Transcription
Coding andPayment Guidewww.optumcoding.comFor the PhysicalTherapistAn essential coding, billing, and reimbursementresource for the physical therapist2016ICD-10A full suite of resources including the latest code set,mapping products, and expert training to help you makea smooth transition. www.optumcoding.com/ICD10
ContentsIntroduction .1Coding Systems .1Claim Forms .2Contents and Format of This Guide .2Sample Page and Key .3HCPCS Level II Definitions and Guidelines . 145Introduction . 145HCPCS Level II—National Codes . 145Structure and Use of HCPCS Level II Codes . 145HCPCS Level II Codes and the Physical Therapist . 147Procedure Codes .7Appropriate Codes for Physical Therapists .7Definitions and Guidelines: Procedures .9Medicare Official Regulatory Information . 165The CMS Online Manual System . 165Pub. 100 References . 165Correct Coding Initiative Update (21.3) .131Glossary . 187CPT Index .139Index . 195ICD-10-CM Index .141ICD-10-CM Coding Conventions . 141Coding Neoplasms . 142Manifestation Codes . 142Official ICD-10-CM Guidelines for Coding and Reporting . 142 2015 Optum360, LLC 2015 American Medical Association. All Rights Reserved.1
IntroductionCoding systems and claim forms are part of the reality of modernhealth care. This Coding and Payment Guide provides a comprehensiveexplanation of the coding and payment systems used by physicaltherapists. Organized by topics and by numerical procedure codelistings pertinent to physical therapy, it can be used as a coding as wellas a payment resource.Coding systems grew out of the need for data collection. By having astandard notation for the procedures performed and for the diseases,injuries, and illnesses diagnosed, statisticians could identify effectivetreatments as well as broad practice patterns. Before long, these earlycoding systems emerged as the basis to pay claims. Coding systemsand claim forms have evolved to become the basis of payment forhealth care services. The correct application of codes and knowledge ofpayer policies correlates directly to payment.The administrative simplification provisions of the Health InsurancePortability and Accountability Act (HIPAA) of 1996 required thestandardization of the several hundred health care claim formatspreviously in existence, as well as the establishment of standardizedcode sets for medical data including diagnoses, drugs, procedures,equipment, and supplies. The goal of the national standards is toreduce the administrative encumbrances of the existing system,simplify the way medical claims are paid, reduce costs, and promotethe growth of electronic business in the health care industry.Other mechanisms involved in getting paid may also includedocumentation of functional deficits, but any translation to a claimform would be payer specific.Coding SystemsCoding systems seek to answer two questions: what was wrong withthe patient (i.e., the diagnosis or diagnoses) and what was done totreat the patient (i.e., the procedures or services rendered).Under the aegis of the federal government, a three-tiered codingsystem emerged for health care providers and outpatient facilities. ThePhysicians’ Current Procedural Terminology (CPT ) codes reportmedical procedures and services and comprises Level I of the system. Asecond level, known as HCPCS Level II codes, are mainly used toidentify products, supplies, and services that are not included in theCPT codes. Dovetailing with each of these is the InternationalClassification of Diseases, 10th Revision, Clinical Modification(ICD-10-CM) classification system that reports the diagnosis ofillnesses, diseases, and injuries.Further explanations of each of these coding systems follows.HCPCS Level I or CPT CodesCMS, in conjunction with the American Medical Association (AMA), theAmerican Dental Association (ADA), and several other professionalgroups developed, adopted, and implemented a coding systemdescribing services rendered to patients. Known as HCPCS Level I, theCPT coding system is the most commonly used system to reportprocedures and services. Copyright of CPT codes and descriptions isheld by the AMA. This system reports outpatient and provider services.CPT codes predominantly describe medical services and procedures,and are adapted to provide a common billing language that providers 2015 Optum360, LLCand payers can use for payment purposes. The codes are required forbilling by both private and public insurance carriers, managed carecompanies, and workers’ compensation programs.The AMA’s CPT Editorial Panel reviews the coding system and adds,revises, and deletes codes and