Transcription
Nevada Advanced Practice Nurses AssociationMarch 7, 2017RE: NAPNA OPPOSED TO SB 210 (ANESTHESIOLOGY ASSISTANT BILL)Dear Esteemed Nevada Legislators:NAPNA is an organization representing more than 1,500 autonomous advanced practice registered nurses (APRNs)focused on improving access to health care for all Nevadans. This access includes the caveat that the health careprovided be high quality, safe, cost-effective, and evidence-based. The use of anesthesiology assistants (AAs) hasnot been proven to be safe, does not reduce health care costs, and does not improve access to anesthesia servicesin the rural or urban underserved areas where physician anesthesiologists do not practice.NAPNA has submitted PowerPoint slides for the record and this testimony is meant to complement the compellingdata they contain. Certified registered nurse anesthetists (CRNAs) are found in 9 out of 17 Nevada counties, and 5of those counties rely solely on CRNAs as their anesthesia provider (Office of Statewide Initiatives, 2016). Whilethere are about 5 times more physician anesthesiologists than CRNAs in Nevada, they are found predominantly inthe urban areas and in fact, urban per capita anesthesiologists exceed the national average (Office of StatewideInitiatives, 2016). Unlike most other types of health care providers, there is no shortage of physiciananesthesiologists in Nevada or the western portion of the United States.Other than the fact that CRNAs are already found in the rural areas, why should Nevada look to CRNAs rather thanAAs to improve access to anesthesia care? CRNAs are the most cost-effective model for anesthesia delivery (Hoganet al, 2016). Data shows no conclusive difference in outcomes between physician anesthesiologists and CRNAsworking individually or together as a team (Dulisse & Cromwell, 2010). CRNAs practice safely and autonomouslywith the same case mix as anesthesiologists (Hogan et al, 2010). CRNAs are full scope anesthesia providers whoare equivalent in function, scope, and outcomes as physician anesthesiologists.There is no comparison between CRNAs and AAs. AAs are trained only to assist physician anesthesiologists intechnical functions. By proposing to allow AAs to administer spinals and epidurals, including the placement ofregional blocks, SB 210 exceeds the scope of practice typically associated with AAs unless the physiciananesthesiologist is physically present in the room, in which case the proven anesthesia provider, the physiciananesthesiologist, should perform the procedure and negates the need for an AA to do so. As the AA is limited bysetting and geography due to the requirement for immediate anesthesia supervision availability, they cannotaddress access issues in rural and underserved areas.There is no data to show the use of AAs is cost effective. AA supervision lapses are known to be common with firstcase starts even with 1:2 supervision ratio (Epstein & Dexter, 2010) and SB 210 calls for 1:4 supervision ratio.Safety of Nevadans is of utmost importance, and although AAs have been around almost as long as nursepractitioners, there are NO published, peer-reviewed, evidence-based safety and outcomes data. Do we want toEXHIBIT P Senate Committee on Commerce Labor and EnergyDate:3-8-2017Total pages: 15 Exhibit begins with: P1thru P15
