Transcription
The Management of theCOVID-19 Patient withRespiratory FailureJames Allen, MDMedical Director, The Ohio State University WexnerMedical Center East HospitalProfessor of Internal MedicineDivision of Pulmonary and Critical Care MedicineThe Ohio State University Wexner Medical CenterCoronaviruses Hosts: humans, other mammals, birds Frequent cause of the common cold Accounts for 5-10% of adult URIs Typical symptoms: fever, cough, sorethroat Can cause viral pneumonia or bronchitis Primarily occur in winter and early spring Spread by aerosol droplets and contactwith secretions No effective vaccines or approved antivirals Investigational anti-virals available forcompassionate useCredit: NIAID-RMLCOVID-19 Virus SARS-CoV-2 Originated in Wuhan, China November2019 Coronavirus strains causing severe illness: SARS* MERS* COVID-19 **These strains do NOT present like the common coldand present with flu-like symptoms1
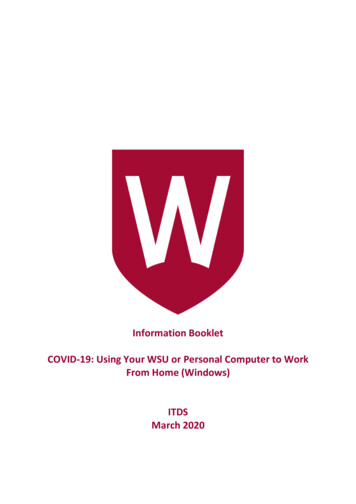
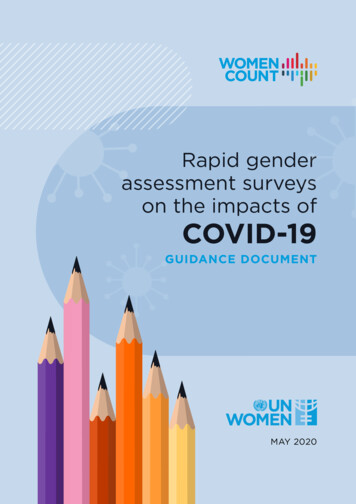
Mortality Rates Of ViralOutbreaks 1918 – 1919 Influenza2002 – 2004 SARS2014 – 2017 MERS2019 – 2020 COVID-19Influenza 2019-2020 Season10%10%37%3.7%Common Presenting SymptomsMortality RateCOVID-19 mortality by ageN 201Age (years)JAMA Intern Med. doi:10.1001/jamainternmed.2020.09942
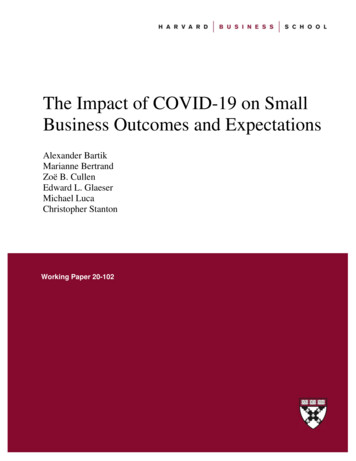
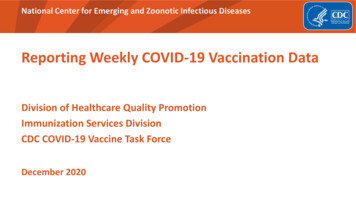
Symptoms at PresentationMedian Timeline ofDisease ProgressionN 201JAMA Intern Med. doi:10.1001/jamainternmed.2020.0994Risk Factors for RespiratoryFailure:Wuhan Jinyintan Hospital, ChinaHuang C et al Clinical features of patients infected with 2019 novel coronavirusin Wuhan, China. Lancet. 2020;395(10223):497-506. doi: 10.1016/S01406736(20)30183-5Risk Factor for RespiratoryFailure:Wuhan Jinyintan Hospital, China ARDS risk factors: 84 of 201 patients (42%) developed ARDS 44 of 84 patients (52%) died Average hospital stay – 13 days 71% discharged (6.5% still hospitalized attime of writing)JAMA Intern Med. doi:10.1001/jamainternmed.2020.0994 Older age Neutrophilia Elevated LDH or D-dimer High fever at presentation was a risk forARDS but was also associated with a lowermortalityJAMA Intern Med. doi:10.1001/jamainternmed.2020.09943
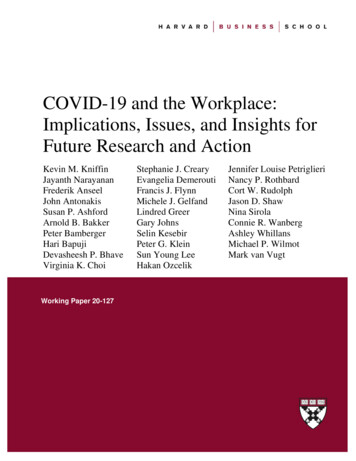
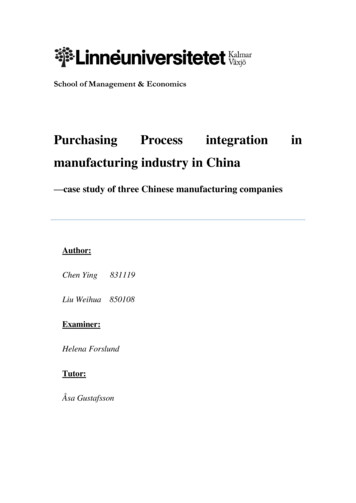
Respiratory Management:Wuhan Jinyintan Hospital, ChinaClinical Characteristics ofHospitalized Patients:Zhongnan Hospital of WuhanUniversity, China 138 patients 40 of these were healthcare workers Median age 56 years ICU median 66 years Non-ICU 51 years Symptoms: Fever (98.6%) Fatigue (69.6%) Cough (59.4%) Chest CT: bilateral patchy or ground glass infiltrates in allpatientsJAMA 2020; 3231061-9JAMA Intern Med. doi:10.1001/jamainternmed.2020.0994Clinical Characteristics ofHospitalized Patients:Zhongnan Hospital of WuhanUniversity, China 36 patients (26.1%) of patients required ICU care; ofthese: ARDS (61.1%) Arrhythmia (44.4%) Shock (30.6%) Median time intervals: Symptom onset to dyspnea: 5 days Symptom onset to hospitalization: 7 days Symptoms onset to ARDS: 8 days Average hospital stay 10 days Average mortality 4.3%JAMA 2020; 3231061-9Clinical Characteristics ofHospitalized Patients:Zhongnan Hospital of WuhanUniversity, China ICU respiratory management: 11.1% heated high flow oxygen 41.7% non-invasive ventilation 47.2% intubation and mechanical ventilation 4 of these switched to ECMO 36% of patients required vasopressors 2 patients required dialysisJAMA 2020; 3231061-94
