Transcription
BUSINESS PROCESS REENGINEERING AT THE HOSPITALS:A CASE STUDY AT SINGAPORE HOSPITALArun Kumar and Linet OzdamarSchool of Mechanical & Production EngineeringNanyang Technological University50 Nanyang Avenue, SINGAPORE-639798Email: makumar@ntu.edu.sgKEYWORDSBusiness process reengineering, Healthcare.ABSTRACTAs health care costs increase, there is a need forhealthcare service providers to look for ways tocontain costs and to achieve a higher efficiency attheir operating facilities without sacrificingquality. This paper studies a case in employingbusiness process reengineering techniques on oneaspect of a health care service – surgical work.The system is simulated focusing on the processesthat contribute to the effective functioning of anoperating theatre.INTRODUCTIONBusiness process reengineering (BPR) hasbecome increasingly important in recent years.Customers now have the choice of differentproduct and service providers, to provide themwith the same core product or service that theywant. Over the last fifteen years, companies havebeen forced to reengineering their businessprocesses to stay competitive because customersare demanding better products and services.Improving and redesigning business processes isparamount for businesses to stay competitive.With the escalating health care costs, healthcareservice providers in Singapore are alsocontinuously seeking ways to stay competitiveand provide quality service to the customers.Little research has been done on the employmentof BPR in healthcare systems. Healthcare industryhas traditionally emphasized on breakthroughs inoperating procedures and technology in the bid tostay competitive. Healthcare service providers arebeginning to understand that BPR initiativescould be a better solution to achievingcompetitive advantage.The operating theatre suite is a criticallyimportant segment of any healthcare organizationProceedings 18th European Simulation MulticonferenceGraham Horton (c) SCS Europe, 2004ISBN 3-936150-35-4 (book) / ISBN 3-936150-36-2 (CD)that delivers surgical care to patients. It canconsume multitudes of resources, but at the sametime can generate significant revenue if managedproperly. The conflict between the national goalof healthcare and the high cost of surgicaloperations is a powerful incentive to improve thequality of management of the surgical suite. Forthis reason, many hospitals are reengineering theiroperating theatre processes in an effort toestablish, restore or boost profitability whileretaining quality (Harris and Zitzmann 1998;Gabel et al. 1999). Reengineering techniquesenable healthcare service providers to take acareful look at the processes involved within theorganization, identifying redundancy andinefficiency that can be removed from the system.This research employs the concept of BPR toimprove the efficiency and effectiveness ofcertain processes involved in surgical operations.This paper intends to explore the possibilities ofcost containment/reduction in a particular aspectof the healthcare industry with the application ofBPR. A simulation model has been formulated toreduce any inefficiencies or bottlenecks inherentin the system under study. The scope of thisresearch is limited to an operating theatre suitewithin a hospital.LITERATURE REVIEWThe aggregate per capita healthcare expenditurein Singapore has risen consistently for the lastthree decades from about S 150 in the 1960s toS 800 in the 1997 (Tan and Chew 1997). Thehealthcare industry in Singapore, like its globalcounterparts, has been facing tremendouspressures since the turn of the last century. Thechallenges faced by the industry in the near futureare as follows.The accelerated population ageing will haveserious implications to the provisions of healthcare for the elderly population who will occupy
most of the hospital beds with a low turnover rate.Moreover, the entry of more private-sectorhospitals and medical service will lead to ls (Zhang 2001).There is a lack of health care professionals inSingapore. The local doctor-to-patient ratio was140 doctors for every 100,000 of the populationfor the year 2000. According to OECD data, theaverage ratios for the decade of the '90s forAustralia and New Zealand were 240 and 218respectively (Wee 2002).Business Process Reengineering in HealthcareManagers use process reengineering methods todiscover the best processes for performing work,and that these processes be reengineered tooptimize productivity (Weicher et al. 1995).Hammer and Champy (1993) state that BPRrefers to the fundamental rethinking and radicalredesign of business processes to achievedramatic improvements in critical, contemporarymeasures of performance, such as cost, qualityand speed. Business processes are sequences andcombinations