Transcription
International Journal ofMedicine and MedicalSciencesVolume 5 Number 6 June 2013ISSN 2009-9723
ABOUT IJMMSThe International Journal of Medicine and Medical Sciences is published monthly (one volume per year) byAcademic Journals.The International Journal of Medicine and Medical Sciences (IJMMS) provides rapid publication (monthly) ofarticles in all areas of Medicine and Medical Sciences such as:Clinical Medicine: Internal Medicine, Surgery, Clinical Cancer Research, Clinical Pharmacology, Dermatology,Gynaecology, Paediatrics, Neurology, Psychiatry, Otorhinolaryngology, Ophthalmology, Dentistry, TropicalMedicine, Biomedical Engineering, Clinical Cardiovascular Research, Clinical Endocrinology, ClinicalPathophysiology, Clinical Immunology and Immunopathology, Clinical Nutritional Research, Geriatrics andSport MedicineBasic Medical Sciences: Biochemistry, Molecular Biology, Cellular Biology, Cytology, Genetics, Embryology,Developmental Biology, Radiobiology, Experimental Microbiology, Biophysics, Structural Research,Neurophysiology and Brain Research, Cardiovascular Research, Endocrinology, Physiology, MedicalMicrobiologyExperimental Medicine: Experimental Cancer Research, Pathophysiology, Immunology, Immunopathology,Nutritional Research, Vitaminology and EthiologyPreventive Medicine: Congenital Disorders, Mental Disorders, Psychosomatic Diseases, Addictive Diseases,Accidents, Cancer, Cardiovascular Diseases, Metabolic Disorders, Infectious Diseases, Diseases of Bones andJoints, Oral Preventive Medicine, Respiratory Diseases, Methods of Epidemiology and Other PreventiveMedicineSocial Medicine: Group Medicine, Social Paediatrics, Medico-Social Problems of the Youth, Medico-SocialProblems of the Elderly, Rehabilitation, Human Ecology, Environmental Toxicology, Dietetics, OccupationalMedicine, Pharmacology, Ergonomy, Health Education, Public Health and Health Services and Medical Statistics TheJournal welcomes the submission of manuscripts that meet the general criteria of significance andscientific excellence. Papers will be published approximately one month after acceptance. All articles published inIJMMS are peer-reviewed.Submission of ManuscriptSubmit manuscripts as e-mail attachment to the Editorial Office at: ijmms@academicjournals.org. A manuscriptnumber will be mailed to the corresponding author.The International Journal of Medicine and Medical Sciences will only accept manuscripts submitted as e-mailattachments.Please read the Instructions for Authors before submitting your manuscript. The manuscript files should begiven the last name of the first author.
EditorsAfrozul HaqEditor, Laboratory MedicineDepartment of Laboratory MedicineSheikh Khalifa Medical CityP.O. Box 51900, ABU DHABIUnited Arab Emirates
Editorial BoardChandrashekhar T. SreeramareddyDepartment of Community Medicine,P O Box No 155, Deep HeightsManipal College of Medical Sciences,Pokhara,NepalSisira Hemananda Siribaddana259, Temple Road, Thalapathpitiya,Nugegoda, 10250Sri LankaProfessor Viroj WiwanitkitWiwanitkit House, Bangkhae,BangkokThailand 10160Dr. Srinivas KoduruDept of Clinical SciencesCollage of Health SciencesUniversity of KentuckyLexington USADr. santi M. MandalInternal MedicineUTMB, Galveston, TX,USAWeiping ZhangDepartment of Oral BiologyIndiana University School of Dentistry1121 West Michigan Street, DS 271Indianapolis, IN 46202USAKonstantinos TziomalosDepartment of Clinical Biochemistry(Vascular Prevention Clinic),Royal Free Hospital Campus,University College Medical School, University CollegeLondon, London,United KingdomLisheng XUHo Sin Hang Engineering BuildingDepartment of Electronic EngineeringThe Chinese University of Hong KongShatin, N.T. Hong Kong,ChinaCyril Chukwudi DimDepartment of Obstetrics & GynaecologyUniversity of Nigeria Teaching Hospital (UNTH)P.M.B. 01129, Enugu. 400001,NigeriaDr. Mustafa SahinDepartment of Endocrinology and MetabolismBaskent University,Ankara,TurkeyMojtaba SaloutiSchool of Medical and Basic Sciences,Islamic Azad University- Zanjan,IranDr. Harshdeep JoshiMaharishi MarkandeshwarInstitute of Medical Sciences and ResearchAmbala, (Haryana).India.Imtiaz Ahmed WaniSrinagar Kashmir, 190009,India