Cause of Death due to COVIDPatients Needing ICU Care Older persons (mean age is about 60 yearsold) Co-morbid disease Diabetes Cardiac disease Hypertension Most common reason for needing ICU ARDSRuan Q, Clinical predictors of mortality due to COVID-19 based on an analysis of data of150 patients from Wuhan, China. Intensive Care Med. 2020 Mar 3. doi: 10.1007/s00134-02005991-x. [Epub ahead of print]JAMA. Published online March 11, 2020. doi:10.1001/jama.2020.3633 Hypertension Diabetes Heart disease Persistent lymphopeniaRising D-dimerRising LDHRising troponinwww.thelancet.com Published online March 9, -dimer (ug/ml) Older age Co-morbiditiesTroponin (pg/ml)Risks for mortality inCOVID-19 infectionRisks for mortality inCOVID-19 infectionwww.thelancet.com Published online March 9, 2020 https://doi.org/10.1016/S0140-6736(20)30566-35
ICU Utilization: ItalianLombardi ICU NetworkCT Findings In COVID 17 patients admittedto West China Guang’an Hospital ofSichuan University Average 4 dayssymptoms prior toadmission Findings: 70% ground glassopacities 30% ground glass consolidativeopacitiesGrasselli, G et al. Critical Care Utilization for the COVID-19 Outbreak in Lombardy, Italy.JAMA. Published online March 13, 2020. doi:10.1001/jama.2020.4031Day #1 Location: 82% bilateral 18% unilateral 88% had both upper &lower lobeinvolvement There were no Pleural effusions Tree-in-bud infiltrates CavitiesZhang S, Li H, Huang S, et al. High-resolution CT features of 17 cases of Corona Virus Disease 2019 inSichuan province, China. Eur Respir J 2020; in press (https://doi.org/10.1183/13993003.00334-2020)Day #26
Day #3Management of Respiratory Failure in COVID19Management of Respiratory Failure in COVID19 Certain procedures and therapies may result inaerosolization of the virus If feasible, consider early intubation in patientsrequiring 6LNC Reduces aerosols. Also, temporizing measuresmay delay intubation Experienced intubator Rapid Sequence Intubation (RSI) with paralytic. Video Laryngoscopy may allow operator moredistance from airway Bougie may increase first pass success PPE: N95, contact, and droplet precautions Airborne Infection Isolation Room Consider avoiding High flow nasal cannula ( 6LPM O2) Heated high flow nasal cannula Non-Invasive Positive Pressure Ventilation(unless closed exhalation circuit) Nebulizers, intrapulmonary percussiveventilation, percussive chest physiotherapy,and Metanebs Bronchoscopy7
Management of Critical Illness Hemodynamic supports as needed, keep MAP 65 1st line in septic shock: norepinephrine 2nd line: vasopressin 3rd line: epinephrine Judicious fluid resuscitation in hypoxic respiratoryfailure Evaluate for organ dysfunction: Urine output/creatinine, liver function testing andechocardiogram, Consider impact of testing on hospitaldecontamination; will bedside or point of care testingsuffice?Respiratory failurein COVID-19 is dueto ARDSDon’t Miss The MimicsCardiogenic pulmonary edema Physical exam: S3 orS4, elevated JVP,moist crackles? Elevated BNP level? Cardiac echo?Other forms of pneumonia Influenza Bacterial pneumonia If they present withsepsis, startantibioticsimmediatelyNormal (low power)ARDS (high power)8
