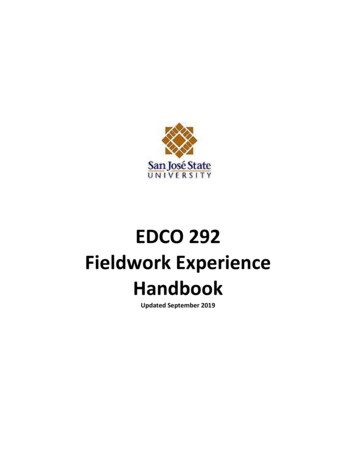
Drug Namemorphine 1 mg/ml inj solmorphine 15 mg tabletmorphine 2 mg/ml solutionmorphine 30 mg tabletmorphine 4 mg/ml solutionmorphine 5 mg/ml inj solmorphine sulfate 20 mg/ml sOPANA ER 10 MG TABLETOPANA ER 15 MG TABLETOPANA ER 20 MG TABLETOPANA ER 30 MG TABLETOPANA ER 40 MG TABLETOPANA ER 5 MG TABLETOPANA ER 7.5 MG TABLEToxycodone /apap 7.5 /500mgoxycodone 15 mg tabletoxycodone 30 mg tabletoxycodone 5 mg tabletoxycodone/apap 2.5/325 mgoxycodone/apap 10 /325mg taoxycodone/apap 5/325 mg taboxycodone/apap 7.5 /325mg toxycodone/aspirin tabletoxycodone/ibuprofen tabletOXYCONTIN 10 MG ER TABLETOXYCONTIN 15 MG ER TABLETOXYCONTIN 20 MG ER TABLETOXYCONTIN 30 MG ER TABLETOXYCONTIN 40 MG ER TABLETOXYCONTIN 60 MG ER TABLETOXYCONTIN 80 MG ER TABLEToxymorphone 10 mg tabletoxymorphone 5 mg *****Drug Namepentazocine /apap 25/650 mgpentazocine /naloxone 50 /0.5roxicet solutionroxicet 5/500 mg tabletroxicet 5/325 mg tabletroxicodone 5 mg tabletSUBOXONE 2-0.5MG SL TABLETSUBOXONE 8-2MG SL TABLETtramadol 100 mg er tablettramadol 200 mg er tablettramadol /apap tablettramadol 50 mg tabletTierNotes111112442211*****QL 240 *QL 240 *11**ANESTHETICS*Local Anestheticslidocaine 10 mg/ml inj sollidocaine 5 mg/ml inj solANTI-INFLAMMATORY AGENTSNonsteroidal Anti-inflammatory DrugsCELEBREX 200 MG CAPSULE4*CELEBREX 400 MG CAPSULE4*CELEBREX 50 MG CAPSULE4*CELEBREX 100 MG CAPSULE4diclofenac 100 mg er tablet1*diclofenac 25 mg ec tablet1*diclofenac 50 mg tablet1*diclofenac 50 mg ec tablet1*diclofenac 75 mg ec tablet1*etodolac 200 mg capsule1*etodolac 300 mg capsule1*etodolac 400 mg tablet1*etodolac 400 mg er tablet2etodolac 500 mg tablet1*etodolac 500 mg er tablet2*We provide additional coverage of this prescription drug in the coverage gap. Please refer to our Evidence of Coverage for moreinformation about this coverage. PA-Prior Authorization Required ST-Step Therapy Required QL-Quantity Limit per 30 days SPOnly Available through Specialty Pharmacy EnvisionRxPlus Gold 2011 Formulary last updated (07/26/2011)2
Drug Nameetodolac 600 mg er tabletfenoprofen 600 mg tabletFLECTOR 15 MG/HR PATCHflurbiprofen 100 mg tabletflurbiprofen 50 mg tabletibuprofen 20 mg/ml suspensiibuprofen 400 mg tabletibuprofen 600 mg tabletibuprofen 800 mg tabletindomethacin 25 mg capsuleindomethacin 50 mg capsuleindomethacin 75 mg er capsuleketoprofen 200 mg er capsuleketoprofen 50 mg capsuleketoprofen 75 mg capsuleketorolac 10 mg tabletketorolac 15 mg/ml inj solketorolac 30 mg/ml inj solmeloxicam 1.5 