Instructions for AuthorElectronic submission of manuscripts is stronglyencouraged, provided that the text, tables, and figures areincluded in a single Microsoft Word file (preferably in Arialfont).The cover letter should include the corresponding author'sfull address and telephone/fax numbers and should be inan e-mail message sent to the Editor, with the file, whosename should begin with the first author's surname, as anattachment.Article TypesThree types of manuscripts may be submitted:Regular articles: These should describe new and carefullyconfirmed findings, and experimental procedures should begiven in sufficient detail for others to verify the work. Thelength of a full paper should be the minimum required todescribe and interpret the work clearly.Short Communications: A Short Communication is suitablefor recording the results of complete small investigations orgiving details of new models or hypotheses, innovativemethods, techniques or apparatus. The style of mainsections need not conform to that of full-length papers.Short communications are 2 to 4 printed pages (about 6 to 12manuscript pages) in length.Reviews: Submissions of reviews and perspectives coveringtopics of current interest are welcome and encouraged.Reviews should be concise and no longer than 4-6 printedpages (about 12 to 18 manuscript pages). Reviews are alsopeer-reviewed.Review ProcessAll manuscripts are reviewed by an editor and members ofthe Editorial Board or qualified outside reviewers. Authorscannot nominate reviewers. Only reviewers randomlyselected from our database with specialization in thesubject area will be contacted to evaluate the manuscripts.The process will be blind review.Decisions will be made as rapidly as possible, and thejournal strives to return reviewers’ comments to authors asfast as possible. The editorial board will re-reviewmanuscripts that are accepted pending revision. It is thegoal of the IJMMS to publish manuscripts within weeksafter submission.Regular articlesAll portions of the manuscript must be typed doublespaced and all pages numbered starting from the titlepage.The Title should be a brief phrase describing thecontents of the paper. The Title Page should include theauthors' full names and affiliations, the name of thecorresponding author along with phone, fax and E-mailinformation. Present addresses of authors shouldappear as a footnote.The Abstract should be informative and completely selfexplanatory, briefly present the topic, state the scope ofthe experiments, indicate significant data, and point outmajor findings and conclusions. The Abstract should be100 to 200 words in length. Complete sentences, activeverbs, and the third person should be used, and theabstract should be written in the past tense. Standardnomenclature should be used and abbreviations should beavoided. No literature should be cited.Following the abstract, about 3 to 10 key words that willprovide indexing references should be listed.A list of non-standard Abbreviations should be added.In general, non-standard abbreviations should be usedonly when the full term is very long and used often.Each abbreviation should be spelled out and introducedin parentheses the first time it is used in the text. Onlyrecommended SI units should be used. Authors shoulduse the solidus presentation (mg/ml). Standardabbreviations (such as ATP and DNA) need not bedefined.The Introduction should provide a clear statement ofthe problem, the relevant literature on the subject, andthe proposed approach or solution. It should beunderstandable to colleagues from a broad range ofscientific disciplines.Materials and methods should be complete enough toallow experiments to be reproduced. However, onlytruly new procedures should be described in detail;previously published procedures should be cited, andimportant modifications of published procedures shouldbe mentioned briefly. Capitalize trade names andinclude the manufacturer's name and address.Subheadings should be used. Methods in general useneed not be described in detail.