Fluid Balance across the LungMovement of fluid across each compartment can bepredicted by “Starling’s Law”Normal lungAlveolusStarling’s Law can be completely derived by ’s Law(V IR)I Conductance (Pressure Gradient)HydrostaticOncoticBasementMembraneJv Kfc[(Ppc – PT) – ( P - T)]Flux of ility (filtration)Coefficient for ction coefficient1.0 means all reflectedAlveolusColloid apillaryHydrostaticColloid OncoticHydrostaticColloid OncoticCapillary9
Effect of lying down supineZone 1PA Pa PvZone 2Zone 3PA alveolar pressurePa arterial pressurePv venous pressurePa PA PvZone 1PA Pa PvZone 2Pa Pv PAPa PA PvPa Pv PAZone 3In ARDS, the dependent parts ofthe lung are often the worstAnterior - chestPosterior- backSo, what if you couldflip the patient over?10
NormalAlveolusInhalationThe treatment ofARDS is AlveolusExhalationNormalARDS11
lationAddition Of10 cm rmalAddition Of10 cm PEEP:InhalationNo veolusInhalationAddition Of10 cm on Of10 cm PEEP:ExhalationNo PEEPPEEP12
How The Mortality Rate Of ARDSWas Reduced By 22%Over‐DistendedAlveolusInhalationAddition Of10 cm on Of10 cm PEEP:ExhalationNo PEEPPEEP High Volume Group Starting Vt 12ml/kg Kept plateaupressure 50 cm Low Volume Group Starting Vt 6ml/kg Kept plateaupressure 30 cmMortality RateN Engl J Med 2000; 342:1301-1308COVID-19 Do’s and Don’tsDO:DON’T: DVT prophylaxis GI prophylaxis 30-45 degree bedelevation Vasopressors for MAP 65 Enteral nutrition within24-48 hours Routinely usecorticosteroids Over-sedate patients Routinely useparalytics Use hypotoniccrystalloids or colloidsolutions for shockThe disaster that youdrill for is not thedisaster that you getWHO guideline: Clinical management of severe acute respiratoryinfection (SARI) when COVID-19 disease is suspected13
Planning for ICU surge capacity Are there other hospital locations that can beconverted to ICU? Step-down units Surgical post-op recovery areas Cath lab recovery areas Endoscopy rooms and recovery areas Operating rooms Are there other staff that can be deployed for ICUcare? Can you acquire additional ventilators? Do you have additional dialysis capacity?Mechanical ventilation topics1. Ventilatorsa)Modesb)Oxygenation and ventilationc)Settings2. ARDSa)Low tidal volume ventilationb)Prone positioning3. Refractory hypoxemia4. Liberation from the ventThe Management of theCOVID-19 Patient withRespiratory FailureRachel Quaney, MDClinical Instructor of Internal MedicineDivision of Pulmonary, Critical Care,and Sleep MedicineThe Ohio State University Wexner Medical CenterVentilator modesAssistControlSIMVPressureSupport14
Ventilator modesVentilator modesSet respiratory IMVPressureSupportNo set rateFull supporteach breathVentilator modesVentilator modesAssist Control - VolumeControlAssistControlVolumeControlFull support on ventilatorinitiated breathsPartial support on patientinitiated breathsRRPressureControlVTPEEPFiO2PEEPFiO2Assist Control - PressureControlRRDP*15
Ventilation and OxygenationInspiratory time andexpiratory time I:E ratio how much time spent ininspiration vs expirationRRVTPEEPVentilationFiO2Oxygenation I:E I:E Oxygenation Ventilation Ventilation OxygenationRR x VT minuteventilationInspiratory time and expiratory time I:E ratio how much time spent in inspiration vsexpiration Normal 1:1.5 or higher Ways to control this depending on ventilator and mode I-time (seconds) usually 1-1.5 sec Flow rate (L/min) usually 60-120 L/minI-timeRRInspirationExpirationI:E ratio1.5 sec2030 seconds30 seconds1:11 sec2020 seconds40 seconds1:2Picking and changing settings1Match their initial needs2Adjust as needs change3Avoid iatrogenic damage16
