Transcription
RISK OF BIAS ASSESSMENTINSTRUMENT FOR SYSTEMATICREVIEWS INFORMINGWHO GLOBAL AIR QUALITYGUIDELINESBy: the WHO Global Air Quality GuidelinesWorking Group on Risk of Bias AssessmentC
AbstractAir pollution represents the single largest environmental threat to health globally. WHO is developing new global airquality guidelines, based on the most recent scientific evidence, synthetized in accordance to predefined systematic reviewmethods. This publication includes a description of the instrument devised to assess the risk of bias in the individual studiesincluded in the systematic reviews of adverse health effects informing the guidelines. Further, general instructions andspecific subject matter advice to guide the assessments are provided.KeywordsEVIDENCE-BASED MEDICINE – methodsRESEARCH DESIGNBIASMETA-ANALYSIS AS TOPICREVIEW LITERATURE AS TOPICAIR POLLUTION – adverse effects, prevention and controlENVIRONMENTAL EXPOSURE – adverse effects, prevention and controlGUIDELINES AS TOPICAddress requests about publications of the WHO Regional Office for Europe to:PublicationsWHO Regional Office for EuropeUN City, Marmorvej 51DK-2100 Copenhagen Ø, DenmarkAlternatively, complete an online request form for documentation, health information, or for permission to quote or translate, on the Regional Officewebsite (http://www.euro.who.int/pubrequest). World Health Organization 2020Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0IGO; igo).Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriatelycited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services.The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commonslicence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was notcreated by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English editionshall be the binding and authentic edition”.Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World IntellectualProperty Organization.Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris.Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/bookorders. To submit requests for commercial use andqueries on rights and licensing, see http://www.who.int/about/licensing.Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such as tables, figures or images, it is yourresponsibility to determine whether permission is needed for that reuse and to obtain permission from the copyright holder. The risk of claimsresulting from infringement of any third-party-owned component in the work rests solely with the user.General disclaimers. The designations employed and the presentation of the material in this publication do not imply the expression of anyopinion whatsoever on the part of WHO concerning the legal status of any country, territory, city or area or of its authorities, or concerning thedelimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet befull agreement.The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by WHO inpreference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguishedby initial capital letters.All reasonable precautions have been taken by WHO to verify the information contained in this publication. However, the published material isbeing distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lieswith the reader. In no event shall WHO be liable for damages arising from its use.The named authors alone are responsible for the views expressed in this publication.
und.1Risk of bias assessment instrument.2General instructions to begin the risk of bias assessment.6Conduct risk of bias assessment at the outcome level. 6Provide a rationale for all judgements. 6Identify all critical and other potential confounders prior to assessing risk of bias. 6Specific guidance to complete the risk of bias assessment.8Confounding. 8Selection bias. 8Exposure assessment. 8Outcome measurement. 9Missing data. 9Selective reporting. 9Overall judgement for a domain.10Judgements per risk of bias domain across studies.10References. 11Risk of bias assessment instrument for systematic reviews informing WHO global air quality guidelinesiii