mg/ml suspensmeloxicam 15 mg tabletmeloxicam 7.5 mg tabletnabumetone 500 mg tabletnabumetone 750 mg tabletnaproxen 500mg tabnaproxen 25 mg/ml suspensionaproxen 250 mg tabletnaproxen 375 mg tabletnaproxen 375 mg ec tabletnaproxen 500 mg ec tabletnaproxen sodium 275 mg tablnaproxen sodium 550 mg tabloxaprozin 600 mg tabletpiroxicam 10 mg ********Drug Namepiroxicam 20 mg capsulesulindac 150 mg tabletsulindac 200 mg tablettolmetin 200 mg tablettolmetin 400 mg capsuletolmetin 600 mg tabletVOLTAREN 0.01 MG/MG idesgentamicin 0.9 mg/ml inj so1*gentamicin 1 mg/ml inj sol1*gentamicin 1.2 mg/ml inj so1**gentamicin 1.4 mg/ml inj so1**gentamicin 1.6 mg/ml inj so1**gentamicin 10 mg/ml inj sol1**gentamicin 40 mg/ml inj sol1**kanamycin 333 mg/ml inj sol1**tobramycin 10 mg/ml inj sol2tobramycin 40 mg/ml inj sol2Antibacterials, Otherbaciim inj sol1**clindamycin 150 mg capsule1**clindamycin 150 mg/ml inj sol1**clindamycin 300 mg capsule1**colistimethate 75 mg/ml inj s5*LINCOCIN 300 MG/ML INJ SOL4*metronidazole 250 mg tablet1**metronidazole 375 mg capsul1**metronidazole 5 mg/ml inj sol1**metronidazole 500 mg tablet1**trimethoprim 100 mg tablet1**VANCOCIN 5 MG/ML INJ SOL4PA*VANCOCIN HCL 125 MG CAPSULE5*We provide additional coverage of this prescription drug in the coverage gap. Please refer to our Evidence of Coverage for moreinformation about this coverage. PA-Prior Authorization Required ST-Step Therapy Required QL-Quantity Limit per 30 days SPOnly Available through Specialty Pharmacy EnvisionRxPlus Gold 2011 Formulary last updated (07/26/2011)3
Drug NameVANCOCIN HCL 250 MG CAPSULEvancomycin 100 mg/ml inj solvancomycin 50 mg/ml inj solZYVOX 20 MG/ML SUSPENSIONZYVOX 600 MG TABLETZYVOX 2 MG/ML INJ SOLBeta-lactam, Cephalosporinscefaclor 25 mg/ml suspensiocefaclor 250 mg capsulecefaclor 50 mg/ml suspensiocefaclor 500 mg capsulecefaclor 500 mg er tabletcefaclor 75 mg/ml suspensiocefazolin 20 mg/ml inj solcefazolin 200 mg/ml inj solcefazolin 225 mg/ml inj solcefazolin 330 mg/ml inj solcefdinir 25 mg/ml suspensiocefdinir 300 mg capsulecefdinir 50 mg/ml suspensiocefepime 160 mg/ml inj solcefepime 280 mg/ml inj solcefoxitin 180 mg/ml inj solcefoxitin 200 mg/ml inj solcefoxitin 95 mg/ml inj solceftriaxone 100 mg/ml inj solceftriaxone 250 mg/ml inj solceftriaxone 350 m
S7694_2011 CF File & Use 09062010 ii What is the EnvisionRx Plus Formulary? A formulary is a list of covered drugs selected by EnvisionRx Plus in consultation with a team of health care providers, which represents the prescription therapi