descriptions. The panel acceptsinformation and feedback from providers about new codes andrevisions to existing codes that could better reflect the providedservice or procedure. The American Physical Therapy Association(APTA) is represented on the Health Care Professional AdvisoryCommittee (HCPAC) for both the AMA CPT Editorial Panel and the AMARelative Value Update Committee (RUC). The CPT HCPACrepresentative provides input for the development and revision of CPTcodes, while the RUC HCPAC representative provides input into theestablishment of relative values for the codes.The majority of codes are found in category I of the CPT coding system.These five-digit codes describe procedures and services that arecustomarily performed including those performed by the physicaltherapist.CPT category II codes are supplemental tracking codes that areprimarily used when participating in the Physician Quality ReportingSystem (PQRS) established by Medicare and are intended to aid in thecollection of data about quality of care. Category II codes arealphanumeric, consisting of four digits followed by an F and shouldnever be used in lieu of a category I CPT code. A complete list of thecategory II codes can be found at the AMA website g-insurance/cpt/about-cpt/category-ii-codes.page. More information regarding the PQRS can befound on the CMS website at tient-Assessment-Instruments/PQRS/index.html, and at http://www.apta.org/pqrs.Category III of the CPT coding system contains temporary trackingcodes for new and emerging technologies that are meant to aid in thecollection of data on these new services and procedures as well asfacilitate the payment process. However, it should be noted that fewpayers reimburse for emerging technology procedures and services.CPT category III codes consist of four numeric digits followed by a T.Like category II codes, category III codes are released twice a year(January 1 and July I) and can be found on the AMA CPT website insurance/cpt/about-cpt/category-iii-codes.page. RVUs are notassigned for category III codes and payment is made at the discretionof the payer. A service described by a CPT code may eventually becomea category I code, as the efficacy and safety of the service isdocumented and as the category II codes are sunsetted after five yearsand then must be reviewed for continued use as category IIIdescriptors.ICD-10-CM CodesIn response to ICD-9-CM’s shortcomings, new coding systems weredeveloped and soon will be implemented in the United States. TheWorld Health Organization (WHO) created and adopted ICD-10 in 1994and it has been used in much of the world since then. This system is thebasis for the new U.S. diagnosis coding system, International 2015 American Medical Association. All Rights Reserved.1
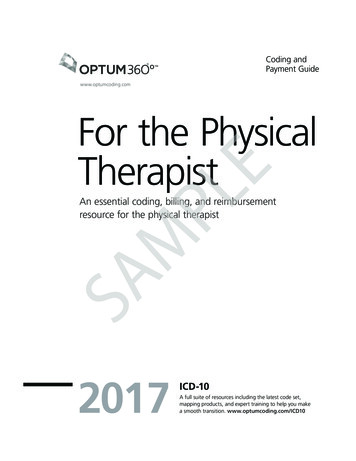
Coding and Payment Guide for the Physical TherapistProcedure Codes16020-16030rule of nines. Rapid measurement system used to calculate the total body surface16020Dressings and/or debridement of partial-thickness burns, initialor subsequent; small (less than 5% total body surface area)16025medium (eg, whole face or whole extremity, or 5% to 10%total body surface area)16030large (eg, more than 1 extremity, or greater than 10% totalbody surface area)ExplanationThe qualified health care provider applies dressing material(s) and/or debridesa partial-thickness burn of blisters and nonviable or nonadherent tissue, initialor subsequent. The qualified health care provider removes devitalized tissueor tissue that is contaminated by bacteria, foreign material, dead cells, or acrust as allowed within the state scope of practice. The wound is cleansed anda dressing is applied. Report 16020 for treatment of a small burn area, lessthan 5 percent of total body surface area; 16025 for a medium-sized area, 5to 10 percent of total body surface area, such as the whole face or a wholeextremity; and 16030 for a large burn area, greater than 10 percent of totalbody surface area, such as more than one extremity.Coding TipsCode selection is determined by the total body area. The Rule of Nines is usedto estimate the percentage of body surface burned. It is appropriate to use acode from this range to report a dressing of a wound that has been describedas blistered, nonviable skin.area (TBSA) involved in burns, based upon dividing the total area into segments asmultiples of 9 percent. The perineum or external genitals are 1 percent; each arm is 9percent; the front and back of the trunk, and each leg are separately counted as 18percent; and the head is another 9 percent in adults. For infants and children, the