experiment on Nevadans with unproven, unsafe providers under a physician "supervision" model that consistentlyhas lapses?NAPNA believes Nevadans deserve the best anesthesia care, which means the 1:1 interaction and attention of aCRNA or physician anesthesiologist who can provide autonomous, full scope anesthesia care. Using AAs with noproven safety or track record will create a two-tiered system for the underserved and underprivileged population.CRNAs and physician anesthesiologists are the best choice for Nevada, not AAs.NAPNA would like to collaborate with the Nevada legislature in developing sustainable evidence-based solutions tohealth care issues. In regards to improving access to anesthesia services in the rural and urban underservedportions of the state, NAPNA recommends against utilizing an unproven, unsafe, dependent provider and toinstead increase the utilization of CRNAs and create a favorable practice environment through policies supportingthe hiring of CRNAs and CMA opt-out for hospitals. By encouraging out-of-state CRNAs to train in Nevada andincreasing CRNA recruitment from states with a surplus, Nevada can simultaneously address the autonomousanesthesia provider pipeline issue and build up the rural workforce.Thank you for your time and consideration.Respectfully yours,\/.///NlarA NP-BC, CCRN-CMC, PHNDr. ean-ne S ygNAPNA Presidentiswygmanpnapna.netReferences Amburgey, B., Kentucky. General Assembly. Legislative Research Commission., . (2007). A study ofanesthesiologist assistants. Frankfort, Ky.: Legislative Research Commission. Dulisse, B., & Cromwell, J. (2010). No harm found when nurse anesthetists work without supervision byphysicians. Health Affairs, 29(8), 1469-1475. http://dx.doi.org/10.1377/hlthaff.2008.0966 Epstein, R. H., & Dexter, F. (2012). Influence of supervision ratios by anesthesiologists on first-case startsand critical portions of anesthetics. Anesthesiology, 116(3), ec24 Hogan, P. F., Seifert, R. F., Moore, C. S., & Simonson, B. E. (2010). Cost effective analysis of anesthesiaproviders. Nursing Economics, 28(3), 159-169. Retrieved nts/nec mi 10 hogan.pdf Office of Statewide Initiatives. (2016). Nevada Instant Atlas [County-level health workforce and populationhealth database]. Retrieved from http://med.unr.edu/statewide/instant-atlasP2
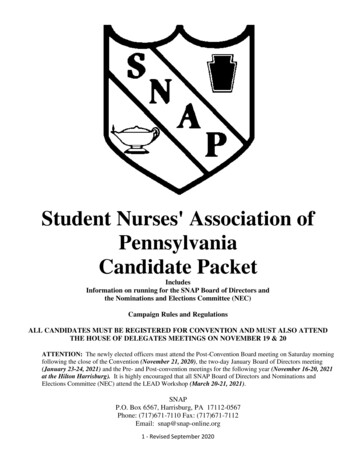
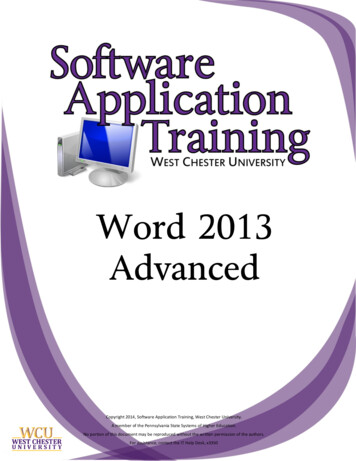
3/7/2017Nevada' Advanced Practice Nurses AssociationCRNAs: Anesthesia ProviderAccess Solution for NevadaDr. Jeanine Swygman DNP, ACNP-BC, CCRN-CMC, PHNNAPNA PresidentExhibit in Opposition to SB 210March 8, 2017Where CRNAs Practice in NVCRNAs in 9 of 17 counties5 CRNA only counties— Carson City (1)— Churchill— Churchill (5)— Elko— Clark (71)— Humboldt— Douglas (1)— Nye— Elko (6)— White Pine— Humboldt (2)TOTAL: 15 (16% ofCRNAs)— Nye (1)— Washoe (6)— White Pine (1)(Office of Statewide Intbatives, 2016)— TOTAL: 94P31
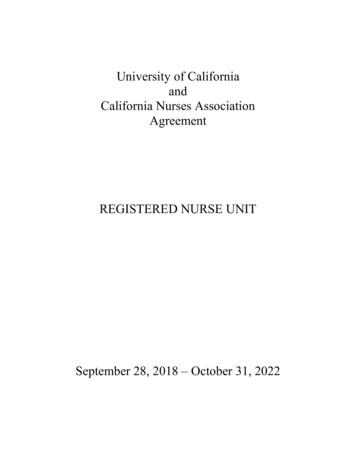
3/7/2017Where Anesthesiologists Practice inNV Anesthesiologists Out of 464anesthesiologists in thepractice in 4 counties— Carson City (17)state, only 3 are in the— Clark (337)rural & frontier areas— Douglas (3) Anesthesiologist only— Washoe (107)counties— NONE Urban per capitaanesthesiologistsexceeds nationalaverage(Office of Statewide Initiatives, 2016)CRNA Numbers10090807060State50 Rural & Frontier403020102006 2008 2010 2012 2014 2016(Office of Statewide Initiotive, 2016)P42
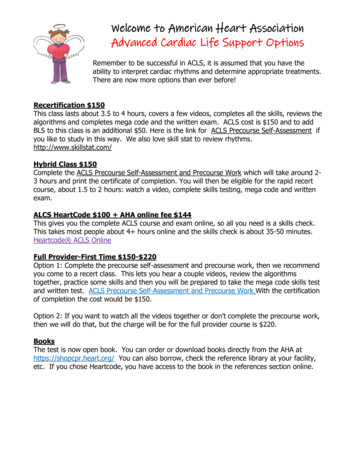
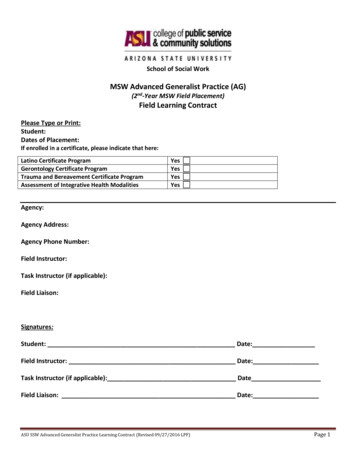
3/7/2017CRNAs per 100,000 PopulationChart ural & Frontier sia Urban U.S.(Office of Statewide Initiatives, 2016)Anesthesiologists per 100,000Population2015201816141210 201586420StateUrbanRural & FrontierU.S.(Office of Statewide Initiatives, 2016)3P5