of activities that deliver value to acustomer (Coulson-Thomas 1996). A corebusiness process usually creates value by thecapabilities it gives the company forcompetitiveness. A limited number of such corebusiness processes can be identified in anycompany, and enhancing those processes can leadto business improvement.Over the last few years, the reengineering concepthas evolved from a "radical change" to accountfor the contextual realism (Caron et al. 1994, Earl1995). Davenport and Short (1990) prescribe afive-step approach to BPR. They argue thatprocess reengineering requires taking a broaderview of both IT and business activity, and of therelationships between them. The rhetoric of BPRalso encourages fundamental step, or framebreaking change (Coulson-Thomas 1996). BPR isincreasingly recognized as a form oforganizational change characterized by strategictransformation of interrelated organizational subsystems producing varied levels of impact. Thisorganizational change perspective recognizes thatbusiness process reengineering is not a monolithicconcept but rather a continuum of approaches toprocess change (Kettinger et al. 1997). The fasterthe speed of change the more difficult andstressful it is to manage (Edwards and Walton1996).With 80 percent of the expenses tied to patientcare activities, hospitals and healthcare systemscan garner substantial savings and improveclinical practices by better managing their labor,supplies, equipment, and facilities. The benefitsof reinventing hospitals hold the tangible andrealistic promise of radically reducing cost whiledramatically increasing the quality of careprovided (Harmon 1996).A case study at Karolinska Hospital in Sweden byJacob (1995), and Hout and Stalk (1993) revealsthat rising costs and a weakened economy in1990s were forcing the government to reassessand reduce health care expenditures. KarolinskafollowedBoston Consulting Group’s (BCG)Time-Based Management methods to reengineerthe way work was done. BCG reorganized workat the hospital around patient flow by creating anew position of "nurse coordinator" in mostdepartments. By redesigning operating proceduresand staffing patterns, Karolinska was able to cutthe time required for preoperative testing frommonths to days, close 2 of 15 operating roomsand still increase the number of operations perday by 30 percent.Operating theatre management often involveshuman resources, information systems, finance,physical plant design and utilization, capitalequipment, clinical quality and efficiency andregulatory(Merriam-Webster2002).Furthermore, surgical cases are conventionallyclassified into elective and emergency. Anelective case is one whereby the patient can waitat least three days without sustaining morbidity ormortality. A surgical group comprises of severalsurgeons who share allocated operating theatretime. The term block time is the time allocated toeach surgical group into which only the surgeonsbelonging to that surgical group can scheduletheir patients.Managing operating theatre suites is a difficulttask, because individual theatres and the entiresuite are highly complex and tense environments.Many personnel working in the suite are notunder the direct control of the operating theatremanager. The operating theatre schedule sets thestage for the daily flow of patients and staff. Oncethe day starts, however, deviations from thisschedule are frequent and expected. Emergencycases must be accommodated, cases may belonger or (rarely) shorter than scheduled, patientsmay be late or fail to arrive at all, and personnel
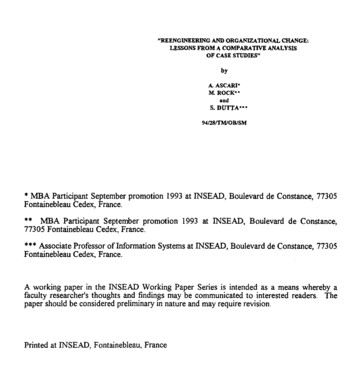
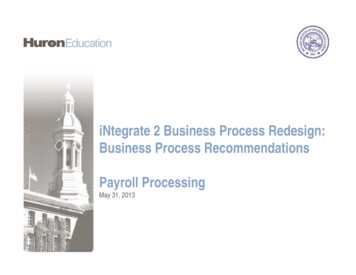
may call in sick or become ill during the course ofthe day (Gabel et al. 1999).Modern operating theatre management requiresan information system that includes an effectivescheduling system. Such a system has two basicbut critical functions: performing the actualscheduling of cases, which involves finding outthe time available on the schedule, whether thattime occurs in a surgeon’s specific block time,and to facilitate intelligent management ofresources. It must provide data on how resourcesare being used in relation to their availability(Harris et al. 1998). Block scheduling assigns asurgeon (or a surgical group) a block of time thatis exclusively for his cases.The anaesthesia service is often a separatedepartment; in some hospitals it is a divisionunder surgery department. In contrast withsurgical sub-specialties, anaesthetists specializingin specific clinical areas such as pediatricanaesthesia, obstetric anaesthesia and cardiacanaesthesia are not typically organized intodistinct departments. The anaesthesia departmentmust be organized in such a way as to ensureavailability of a