Results should be presented with clarity and precision.The results should be written in the past tense whendescribing findings in the authors' experiments.Previously published findings should be written in thepresent tense. Results should be explained, but largelywithout referring to the literature. Discussion,speculation and detailed interpretation of data shouldnot be included in the Results but should be put into theDiscussion section.The Discussion should interpret the findings in view ofthe results obtained in this and in past studies on thistopic. State the conclusions in a few sentences at the end ofthe paper. The Results and Discussion sections caninclude subheadings, and when appropriate, bothsections can be combined.The Acknowledgments of people, grants, funds, etcshould be brief.Tables should be kept to a minimum and be designed tobe as simple as possible. Tables are to be typed doublespaced throughout, including headings and footnotes.Each table should be on a separate page, numberedconsecutively in Arabic numerals and supplied with aheading and a legend. Tables should be self-explanatorywithout reference to the text. The details of the methodsused in the experiments should preferably be describedin the legend instead ofin the text. The same data should not be presented inboth table and graph form or repeated in the text.Figure legends should be typed in numerical order on aseparate sheet. Graphics should be prepared usingapplications capable of generating high resolution GIF,TIFF, JPEG or Powerpoint before pasting in the MicrosoftWord manuscript file. Tables should be prepared inMicrosoft Word. Use Arabic numerals to designatefigures and upper case letters for their parts (Figure 1).Begin each legend with a title and include sufficientdescription so that the figure is understandable withoutreading the text of the manuscript. Information given inlegends should not be repeated in the text.References: In the text, a reference identified by meansof an author‘s name should be followed by the date ofthe reference in parentheses. When there are more thantwo authors, only the first author‘s name should bementioned, followed by ’et al‘. In the event that anauthor cited has had two or more works published duringthe same year, the reference, both in the text and in thereference list, should be identified by a lower case letterlike ’a‘ and ’b‘ after the date to distinguish the works.Examples:Nishimura (2000), Agindotan et al. (2003), (Kelebeni,1983), (Usman and Smith, 2001), (Chege, 1998; Stein,1987a,b; Tijani, 1993,1995), (Kumasi et al., 2001)References should be listed at the end of the paper inalphabetical order. Articles in preparation or articlessubmitted for publication, unpublished observations,personal communications, etc. should not be includedin the reference list but should only be mentioned inthe article text (e.g., A. Kingori, University of Nairobi,Kenya, personal communication). Journal names areabbreviated according to Chemical Abstracts. Authorsare fully responsible for the accuracy of the references.Examples:Giesielski SD, Seed TR, Ortiz JC, Melts J (2001).Intestinal parasites among North Carolina migrant farmworkers. Am. J. Public Health. 82: 1258-1262Stoy N, Mackay GM, Forrest CM, Christofides J,Egerton M, Stone TW, Darlington LG (2005).Tryptophan metabolism and oxidative stress in patientswith Huntington’s disease. N. J. Neurochem. 93: 611623.Mussel RL, De Sa Silva E, Costa AM, Mandarim-DeLacerda CA (2003). Mast cells in tissue response todentistry materials: an adhesive resin, a calciumhydroxide and a glass ionomer cement. J. Cell. Mol.Med. 7:171-178.Booth M, Bundy DA, Albonico P, Chwaya M, Alawi K(1998). Associations among multiple geohelminthinfections in school children from Pemba Island.Parasitol. 116: 85-93.0.Fransiscus RG, Long JC (1991). Variation in human nasalheight and breath, Am. J. Phys. Anthropol. 85(4):419427.Stanislawski L, Lefeuvre M, Bourd K, Soheili-Majd E,Goldberg M, Perianin A (2003). TEGDMA-inducedtoxicity in human fibroblasts is associated with earlyand drastic glutathione depletion with subsequentproduction of oxygen reactive species. J. Biomed. Res.66:476-82.