headis 18 percent involvement and the legs are 14 percent each, due to the larger surfacearea of a child's head in proportion to the body.ICD-10-CM Diagnostic CodesThe application of this code is too broad to adequately present ICD-10-CMdiagnostic code links here. Refer to your ICD-10-CM book.Medicare Edits160201602516030Fac RVUNon-Fac )1(3)Modifiers1602051N/A1602551N/A1603051N/A* with documentationN/AN/AN/AMedicare ReferencesN/AN/AN/ANoneBefore assigning a code from this section of the CPT book, see also codes97597–97606.Documentation TipsDocumentation supporting the medical necessity of these procedures includes:Activities, positioning, and postures that aggravate the wound or scaror that relieve symptomsPercentage of total body surface area (TBSA) involved and the depthof the burnSigns of infectionWound characteristicsWound scar tissue characteristicsReimbursement TipsDressing and debridement of burns, codes 16020–16030, are often consideredminor surgical procedures by third-party payers. Check in advance with thepayer and follow payer-specific guidelines regarding the billing of minorsurgical procedures. The type of dressing material used does not determinethe selection of the appropriate code assisted.Use of these codes by physical therapists can be problematic because payersrecognize that physical therapists do not perform surgical procedures.However, particularly for patients with burn wounds, some codes found inthe Surgery section of the CPT book do apply to physical therapists (16020,16025, and 16030) and should be used when appropriate.Terms To Knowdebridement. Removal of dead or contaminated tissue and foreign matter froma wound.dressing. Material applied to a wound or surgical site for protection, absorption, ordrainage of the area. 2015 Optum360, LLCCPT 2015 American Medical Association. All Rights Reserved.11
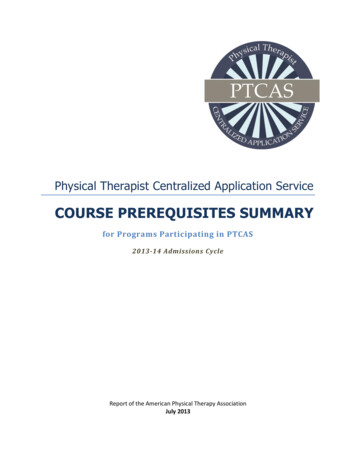
Procedure CodesCoding and Payment Guide for the Physical Therapist29505-2951529505Application of long leg splint (thigh to ankle or toes)29515Application of short leg splint (calf to foot)Under the RBRVS payment methodology, supplies that typically are used inthe delivery of a service (such as electrodes) have been included in thecalculation of the practice expense value for the code and should not be billedseparately.Terms To KnowExplanationsplint. Brace or support. 1) dynamic splint: brace that permits movement of anIn 29505, the qualified health care provider applies a long leg splint from thighto the ankle or toes. A long leg posterior splint is used to immobilize a numberof injuries around the knee or ankle. The qualified health care provider wrapscotton bandaging around the involved leg from the upper thigh to the ankleor toes. Plaster strips or fiberglass splint material are applied along the posterioraspect of the leg from the upper thigh to the ankle or toes. After the splintmaterial dries, it is secured into place by an Ace wrap. In 29515, the qualifiedhealth care provider applies a short leg splint from calf to foot. A short legsplint is used to immobilize the ankle. The qualified health care provider wrapscotton bandaging from just below the knee to the toes. Plaster strips orfiberglass splinting material are applied to the posterior of the calf, aroundthe heel, and along the bottom of the foot to the toes. After the splint materialdries, it is secured into place by an Ace wrap.Coding TipsThe code for the initial treatment of a fracture or dislocation includes theapplication, maintenance, and removal of the first cast or traction. SeeApplication of Casts and Strapping in the CPT book in the Surgery section,under Musculoskeletal System. Splint supplies are reported separately, seeHCPCS Level II codes.According to CPT guidelines, cast application or strapping (including removal)is only reported as a replacement procedure or when the cast application orstrapping is an initial service performed without a restorative treatment orprocedure. See Application of Casts and Strapping in the CPT book in theSurgery section, under Musculoskeletal System.Documentation TipsThe anatomical location, as well as the condition necessitating the treatment,should be clearly identified in the medical record.A dislocation is the traumatic displacement of the bones in any articulatingjoint severe enough to lose normal anatomic relationship. A dislocation(luxation) occurs when the bones completely lose contact with their articulatingsurfaces. A subluxation occurs when there is only a partial loss of contact.Closed dislocation is described by terms such as complete, NOS, partial, simple,and uncomplicated. Open dislocation is described by terms such as compound,infected, and with foreign body. Dislocations not specified as open or closedshould be classified as closed.A sprain is a complete or incomplete tear in any one or more of the ligamentsthat surround and support a joint. A strain is an ill-defined injury caused byoveruse or overextension of the muscles or tendons of a joint.Reimbursement Tipsanatomical structure such as a hand, wrist, foot, or other part of the body after surgeryor injury. 