AcknowledgementsThis publication consists of a risk of bias assessment instrument for epidemiologic studies of air quality and health,and written guidance for its application. The work was conducted by the WHO Global Air Quality GuidelinesWorking Group on Risk of Bias Assessment convened by the WHO European Centre for Environment and Health(WHO Regional Office for Europe) in the context of the forthcoming WHO global air quality guidelines. Externalmethodologists Jos Verbeek (Cochrane Work) and Rebecca Morgan (McMaster University) led the developmentof the instrument and the guidance, respectively.Both the tool and guidance were developed with input from members of the Guideline Development Group(for the update of WHO global air quality guidelines): Bert Brunekreef (Utrecht University), Francesco Forastiere(King’s College London) and Aaron Cohen (Health Effects Institute), as well as from staff of the WHO RegionalOffice for Europe: Román Pérez-Velasco, Hanna Yang and Dorota Jarosińska.Additional comments were provided by external methodologists Inga Mills (formerly Cochrane Response) andEva Rehfuess (Cochrane Public Health Europe), and members of the Global Development Group: Michael Brauer(University of British Columbia), Marie-Eve Héroux (Health Canada), Michal Krzyzanowski (King’s College London),Nino Künzli (Swiss Tropical and Public Health Institute) and Martin Williams (King’s College London).The instrument was pilot tested by the Systematic Review Team members: Richard Atkinson (St George’s,University of London), Jie Chen (Utrecht University), Wei-jie Guan (Guangzhou Institute of Respiratory Disease),Gerard Hoek (Utrecht University), Ken Lee (University of Edinburgh), Pablo Orellano (Universidad TecnológicaNacional San Nicolás), Nick Spath (University of Edinburgh) and Xueyan Zheng (Guangdong Provincial Center forDisease Control and Prevention), who also provided valuable input for its improvement.The tool was discussed at the 2nd Guideline Development Group meeting held on 14–16 March 2018 in Bonn,Germany, and the Working Group revised both the tool and guidance in accordance with suggestions receivedthroughout their development.The WHO Regional Office for Europe acknowledges funding and in-kind contributions from the EuropeanCommission (Directorate-General for Environment); the German Federal Ministry for the Environment, NatureConservation and Nuclear Safety; the German Federal Ministry of Health; the Government of the Republic ofKorea; the Swiss Federal Office for the Environment; and the United States Environmental Protection Agency.AbbreviationsAQGsair quality guidelinesGRADEGrading of Recommendations Assessment, Development and Evaluation (framework)PECOSPopulation, Exposure, Comparator, Outcome(s), and Study DesignPMparticulate matterPM2.5particulate matter with a diameter of 2.5 µm or lessROBINS-IRisk of Bias In Non-randomized Studies - of InterventionsSESsocioeconomic statusivRisk of bias assessment instrument for systematic reviews informing WHO global air quality guidelines
BackgroundWith the release of the Risk of Bias In Non-randomized Studies - of Interventions (ROBINS-I) (1) and the subsequentpublication of an equivalent instrument to evaluate ROBINS-I of exposures (2), research is progressing to assistsystematic review authors and guideline developers. For guideline panels and decision-makers, researchers aredefining methods for integration of these instruments into established evidence assessment frameworks, suchas the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach (3). However,interest exists to further develop the current instrument for assessment of risk of bias in observational air pollutionepidemiology studies. Likewise, recent guidance on systematic review of observational studies of aetiologyrecommends the development of tailored-made instruments for each review, based on general principles (4).Assessment of potential bias lies at the core of all epidemiology when trying to understand the relationshipbetween an exposure and an outcome. In addition, it is a basic component of any well-performed systematicreview of evidence, as outlined by the WHO handbook for guideline development, 2nd edition (5). When conductingsystematic reviews to inform the WHO global air quality guidelines (AQGs), risk of bias assessment was thereforenecessary for all eligible studies to understand the certainty in that relationship.The current instrument was iteratively developed by members of the Guideline Development Group forthe update of WHO global AQGs with expertise in air pollution epidemiology and experts in developing andapplying risk of bias instruments in observational studies, under the oversight of WHO staff. The instrument wasdesigned specifically to evaluate risk of bias within eligible