sufficient number of anaesthesiaproviders for elective and emergency cases,which requires 24-hour-a-day coverage (Gabel etal. 1999).Simulation in the Health Care IndustryThe health care industry is a dynamic system withcomplex interactions, in which the simulationtechnique would play an indirect but vital role toachieve the optimal result (Zhang 2001). Keltonet al. (1998) state that the real power of thesimulation technique is fully realized when it isused to study a complex system. Numeroushealthcare service providers such as D. R.Hospital in North Carolina, and St John Hospitalin Detroit, U.S.A. have successfully employed thesimulation technique to help them inunderstanding their processes and to optimizethem (ProModel Corporation 2002).CASE STUDYThe Department of Surgery at the SingaporeHospital oversees the operations of the surgicaltheatres. The main operating theatre complex atBlock 3 of the hospital grounds is where surgicaloperations of different specialties take place. Thelocal demand for surgery services has increasedover the last two decades. The capacity of theoperating theatres at the complex has reachedhigh levels of utilization, and action is necessaryto ensure that the department is able to cope withincreasing patient load. Due to the increasingdemand by patients on the services provided bythis operating theatre complex and the acuteshortage of manpower in the local health careindustry, the Department of Surgery has toemploy reengineering practices to achieve moreefficient and effective utilization with its existingresources.There are a total of 21 operating theatres at themain OT complex at Block 3 of the hospital. Inthe year 2000, the number of surgical operationsconducted at the hospital was 59,377, of whichabout 45% were outpatient (day) surgeries. Thedaily average was 162. Out of the 21 theatres, 19are allocated for elective surgery and operate 8hours a day (from 8:30 to 17:30), and theremaining 2 are employed as emergencyoperating theatres and operate 24 hours a day.Historical data was extracted from the hospital’sscheduling database for the period January toSeptember 2001. The data includes the percentageutilization of all the operating theatres, and thesurgeons’ log of all the surgical operationsconducted within the same period.Every day, each operating theatre is reserved for aspecific clinical discipline to carry out surgicaloperations. Some of the operating theatres areexclusively reserved for a particular discipline,whereas others may be used by differentdisciplines for each day of the week.MODELING OF THE OPERATINGTHEATRE COMPLEXMedModel is a simulation-based powerfulsoftware tool for evaluating, planning or redesigning hospitals and other healthcare systems.It provides a basis for the comprehensiveevaluation of large and complex health caresystems. MedModel is also equipped with animpressive collection of pre-programmedconstructs. Before a model for the operatingtheatre complex can be developed, a flow chart ofthe operating theatre process is provided in Figure1 to illustrate the entities, resources and locationsinvolved. Figure 2 shows the layout of thecompleted simulation model. The proportion ofelective surgical operations for each clinicaldiscipline varies greatly.To keep simulation as simple as possible, thismodel deals with only 8 operating theatres, each
sat entrancePre-opPatientPatientwaitsat pre-opareaOTPatientPatient issummonedwhen OTis readyOTGurneyPatientPatient isescorted toOT by igure 1: Flow Chart of the Operating Theatre ProcessOTSetupOT isset up whenavailableRecoveryGurneyPatientPatient isescorted toRecoveryby gurneyExitPatientPatient exitssystem
Figure 2: Layout of Completed Simulation ModelTable 1: Patient Types and DistributionPatient TypeClinical codePercentage(%)Surgery required1CLR12Colorectal surgery2CTS6Cardiothoracic surgery3ENT9Ear, nose and Throat surgery4GES26General surgery5GYN11Obstetrics and gynaecology6OTHERS9Other surgery7OTO22Orthopaedic surgery8PLS5Plastic surgery
reserved for a different category of surgery. Assuch, the number of entities and resources used inthis model will be scaled down from the real-lifenumbers obtained. There are 2 entities in thissimulation model, namely Patient and Setup. Inaccordance with the 8 categories of surgical cases,the patient is classified into 8 different typesusing the attribute aPt Type and the user-defineddistributio
quality. This paper studies a case in employing business process reengineering techniques on one aspect of a health care service – surgical work. The system is simulated focusing on the processes that contribute to the effective functioning of an operating theatre. INTRODUCTION Business process reengineering (BPR) has become increasingly important in recent years.