Transcription
Provider Group/Facility Information Change Form (ICF-02)The data provided on this form or additional formFor changes to your corporation or businesswith equivalent data is used by Blue Shield ofstructure: Please submit the Articles ofCalifornia (Blue Shield) and/or Blue Shield ofIncorporation with this form.California Promise Health Plan (Blue ShieldPromise) to add, change, or remove information For changes to your EmployerIdentification Number (EIN) oron an established provider group or facilityTax Identification Number (TIN):record. Blue Shield and/or Blue Shield Promise willPlease submit a signed W-9 orconfirm that the request has been processed.Department of Treasury/InternalInstructionsRevenue Service (IRS) taxIdentify the provider group or facility requiringdocument.changes by populating the Business Name/DBA,Tax Identification Number(TIN), and National require a current location license.Provider Identifier (NPI) fields. Complete allRequest must be on letterhead with anapplicable fields that require changes. Attach allrequired documentation, as outlined below, andreturn this form to Blue Shield and/or Blue ShieldPromise via email atChanges to facility locations mayauthorized signature. For all other changes to your information,no supporting documentation is required.BSCProviderInfo@blueshieldca.com. This form maybe completed electronically.Changes to Roster MembersTo add/change/remove a roster member, refer tothe instructions on the roster page of this form.Copies of roster pages can be used to send anupdate with additional practitioners.Required DocumentationThis request will not be initiated until all therequired documentation, as indicated below, isreceived by Blue Shield and/or Blue ShieldPromise. Failure to provide the requireddocumentation will result in no action beingAdditional InformationThis form is only used to update existing providergroup or facility records. To create a newprovider group or facility record, pleasecomplete the Provider Group/Facility RecordApplication (Form RA- 02). This form is not anagreement to participate in the Blue Shieldand/or Blue Shield Promise provider network. Forinformation about joining either network, pleasecontact our Provider Information andEnrollment Department via email atBSCProviderInfo@blueshieldca.comtaken.Blue Shield of California is an independent member of the Blue Shield AssociationICF-02 (1/21)
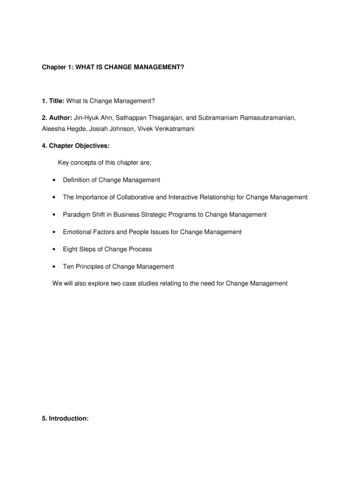
Provider Group/Facility Information Change Form (ICF-02)By submitting this form applicant certifies on behalf of this provider record that all information included on this form is true, accurate and complete. Any false statements,the concealment of material fact, or the use of false documents may lead to prosecution under applicable federal or state laws. Applicant certifies under penalty ofperjury that the foregoing is true and correct. To ADD information, check the ADD box and use the NEW column. To CHANGE information, check the CHANGE box anduse the EXISTING and NEW columns. To REMOVE information, check the REMOVE box and use the EXISTING column.Identify the provider group record requiring change(s):Business Name/DBATax identification number (TIN)National Provider Identifier (NPI)Identify group/facility changes:AddChangeRemoveInformationBusiness name/DBAExistingNewPrimary Specialty/type of serviceTIN (attach pre-printed taxdocument or W-9)NPILicense NumberService location addressWheelchair accessPhone number (required for newlocations)TelehealthYesTelehealth visitsNoIn-person office visitsYesTelehealth visitsNoIn-person office visitsICF-02 (1/21)Blue Shield of California is an independent member of the Blue Shield Association
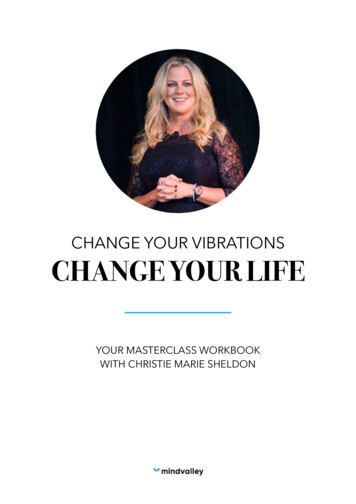
Provider Group/Facility Information Change Form (ICF-02)By submitting this form applicant certifies on behalf of this provider record that all information included on this form is true, accurate and complete. Any false statements,the concealment of material fact, or the use of false documents may lead to prosecution under applicable federal or state laws. Applicant certifies under penalty ofperjury that the foregoing is true andcorrect. To ADD information, check the ADD box and use the NEW column. To CHANGE information, check the CHANGE box anduse the EXISTING and NEW columns. To REMOVE information, check the REMOVE box and use the EXISTING column.Identify the provider group record requiring change(s):Business Name/DBATax identification number (TIN)National Provider Identifier (NPI)Identify group/facility changes:AddChangeRemoveInformationExistingNewFax numberAfter hours phone numberBusiness email for Blue Shield'sadministrative useOffice hoursQualified medical interpreter Cantonese Russian Vietnamese N/A Spanish Mandarin Korean Cantonese Russian Vietnamese N/A Spanish Mandarin KoreanClinical staff languageBilling addressBilling phone numberBilling fax numberICF-02 (3/21)Blue Shield of California is an independent member of the Blue Shield Association.
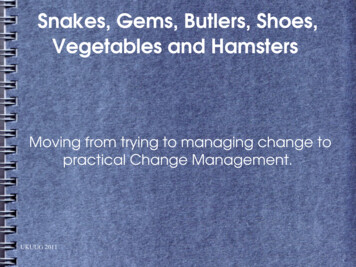
Provider Group/Facility Information Change Form (ICF-02)By submitting this form applicant certifies on behalf of this provider record that all information included on this form is true, accurate andcomplete. Any false statements, the concealment of material fact, or the use of false documents may lead to prosecution underapplicable federal or state laws. Applicant certifies under penalty of perjury that the foregoing is true and correct. To ADD information,check the ADD box and use the NEW column. To CHANGE information, check the CHANGE box and use the EXISTING and NEW columns.To REMOVE information, check the REMOVE box and use the EXISTING column.Changes to roster practitioners:Business name/DBATax identification number (TIN)Service locationAddChangeRemoveInformationPractitionerfull nameRoster Member 1ExistingNewPractitioner nerspecialtyLicense numberSocial securitynumber (SSN)NPISupervisingphysician(if tyPatientGenderlimitations:acceptanceN/AHospital basedpractitionerHospital affiliationnames (for MD esNoICF-02 (1/21)Blue Shield of California is an independent member of the Blue Shield Association
Provider Group/Facility Information Change Form (ICF-02)AddChangeRemoveInformationPractitionerfull nameRoster Member 2ExistingNewPractitioner nerspecialtyLicense numberSocial securitynumber (SSN)NPISupervisingphysician(if ceptanceN/AHospital basedpractitionerHospital affiliationname(s) (for MDor DO)YesNoYesMaleonlyFemaleonlyNoICF-02 (1/21)Blue Shield of California is an independent member of the Blue Shield Association
provider group or facility record, please complete the Provider Group/Facility Record Application (Form RA- 02). This form is not an agreement to participate in the Blue Shield and/or Blue Shield Promise provider network. For information about joining either network, please contact our Provider Informatio