air pollution studies included in systematic reviews,commissioned by WHO, of studies on short- and long-term exposure to air pollutants (i.e. particulate matter(PM) smaller than 2.5 and 10 µm in diameter, nitrogen dioxide, sulphur dioxide, carbon monoxide and ozone), toexamine their effect on critical patient-important outcomes, such as natural cause and cause-specific mortality(e.g. cardiovascular mortality).Studies of short- and long-term exposure to air pollution use different study designs and make use of differentcontrasts of exposure: day-to-day fluctuation for the short-term studies and spatial variation of averageconcentrations for the long-term exposure studies. Designs included in the WHO-commissioned systematicreviews were time series, case-crossover and panel studies (short-term) and cohort and case-control studies(long-term).In developing this instrument, each topic of interest (exposures and outcomes) was examined based on theresearch questions (framed as PECOS; Population, Exposure, Comparator, Outcome(s), and Study Design) to informthe confounders and analysis methods that should be taken into account when determining the potential forbias within a primary study. In a well-formed research question (such as a PECOS), a distinction is made betweenan exposure and comparator group. This is required for decision-making, as the exposure and the comparatordistinguish between the options available. For studies of exposure, the PECOS may take one of five variations (6).For WHO global AQGs, the interest lies in the comparison between different levels of exposure (e.g. a lower levelcompared to a higher level of exposure to PM2.5).To inform the development process, WHO staff conducted a review of existing tools at inception. In addition,members of the Working Group on Risk of Bias Assessment and the Systematic Review Team pilot tested theinstrument for accuracy. It is important to note, however, that the risk of bias instrument below is not a checklist,but a list of guided topics organized by domains and subdomains to consider when judging the potential for bias.The instrument should be used by assessors with detailed subject matter knowledge of air pollution epidemiologyand training in risk of bias instrument application.Risk of bias assessment instrument for systematic reviews informing WHO global air quality guidelines1
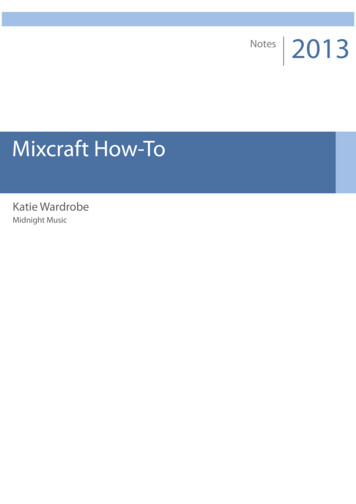
Risk of bias assessment instrumentTopic:Risk of biasinstrumentReviewer ID:Study ID:Date:Long-term studies Short-term studiesFor eachPECOSNotesCritical potentialconfoundersOther w-risk (idealstudy) criteriaModerate-riskcriteriaHigh-riskcriteriaWere allconfoundersconsideredadjusted for inthe analysis?All critical andother/additionalpotentialconfoundersadjusted for orwith support(e.g. exploratoryanalysis) ofminimal riskdue to residualconfounding(i.e. there isevidence that thisconfounder mightnot lead to severeconfounding).All critical potentialconfounders butnot all other/additional potentialconfoundersadjusted forwithout support(e.g. exploratoryanalysis) of minimalrisk due to residualconfounding (i.e.there is evidencethat this confoundermight not lead tosevere confounding).Not all criticalpotentialconfoundersadjusted forwithout support(e.g. exploratoryanalysis) ofminimal riskdue to residualconfounding.Validity ofmeasuring ofconfoundingfactorsConfoundersmeasured withdocumented validmethods.Not all criticalpotentialconfounders weremeasured withdocumented validmethods; however,there is evidencethat this does notlead to severeconfounding.Any critical orother/additionalpotentialconfounder notvalidly assessedand evidenceof residualconfounding.Control inanalysis (Didthe authors usean appropriateanalysis methodor study designthat controlledfor confoundingdomains?)Authors usedappropriateanalysis methodsor study designsthat controlledfor confoundingdomains.Authors usedinappropriatemethods or designswhen adjusting forcritical potentialconfounders;however, there isevidence that thisdoes not lead tosevere confounding.Authors usedinappropriatemethods orstudy designswhen adjustingfor critical gementfor adomain:Low/Moderate/HighRationale/Notes(quotes fromthe study tojustify thejudgement)Overall2Risk of bias assessment instrument for systematic reviews informing WHO global air quality guidelines
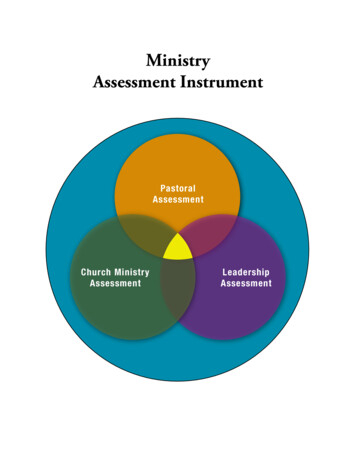