3/7/2017Why CRNAs? CRNAs as sole anesthesia provider is most costeffective model for anesthesia delivery (Hogan et al, 2016)— No difference in complications from anesthesiologists(Dulisse & Cromwell, 2010) CRNAs practice safely and autonomously withsame case mix as anesthesiologists—Can perform the same set of anesthesia servicesincluding open heart surgeries, organ transplantationsand pediatric procedures (Hogan et al, 2010)Why CRNAs? Qualified to make independent judgementsregarding all aspects of anesthesia care basedon education, licensure, and certification Can work in diverse settings throughout state— Urban, underserved, rural and frontier— Every setting: hospital surgical suites; obstetricaldelivery rooms; critical access hospitals;ambulatory surgical centers; offices of dentists,podiatrists, ophthalmologists, plastic surgeons;DOD & VA healthcare facilitiesP64
3/7/2017CRNAs are equivalent in function,scope, and outcomes toanesthesiologists.There is no comparison betweenCRNAs and AAs.AAs Will Not Benefit NV Not a full service anesthesia provider. SB 210 exceeds the scope of practice typically associatedwith AAs re: epidural & spinal anesthetic procedures,including placement of regional blocks unless theanesthesiologist is physically in the room— Limited value in obstetrics, pain management, orthopedics,and on-call Trained only to assist anesthesiologists in technicalfunctions. Limited to certain settings and geographic areasdependent on anesthesiologist supervision availability. Cannot meaningfully address access issues in rural andunderserved areas.P75
3/7/2017AAs Will Not Benefit NV Not cost effective— Requires two healthcare providers to provideanesthesia care to one patient— OR start times need to be staggered AA supervision lapses common during first casestarts even with 1:2 supervision ratio (Epstein & Dexter, 2012) Fails to adequately meet the needs of patientsand healthcare providers No published, peer reviewed, evidence-basedsafety and outcomes dataLack of Data on AA Safety No published, peer reviewed, evidence-basedsafety and outcomes data 2007: Kentucky Legislative ResearchCommission published "A Study ofAnesthesiologist Assistants"— Lack of data "limits the conclusions that can bemade about patient safety outcomes for AAs"(Amburgey, et al, 2007)P86
3/7/2017Lack of Data on AAs ImprovingHealthcare Access Kentucky Legislative Research Commissionnoted no studies involving AAs impact onaccess to care Any positive impact "may be limited due tothe requirement that anesthesiologistassistants practice under the directsupervision of anesthesiologists"(Amburgey, et al, 2007)Closed Claims Malpractice Data on AAs Suggested as a way to assess safety of AAs Closed claims malpractice data is used toidentify safety concerns in anesthesia,patterns of injury, and develop strategies ofprevention to improve patient safety Data is from malpractice insuranceorganization claim files Not appropriate data source for and has notbeen used to demonstrate AA safety(AANA Foundation Closed Malpractice Claims Database; www.asaclosedclaims.org)P97
3/7/2017Efficacy Argument for AAs: "Lack of data does notmean lack of efficacy" Merriam-Webster definition: the power toproduce an effect NO DATA on AA's safety, outcomes, impact onhealthcare access since 1969 LACK OF DATA LACK OF EFFICACY OF AAsChoice Anesthesiologists want a choice in providerslike surgical colleagues— Surgeons have choice between APRNs and PAs— Anesthesiologists have CRNAs, want AAs instead Why?P108
3/7/2017How AAs Fit Into a Business Model One anesthesiologist 1 case 100(example) One anesthesiologist supervises 4 AAs 100x 4 400—Assume 50% from each AA 200 Benefits to practice— Need less expensive anesthesiologists to take careof 4 times as many patients— Increases profitNevadans Deserve the Best inAnesthesia Care 1:1 interaction and attention of CRNA oranesthesiologist who can provide safe, fullscope anesthesiology care autonomously—AAs with no proven safety or outcomes trackrecord will create two-tier system for underservedand underprivileged population— Best choice for Nevadans is anesthesiologist andCRNAs, not AAsP119