Picking and changing settingsInitial settings-hypoxemic respiratory failurewith or at risk for ARDSAssist Control - Volume Control1Match their initial needs2Adjust as needs change3Avoid iatrogenic damageRRVTPEEPFiO216‐24 bpm6‐8 mL/kg PBW5‐10 cmH20100%Assist Control - Pressure ControlRR16‐24 bpmInitial settings -obstructive lung disease(COPD or asthma)DP15 cmH20PEEP5‐10 cmH20FiO2100%metabolic acidosisInitial settings- (DKA,AKI, shock, toxins)Assist Control - Volume ControlRR10‐14 bpmVTPEEP8 mL/kg PBW 0‐5 cmH20FiO2100%Assist Control - Pressure ControlPressure SupportRRExample:RRDPPEEPFiO210‐14 bpm15‐20 cmH200‐5 cmH20100%PSPEEPFiO2Initial values of pH 7 / PaCO2 14 with HCO3 5 mmol/L “normal” assist control settings ineffective ventilation and worsening acidosis17
metabolic acidosisInitial settings- (DKA,AKI, shock, toxins)Picking and changingsettingsPressure SupportRRPSPEEPFiO2 10‐5 cmH205‐10 cmH20100%Example:Initial values of pH 7 / PaCO2 14 with HCO3 5 mmol/L1Match their initial needs2Adjust as needs change3Avoid iatrogenic damage “normal” assist control settings ineffective ventilation and worsening acidosisMonitors Blood gas pH PaCO2 PaO2 Pulse oximetry SpO2&Goals Oxygenation PaO2 60 mmHg SpO2 90%Adjusting for oxygenationor ventilationRRVTPEEPFiO2PaO2 too lowPaO2 too high Ventilation pH 7.2-7.45 PaCO2pH too lowpH 7.1 / PaCO2 70pH too highpH 7.5 / PaCO2 30*hypoventilating soincrease minute ventilation*hyperventilating sodecrease minute ventilation permissivehypercapnia exceptwith increasedintracranial pressure18
Picking and changing settings1Match their initial needs2Adjust as needs change3Avoid iatrogenic damageVolutraumaIssues to avoid withmechanical ventilation Volutrauma Auto peepingAuto peeping Also known as overdistention of alveoli Also known as “dynamic hyperinflation” or“breath stacking” More important contributor to ventilator inducedlung injury than barotrauma What it is: When not enough time to exhale before anew breath is delivered Recommend conservative tidal volumes Specifically low tidal volume ventilationwith ARDS Why it is bad: Not appropriately ventilating Thoracic over-inflation can lead tocardiovascular compromise19
Auto peepingMechanical ventilation topicsnormalinspiration How to tell: Ventilator flow waveform Expiratory hold maneuverflowtime What to do:normalincomplete Decrease respiratory rateexpirationexpiration Lower I:E ratio Shorter inspiration time and longer expiration time1. Ventilatorsa)Modesb)Oxygenation and ventilationc)Settings2. ARDSa)Low tidal volume ventilationb)Prone positioning3. Refractory hypoxemia4. Liberation from the ventARDS definitionImagingBilateral opacitiesEtiologyNot fully explained by heart failure orvolume overload 1 week since onset or insultTiming1. Diagnose ARDS2. Set up ventilator with low tidal volume ventilationSeverity:(with PEEP 5)Mild ARDSModerate ARDSPaO2/FiO2 ratio 200‐300 mmHg 100‐200 mmHgSevere ARDS 6 mL/kg PBW, as based on sex and height3. Adjust VT and RR to reach pH and plateaupressure goals 100 mmHgPaO2150PaO250FiO20.5FiO21.04. Adjust PEEP and FiO2 to reach oxygenation goal20