contd.Domain2.Selection biasSubdomainLow-risk (idealstudy) ction ofparticipantsinto the study(includes nonresponse)Participants inall exposurelevels and withall outcomes hadequal opportunityto be in the study.Participants in allexposure levelsdid not have equalopportunity to be inthe study, but notto the extent thateffect estimates wereseriously biased(rationale required).Participants inall exposurelevels did nothave equalopportunity tobe in the study,to the extent thateffect estimateswere seriouslybiased.Overalljudgementfor adomain:Low/Moderate/HighRationale/Notes(quotes fromthe study tojustify thejudgement)Overall3.ExposureassessmentMethods usedfor exposureassessmentExposure levelsassessed withappropriatemethods.Exposure levelsassessed with lessthan appropriatemethods but notto the extent thateffect estimates wereseriously biased.Exposure levelsnot assessedwith appropriatemethods to theextent that effectestimates wereseriously biased.Exposuremeasurementmethodscomparableacross the rangeof exposureMeasurementmethods usedare comparableacross the range ofexposure.Measurementmethods varyacross the range ofexposure; however,there is evidencesupporting thatthe exposuremeasurement issufficiently similarthat effect estimatesare not seriouslybiased.Measurementmethods varyacross the rangeof exposure anddifferences arenot accounted for.Change inexposure status(for long-termstudies only)Spatial exposurecontrasts didnot changethroughout thestudy or timevarying exposurewas used toaccount forchanges.Spatial exposurecontrasts did changethroughout thestudy and were notaccounted for buteffect estimates werenot seriously biased.Spatial exposurecontrastsdid changethroughout thestudy and werenot accountedfor, and effectestimateswere seriouslybiased and weredifferent in casesand non-cases.ExposurecontrastExposurecontrast waslarge comparedto the precisionof exposureassessment(between-subjectvariance largerthan withinsubject variance).Exposure contrastwas small relativeto the withinsubject variance butnot to the extentthat the study isuninformative.Exposure contrastwas so smallrelative to thewithin-subjectvariance thatthe study isuninformative.OverallRisk of bias assessment instrument for systematic reviews informing WHO global air quality guidelines3
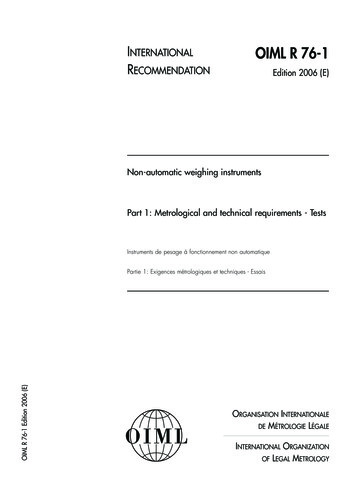
contd.Domain4.OutcomemeasurementSubdomainLow-risk (idealstudy) ding ofoutcomemeasurementOutcomemeasurementswere notinfluenced byknowledge of theexposure.Outcome measureswere influenced byknowledge of theexposure; however,evidence supportsthat effect estimateswere unlikely biased.Outcomedetectionwas relatedto exposurestatus and effectestimates arelikely biased.Validity ofoutcomemeasurementsNo systematicerrors in themeasurement ofthe outcome orsystematic errorswere unrelated tothe exposure.Minimum systematicerrors suspected inthe measurementwere related to theexposure received.Critical systematicerrors in themeasurementwere related tothe exposurereceived.OutcomemeasurementMethods ofoutcomeassessment werecomparable acrossexposure groups.Methods of outcomeassessment were notcomparable acrossexposure groups;however, evidencesupports thatoutcome detectionwould not havevaried.Methods ofoutcomeassessment werenot comparableacross exposuregroups.Overalljudgementfor adomain:Low/Moderate/HighRationale/Notes(quotes fromthe study tojustify thejudgement)Overall5.Missing dataMissing dataof outcomemeasuresNo missingoutcome dataor missing datainfrequent ( 10%)or missing datarelated to outcomeor exposure dataimputed usingappropriatemethods.Missing data onoutcomes notinfrequent ( 10%)and rationale forattrition explained inthe study; methodshave possibly beenused to properlyaccount for it.Evidence ofsubstantialmissing outcomedata ( 10%),rationale forattrition notexplained inthe study andmethods unlikelyto properlyaccount for it.Missing data ofexposuresNo missingexposure dataor missing datainfrequent ( 10%)or missing datarelated to exposureor outcome dataimputed usingappropriatemethods.Missing data onexposure notinfrequent ( 10%)and rationale forattrition explained inthe study; methodshave possibly beenused to properlyaccount for it.Evidence ofsubstantialmissing exposuredata ( 10%),rationale formissing datanot explained inthe study, and/or the portionof participantsand reasons formissing data aredissimilar acrossexposures/exposure groups.Overall4Risk of bias assessment instrument for systematic reviews informing WHO global air quality guidelines