3/7/2017VA Final Rule Effective 1/13/2017 NPs, CNS, CNM practicingunder the auspices of the VA will be grantedfull practice authority—CRNA exclusion "does not stem from the CRNAsinability to practice to the full extent of theirprofessional competence, but rather from VA'slack of access problems in the area ofanesthesiology"VA Final Rule Main argument against VA CRNAs was fullpractice authority would eliminate teambased concept of care— Established in VHA Handbook 1123, AnesthesiaService— Full practice authority does not eliminate teambased care(Federal Register § 38 CFR Part 17, 2016)10P12
3/7/2017VA Final Rule Second argument: "No shortage of physiciananesthesiologists in VA and the current systemallows for sufficient flexibility to address theneeds of all VA hospitals"— Noted that most of comments "not substantiatedby evidence" however "VA believes evidenceexists there is not currently a shortage ofanesthesiologists that critically impacts access tocare"(Federal Register § 38 CFR Part 17, 2016)Workforce Shortage Myth Per capita anesthesiologists exceeds nationalaverage September 2016: 13 CRNAs fired from largeanesthesiology practice in Las Vegas—Almost 15% of the state's CRNAs—Almost 20% of Clark county CRNAs AAs will displace not only CRNAs butanesthesiologistsP1311
3/7/2017Workforce Shortage Myth Monopolistic anesthesia employmentmarketplace does not allow flexibility to addressNevada's anesthesia access needs Most CRNAs un- and underemployed—Interest from CRNAs to move to NV if jobs available Need to maximize use of currently availableCRNAs to the fullest extent of their education,training and certification No evidence of need for AAs with an unproventrack recordAnesthesia Provider Demand National (as of 12/22/2016)— Anesthesiologists: 1664—CRNAs: 2298— AAs: 45 Nevada—Anesthesiologist: 17— CRNA: 4(Ga,vorLcon-412P14
3/7/2017Anesthesia Workforce Solutions Improve access to care by increasing utilization ofCRNAs in urban underserved and rural/frontierareas Address autonomous anesthesiology providerpipeline issue and build up rural workforce— Encourage training of CRNAs (instead of AAs) fromout-of-state— Increase recruitment from states with CRNA surplus(i.e. OR) Create favorable practice environment throughpolicies encouraging hiring CRNAs & CMS opt-outReferences Advanced Practice Registered Nurses, 81 Federal Register§ 38 CFR Part 17 (2016).Department of Veterans Affairs Amburgey, B., Kentucky. General Assembly. Legislative Research Commission.,.(2007). A study of anesthesiologist assistants. Frankfort, Ky.: Legislative ResearchCommission.Dulisse, B., & Cromwell, J. (2010). No harm found when nurse anesthetists workwithout supervision by physicians. Health Affairs, 29(8), 1469-1475. Epstein, R. H., & Dexter, F. (2012). Influence of supervision ratios byanesthesiologists on first-case starts and critical portions of anesthetics.Anesthesiology,11.6(3), 683-691. Hogan, P. F., Seifert, R. F., Moore, C. S., & Simonson, B. E. (2010). Cost effectiveanalysis of anesthesia providers. Nursing Economics, 28(3), 159-169. Retrievedfrom Office of Statewide Initiatives. (2016). Nevada Instant Atlas [County-level healthworkforce and population health database). Retrieved fromP1513
Data is from malpractice insurance organization claim files Not appropriate data source for and has not been used to demonstrate AA safety (AANA Foundation Closed Malpractice