Case StudiesCase Studies include original case reports that willdeepen the understanding of general medicalknowledgeThe Title should be a brief phrase describing thecontents of the paper. The Title Page should include theauthors' full names and affiliations, the name of thecorresponding author along with phone, fax and E-mailinformation. Present addresses of authors shouldappear as a footnote.The Abstract should be informative and completely selfexplanatory, briefly present the topic, state the scope ofthe experiments, indicate significant data, and point outmajor findings and conclusions. The Abstract should be100 to 200 words in length. Complete sentences, activeverbs, and the third person should be used, and theabstract should be written in the past tense. Standardnomenclature should be used and abbreviations should beavoided. No literature should be cited.Following the abstract, about 3 to 10 key words that willprovide indexing references should be listed.A list of non-standard Abbreviations should be added. Ingeneral, non-standard abbreviations should be used onlywhen the full term is very long and used often. Eachabbreviation should be spelled out and introduced inparentheses the first time it is used in the text. Onlyrecommended SI units should be used. Authors shoulduse the solidus presentation (mg/ml).The Introduction should provide a clear statement ofthe problem, the relevant literature on the subject, andthe proposed approach or solution. It should beunderstandable to colleagues from a broad range ofscientific disciplines.The presentation of the case study should include theimportant information regarding the case. This mustinclude the medical history, demographics, symptoms,tests etc. Kindly note that all information that will leadto the identification of the particular patient(s) must beexcludedThe conclusion should highlight the contribution of thestudy and its relevance in general medical knowledgeThe Acknowledgments of people, grants, funds, etcshould be brief.References: Same as in regular articlesShort CommunicationsShort Communications are limited to a maximum of twofigures and one table. They should present a completestudy that is more limited in scope than is found in fulllength papers. The items of manuscript preparation listedabove apply to Short Communications with the followingdifferences: (1) Abstracts are limited to 100 words; (2)instead of a separate Materials and Methods section,experimental procedures may be incorporated into FigureLegends and Table footnotes; (3) Results and Discussionshould be combined into a single section.Proofs and Reprints: Electronic proofs will be sent (e-mailattachment) to the corresponding author as a PDF file.Page proofs are considered to be the final version of themanuscript. With the exception of typographical or minorclerical errors, no changes will be made in the manuscriptat the proof stage. Because IJMMS will be publishedfreely online to attract a wide audience), authors will havefree electronic access to the full text (in both HTML andPDF) of the article. Authors can freely download the PDFfile from which they can print unlimited copies of theirarticles.Copyright: Submission of a manuscript implies: that thework described has not been published before (except inthe form of an abstract or as part of a published lecture, orthesis) that it is not under consideration for publicationelsewhere; that if and when theManuscript is accepted for publication, the authors agree toautomatic transfer of the copyright to the publisher.
International Journal of Medicine and Medical SciencesTable of Contents:Volume 5Number 6June 2013ARTICLESCase ReportMultiple oesophageal coin-like foreign bodies appearing like one:A caution for otorhinolaryngologistSegun-Busari Segun, Afolabi Olushola Abdulrahman, Alabi Biodun Sulyman,Adebola Stephen Oluwatosin247Research ArticlesThe effect of clofibrate in near term newborns with non hemolytic jaundiceSedigheh Hossein pour Sakha, Manizheh Mostafa Gharehbaghi andMohammad Ebrahim RahbaniThe comparison of intradermal versus intramuscular vaccination ofhepatitis B in healthcare workers who fail to respond to previous repeatedintramuscular vaccinesMasoud Mardani and Amir RoudgariAntibacterial activity of Schiff base ligands containing pyridine anddisulphide moieties against some chosen human bacterial pathogensSabina Jhaumeer Laulloo, M. G. Bhowon, S. Ravikumar, A.Kalaiarasi, M. Raja and V. VijayakumarPatterns of antibiotic use among childrenHala Abdullah Hussien Abu Romman251255260264