Plateau pressure Plateau pressure goal 30 mmHg Measure Pplat every 4 hours and withchanges in PEEP or VT0.5-1 second inspiratory holdPIPPplatPIPpressurePEEPPEEPtimetimePlateau pressure If Pplat 30: decrease VT by 1 mL/kg incrementally(minimum 4 mL/kg) If Pplat 25 and VT 6 mL/kg: increase VT by 1 mL/kg until Pplat 25 or VT 6 mL/kg If Pplat 30 and breath stacking or dyssynchrony: increase VT by 1 mL/kg incrementally to 7-8 mL/kg ifPplat remains 3021
Other therapies for ARDS Prone positioning ECMOProne positioning Early prone positioning in severe ARDS hasmortality benefit Consider early on in patient’s course if P:F 150 How it works: Prone positioning contraindications compression of left lung by the heart dependent atelectasis from interstitial edemaAllows more lung regions to be functionalImproves V/Q mismatchProne positioning – logistics Absolute contraindication: Open wound of neck, chest, or abdomen Relative contraindications: Hemodynamic instability Elevated intracranial pressure Recent trauma or surgery Unstable fractures Face/neck 15 days Sternotomy 30 days Pregnancy 20% BSA burns Requiring impending surgery/procedure22
Prone positioning – logisticsMechanical ventilation topics1. Ventilatorsa)Modesb)Oxygenation and ventilationc)Settings2. ARDSa)Low tidal volume ventilationb)Prone positioning3. Refractory hypoxemia4. Liberation from the ventRefractory hypoxemia Prone positioningECMOInhaled epoprostenol or nitric oxideNeuromuscular blockadeCaution againstnebulizedmedications withconfirmedCOVID-19 or PUINeuromuscular blockade 2010 ACURASYS trial mortality benefit 2019 ROSE trial no mortality benefit compared tolighter sedation Bottom line: Not needed for all ARDS patients Still useful for significant vent dyssynchrony ORrefractory hypoxemia If used: Ensure adequate continuous sedation and analgesia Ensure DVT prophylaxis23
Mechanical ventilation topics1. Ventilatorsa)Modesb)Oxygenation and ventilationc)Settings2. ARDSa)Low tidal volume ventilationb)Prone positioning3. Refractory hypoxemia4. Liberation from the ventThe ICU Liberation Bundle ABCDEF bundle A assess, prevent, manage pain B both SAT SBT C choice of analgesia and sedation D delirium: assess, prevent, and manage E early mobility and exercise F family engagement and empowermentSAT SBTSAT SBTSAT Daily todetermine ifeligible forextubationCriteria:Performance: No active Hold lischemia,elevated ICPSATFailure: Anxiety, agitation,pain RR 35 SpO2 88% Acute arrhythmiaSBTCriteria:Performance: Failure: SpO2 88% 30-60 RR 35 or 8 PEEP 8minutes of SpO2 88% Respiratory FiO2 50%minimal Hemodynamicallydistressventstable Mental statussupportchange Acute arrhythmia Daily todetermine ifeligible forextubationCriteria:Performance: No active Hold lischemia,elevated ICPFailure: Anxiety, agitation,pain RR 35 SpO2 88% Acute arrhythmiaResume sedation at ½ doseSBTCriteria:Performance: Failure: SpO2 88% 30-60 RR 35 or 8 PEEP 8minutes of SpO2 88% Respiratory FiO2 50%minimal Hemodynamicallydistressventstable Mental statussupportchange Acute arrhythmiaResume prior vent settings24
Mar 11, 2020 · 2 Mortality Rates Of Viral Outbreaks 1918 – 1919 Influenza 10% 2002 – 2004 SARS 10% 2014 – 2017 MERS 37% 2019 – 2020 COVID-19 3.7% Influenza 2019-2020 Season COVID-19 mortality by