2) static splint: brace that prevents movement and maintains support andposition for an anatomical structure after surgery or injury.ICD-10-CM Diagnostic 61M66.862S97.01XAS97.02XARecurrent dislocation of patella, right kneeRecurrent dislocation of patella, left kneeRecurrent subluxation of patella, right kneeRecurrent subluxation of patella, left kneeChondromalacia patellae, right kneeChondromalacia patellae, left kneeChronic instability of knee, right kneeChronic instability of knee, left kneeRecurrent dislocation, right kneeRecurrent dislocation, left kneeEffusion, right kneeEffusion, left kneeSpontaneous rupture of flexor tendons, right lower legSpontaneous rupture of flexor tendons, left lower legSpontaneous rupture of other tendons, right lower legSpontaneous rupture of other tendons, left lower legCrushing injury of right ankle, initial encounterCrushing injury of left ankle, initial encounterPlease note that this list of associated ICD-10-CM codes is not all-inclusive.The procedure may be performed for reasons other than those listed thatsupport the medical necessity of the service. Only those conditions supportedby the medical record documentation should be reported.Medicare EditsFac RVUNon-Fac 515Modifiers295055150295155150* with documentationN/AN/AMedicare ReferencesN/AN/ANoneThe multiple procedure payment reduction (MPPR) policy applies to thisservice. Under MPPR, when multiple “always therapy” procedures are renderedto the same patient on the same date of service (even in separate sessions),the procedure with the highest practice expense value that day is paid at 100percent, and the practice expense component of the second and subsequenttherapy services is paid at 50 percent. The work and malpractice componentsof the therapy service payment are not reduced. For payers other thanMedicare, the amount of the reduction may vary by payer and by insuranceplan.18CPT 2015 American Medical Association. All Rights Reserved. 2015 Optum360, LLC
Coding and Payment Guide for the Physical TherapistProcedure Codes29520-2955029520therapy services is paid at 50 percent. The work and malpractice componentsof the therapy service payment are not reduced. For payers other thanMedicare, the amount of the reduction may vary by payer and by insuranceplan.Strapping; hip29530knee29540ankle and/or foot29550toesUnder the RBRVS payment methodology, supplies that typically are used inthe delivery of a service (such as electrodes) have been included in thecalculation of the practice expense value for the code and should not be billedseparately.ExplanationThe qualified health care provider uses tape to strap a lower extremity. Tapingof the hip for immobilization is rarely used because of the hip muscles' superiorstrength to that of the tape. A hip spica taping procedure may be used to holdanalgesic packs in place and to offer mild support to injured hip adductors orflexors. The patient stands with all weight on the unaffected leg. Six inch Acewrap is usually used. The end of the wrap begins at the upper part of the thighand immediately encircles the upper thigh and groin, crossing the startingpoint. When the starting end is reached the roll is taken completely aroundthe waist and fixed firmly above the iliac crest. The wrap is carried around thethigh at groin level and up again around the waist. The end is secured withtape. Report 29520 if the site taped is the hip. Report 29530 if the site tapedis the knee. Code 29540 is reported when the site taped is the ankle or foot,and code 29550 if the site is the toes.Coding TipsAccording to CPT guidelines, cast application or strapping (including removal)is only reported as a replacement procedure or when the cast application orstrapping is an initial service performed without a restorative treatme
Use of these codes by physical therapists can be problematic because payers recognize that physical therapists do not perform surgical procedures. However, particularly for patients with burn wounds, some codes found in the Surgery section of the CPT book do apply to physical therapists (1602