International Journal of Medicine and Medical SciencesTable of Contents:Volume 5Number 6 June 2013ARTICLESResearch ArticlesHealth care seeking among pulmonary tuberculosis suspects in Wuhan:A community-based studyQiong-hong Duan, Peng Wang , Jing Lv , Rong Zhong, Wei-hua Wangand Qing-zhi ZengPerception of the public on the common zoonotic diseases in Jimma,Southwestern EthiopiaDawit Tesfaye, Daryos Fekede, Worku Tigre Alemayahu Regassaand Amene Fekadu273279Profile and outcome of diabetic admissions at the University of UyoTeaching Hospital, UyoB. C. Unadike, I. Essien, N. A. Akpan, E. J. Peters and O. E. Essien286Awareness and attitudes to voluntary counseling and testing (VCT) forhuman immunodeficiency virus/acquired immune deficiency syndromeS. U. Mbamara, N. J. A. Obiechina and J. C. Akabuike290Seroprevalence of Toxoplasma gondii between couples in Ramadi cityusing enzyme linked immunosorbent assay (ELISA)Mohanad Mohammad, Shehab Ahmed and Abudalla Hussain295Impact of lymphatic filariasis elimination programme by study ofadvances and challenges using mathematical modelVaibhav Changediya and Subhash Devdhe300
International Journal of Medicine and Medical SciencesTable of Contents:Volume 5Number 6 June 2013ARTICLESResearch ArticlesComparison of efficacy and safety of mifepristone-misoprostolcombination with ethacridine lactate in mid-trimester terminationof pregnancySmiti Nanda and Anshu PaulInhibition of ubiquitin-proteasome pathway: A possible treatmentof hepatocellular carcinomaAbdulkareem Albekairy, Abdulmalik Alkatheri and Mahmoud Mansour307312
Vol. 5(6), pp. 247-250, June 2013DOI: 10.5897/IJMMS09.395ISSN 2006-9723 2013 Academic national Journal of Medicineand Medical SciencesCase ReportMultiple oesophageal coin-like foreign bodiesappearing like one: A caution for otorhinolaryngologistSegun-Busari Segun, Afolabi Olushola Abdulrahman*, Alabi Biodun Sulyman, AdebolaStephen OluwatosinDepartment of Otorhinolaryngology,University of Ilorin Teaching Hospital,P. O. Box 2400, Ilorin,Kwara State, Nigeria.Accepted 2 May, 2013Ingestion of foreign bodies is a common pediatric problem. Majority of ingested foreign bodies passfreely without causing any injury. Ingestion of multiple foreign objects and recurrent episodes areuncommon. Thus we present a case of multiple foreign body ingestion to cautionotorhinolaryngologist. We present a six year old boy admitted eight hours following ingestion of amultiple roundish metallic object. There is associated dysphagia to solids and liquid feeds withdrooling of saliva. He has had two episodes of induced non-projectile vomiting which contains recentlyingested feeds prior to admission. There is no cough or difficulty in breathing. Examination of the neckrevealed a positive pointing sign. Plain radiograph of the soft tissues neck revealed a spherical radioopaque object of metallic density within the oesophagus at the level of C5 to C7. Patient had rigidoesophagoscopy under general anaesthesia with extraction of the multiple metallic foreign bodies. Itwas uneventful both post operatively and on follow up. The study thus revealed though multipleoesophageal foreign body is rare, there is need for caution among the otorhinolaryngologist whenextracting the oesophageal foreign bodies and also stressed the need to double check again followingextraction, that is, to repeat endoscopy.Key words: Multiple, oesophageal, foreign bodies, endoscopy, otorhinolaryngologist.INTRODUCTIONIngestion of foreign body is relatively common in theaero-digestive tract among the paediatric populationworld wide. However some of them get impactedbecause of either their large size or shapes (Amadasun1995; Hawkins 1990; Crysdal et al., 1991; Davey andBurkitt 1989; Jackler and Kaplan 1989), while some maypass through the gastrointestinal tract freely uneventful(MacManus 1941). Aerodigestive foreign body ingestionamong the paediatric population is a preventable problem(Afolabi et al., 2009). Management of foreign body ingestions varies and it depends upon the object ingested,its location, the patient's age and past history. Once a foreign body is impacted in the throat, it become associatedwith dramatic presentation of dysphagia and or droolingof saliva which may be a source of apprehension to thepatient, to the care giver and the healthcare providers.Ingestion of multiple foreign objects and repeatedepisodes are uncommon. Thus we present our case tocaution otorhinolaryngologist who is providing the rescueservices to have a second and third look.CASE REPORTPatient I.A. is six year old school boy who was admitted through theemergency Paediatric Unit eight hours post foreign body ingestion.The patient was said to have swallowed a roundish metallic object,*Corresponding author. E-mail: droaafolabi@yahoo.com. Tel: 2348035727069.
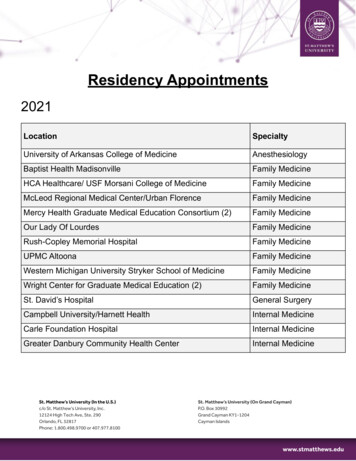
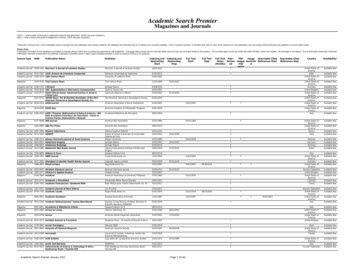
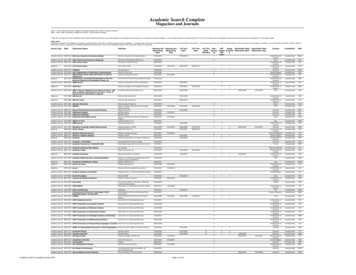
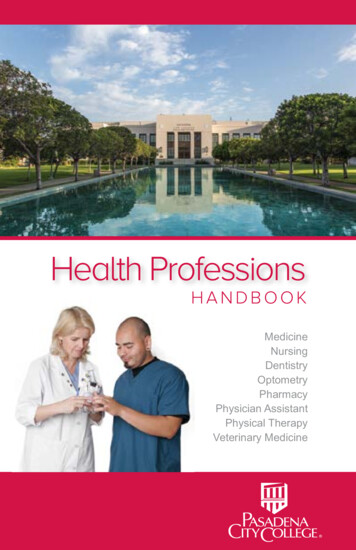
248Int. J. Med. Med. Sci.Figure 1. Plain radiographs of the soft tissues of theneck (anterior-posterior view).joint.The patient has good oro-dental hygiene but with pooling ofsaliva in the oral cavity; dentition was intact with no use of dentures,no foreign body visualised in the oropharynx. He has a granularposterior pharyngeal wall.Otologic and anterior rhinoscopy was essentially normal. Therewas tenderness at the front of the neck on palpation andscarification marks were noticed at these points.A diagnosis of impacted pharyngo-oesophageal foreign bodyingestion was made. Plain radiographs of the soft tissues of theneck (AP and lateral view) revealed a spherical radio-opaque objectof metallic density within the oesophagus at the level of C5 to C7,with air-oesophagogram in which the lower limit cannot bedelineated (Figures 1 and 2).The patient’s heamogram and blood biochemistry were all withinnormal limits. Patient had rigid oesophagoscopy using paediatricKarl Storz oesophagoscope with gentle extraction of foreign bodyunder general anaesthesia with small size 3.0 endotracheal tubeintubation. The surgical findings were multiple, silver colouredspherical metallic objects of the same size were extracted at about12 to 14 cm from the upper incisor, at the level of the cricopharyngeus. These objects were superimposed on one another.Repeat endoscopy was done to ensure no other foreign bodieswere left out.Post operatively, patient was uneventful. Patient commenced oralintake, 48 h post-operatively with no evidence of oesophageal perforation. The patient was discharged home 72 h post operatively.Follow up revealed he has remained well for six months now.DISCUSSIONFigure 2. Plain radiographs of the soft tissues of theneck (lateral view).while he was playing. There is associated odynophagia, dysphagiato solids and liquid diet and there is drooling of saliva. He has hadtwo episodes of induced non-projectile vomiting of which containsrecently ingested food prior to admission. There was no cough anddifficulty in breathing. There was no abnormal neck swelling. Therewere no otologic or nasal symptoms. The patient was not a knownpsychiatric or asthmatic patient. He is from a monogamous familyand the first child of the family. There was noticed failed attempt atremoval using bolus of meal.Clinical examination revealed a boy not in any obvious cardiorespiratory distress, not pale, afebrile, but with drooling of salivaand a positive pointing sign at the level of cricothyroid cartilageThe majority of foreign body ingestions occur in thepaediatric population with a peak incidence betweenages six months and six years (Afolabi et al., 2009; Webb1995; Cheng and Tam 1999; Hachimi-Idrissi et al.,1998).The age group which our index case presentedfalls into, may be associated with peer group influence. Inchildren, the true duration of the foreign body in theoesophagus may be unknown until it is discomforting;however in the index case the duration was said to beabout eight hours when the attention of the care giverwas drawn to it. Nevertheless, the exact timing ofinsertion may be difficult. Male are at risk of foreign bodyinsertion or ingestion as in the index case reported, thismay be associated with the increased risk of explorationof all cavities and high level of inquisitiveness among themale children than the female children similar to previousreports (Afolabi et al., 2009).In adults, true foreign object ingestion occurs morecommonly among those with psychiatric disorders,mental retardation or impairment caused by alcohol, andthose seeking some secondary gain with access to amedical facility (Webb 1995; Blaho et al., 1998; Kamal etal., 1999). Edentulous adults are also at greater risk forforeign body ingestion, including their dental prosthesis(Blaho et al., 1998; Abdullah et al., 1998).The most common site of foreign body impaction in theoesophagus is the cervical oesophagus at the level of thecricopharyngeus which is similar to our finding; in thereport presented, the foreign body lodged was lodged at
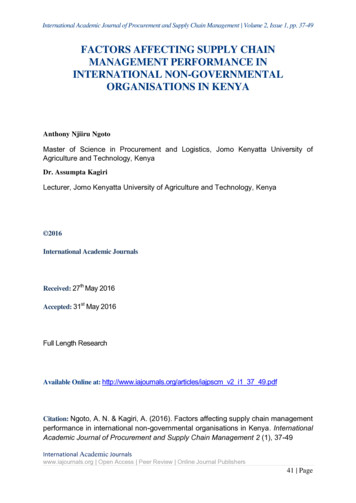
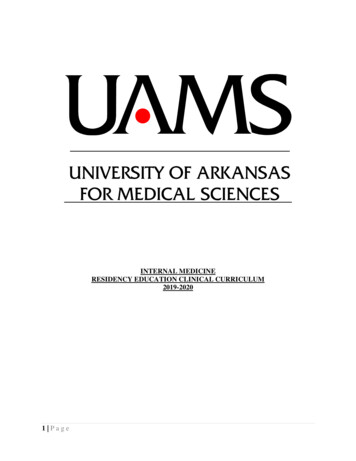
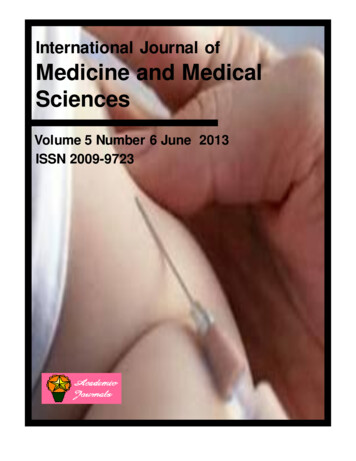
Segun et al.Figure 3. Multiple metallic foreign body.Figure 4. Diameter of multiple metallic foreign body.about 12 to 14 cm from the upper incisors. The nextcommonest site is the thoracic oesophagus at the level ofthe aortic arch (Nandi and Ong 1978). This radiographicinvestigation done in our index case if combined with theclinical findings of his pointing sign as it corresponded tothe location of the foreign body increases the specificity.(Lue et al., 2000) reported a sensitivity and specificity of39 and 72%, respectively while a recent study quoted24954.8 and 100% (Akazawa et al., 2004), for their plainradiographs. The present report does not report a certainpercentage as it was a single case report.Two radiological views as is customarily done in ourcentre was buttressed by Whelan-Johnson S, Hall CE,who equally stated that two radiological views arerecommended in the assessment of oesophageal foreignbodies (Whelan-Johnson and Hall 2009).Oesophageal foreign bodies are commonly encountered in otolaryngology practice. Such circumstances areoften compounded by pre-existing psychiatric problemssuch as bulimia and/or anorexia nervosa (Sastry et al.,2008). Patients with bulimia may often present with avery similar pattern of multiple episodes of ingestion oflarge foreign bodies. Identification of this eating disorder(especially when there is a recurrent history of large,accidentally ingested foreign bodies) and promptpsychiatric referral is essential for efficient long-termmanagement of this condition (Sastry et al., 2008). Ourpatient has no psychiatric illness.Management of the patient is influenced by thepatient’s age and clinical condition; the size, position ofthe coin if vertical or horizontal, shape, and classificationof the ingested material; the anatomic location in whichthe object is lodged; and the technical abilities of theendoscopist (Ginsberg 1995;Faigel et al., 1997; Michaudet al., 2009). The index patient presented had the multiple foreign body that is metallic, silver coloured with adiameter of about 4 cm (Figures 3 and 4) which is equivalent to the oesophageal diameter in vertical positionrelative to the oesophageal lumen; thus there was nosign of airway compression and allows minimal swallowing, thus no total dysphagia. The timing of endoscopicintervention in foreign body ingestion is dictated by theperceived risks of aspiration and/or perforation base onthe position/placement. In this situation, the interventionwas after 12 h of injury due to investigative procedureand sourcing for finance. This extraction was done undergeneral anaesthesia with a Karlstorz rigid oesophagoscope and foreign body removed. Further delay in theremoval may predispose the patient to corrosion of themetallic object with increased risk of perforation andmucosal reaction.ConclusionMultiple oesophageal foreign body though rare, is anemergency with need for caution among theotorhinolaryngologists/endoscopist. As it is commonamong the paediatric population, all patients with foreignbodies in the aero-digestive tract should have adequatehistory, ear, nose and throat examination along with thepointing sign (if the child is old enough) which should becombined with the radiological investigation. Patientsshould be assumed to have multiple foreign bodies thusthe need to scope the aero-digestive tract and re-scope
250Int. J. Med. Med. Sci.after extraction to look for a remnant if there are and toascertain the integrity of the site of impaction of the FB, inthis case the mucosa.REFERENCESAbdullah BJJ, Teong LK, Mahadevan J, Jalaludin A (1998). Dentalprosthesis ingested and impacted in the esophagus andorolaryngopharynx. J. Otolaryngol. 27:190-4.Afolabi OA, Okhakhu AL, Adeosun AA (2009). Re-Emergence Of CoinIn Nigerian Currency: Implication In Medical Practice. Intern. J.Otorhinolaryngol. 9(1):4.Akazawa Y, Watanabe S, Nobukiyo S, Iwatake H, Seki Y, UmeharaT, Tsutsumi K, Koizuka I (2004).The management of possiblefishbone ingestion. Auris Nasus Larynx 31(4):413-416.Amadasun EO (1995). Coin as oesophageal foreign
ABOUT IJMMS The International Journal of Medicine and Medical Sciences is published monthly (one volume per year) by Academic Journals. The International Journal of Medicine and Medical Sciences (IJMMS) provides rapid publication (monthly) of articles in all areas of Medicine and Medical Sciences such as: Clinical Medicine: Internal Medicine, Surgery, Clinical Cancer Research, Clinical .