contd.Domain6.SelectivereportingSubdomainLow-risk (idealstudy) ors reporteda priori primaryand secondarystudy aimsEffect estimatespresented forall hypothesestested as peraims; referenceto published orunpublished studyprotocol.Effect estimatespresented for some(not all) hypothesestested as per aims,but evidencesuggests that effectestimates unlikely tobe seriously biased.Effect estimatesselectivelypresented forsome (not all)hypothesestested as peraims and effectestimates likelyto be seriouslybiased.Overalljudgementfor adomain:Low/Moderate/HighRationale/Notes(quotes fromthe study tojustify thejudgement)OverallRisk of bias assessment instrument for systematic reviews informing WHO global air quality guidelines5
General instructions to begin the risk of biasassessmentThe following fields should be populated in the risk of bias instrument: topic of the review (refer to the specific PECOS from the systematic review) date when the risk of bias assessment is conducted reviewer ID (coordinate across the systematic review team) study ID (coordinate across the systematic review team and studies) relevant critical and other/additional potential confounders.Conduct risk of bias assessment at the outcome levelThe risk of bias assessment is conducted at the outcome level; therefore, should a primary study report on tworelevant outcomes, risk of bias must be evaluated twice. This is because the risk of bias may be different dependingon the outcome. For example, if the same study reports on both all-cause mortality and cardiovascular mortality,separate risk of bias evaluations must be conducted. The risk of bias assessment of all-cause mortality may differfrom that of cardiovascular mortality depending on the certainty of the ability to differentiate specific causes ofmortality. It is important to clearly state when there is uncertainty around the identification or diagnosis of theoutcome of interest.Provide a rationale for all judgementsAs mentioned previously, this instrument is not a checklist because different judgements can be made as to thepotential for bias introduced by each subdomain. As such, for the transparency of the overall risk of bias for thesystematic review and subsequent guideline, rationales must be provided for each risk of bias judgement made.The rationale should address why the specific judgement (“low”, “moderate” or “high” risk of bias) was selected.The rationale may be in a narrative form from the rater or use a quote from the primary study under review.Identify all critical and other potential confounders prior toassessing risk of biasA confounder is a factor associated with the exposure that influences the disease outcome (7). Before ratersattribute any difference in the outcome between the exposure and comparison to the exposure of interest,exploration of potential factors along this causal pathway (i.e. confounders) is required. Confounders have arelationship with the outcome and exposure, and their presence (unless adequately adjusted for) can lead to amis-specified (either over- or underestimate) association between the outcome and exposure.Typically, subject matter expertise is needed when identifying critical and other potential confounders. Criticalpotential confounders may be thought of as strong determinants of the health outcome at hand (e.g., smokingand lung cancer), while other potential confounders would be less strong/consistent determinants (e.g., diet andchronic obstructive pulmonary disease). However, some other potential confounders may be considered criticalin that they are powerful known risk factors for the outcome, and lack of adjustment for them (by analysis orrestriction) is a major source of uncertainty. Critical and other potential confounders that should be adjusted forin each primary study should be identified in the initial stages of the systematic review. However, there may besituations during the conduct of the systematic review where the reviewers realize that either: (i) the confounders6Risk of bias assessment instrument for systematic reviews informing WHO global air quality guidelines
are not relevant or (ii) a confounder that was not identified should indeed be captured in the study. The WorkingGroup identified confounders for the specific reviews informing AQGs in Table 1. This is a task specific to eachbody of evidence at hand.Table 1. Critical and other potential confounders to assess confounding in systematic reviews informing WHOglobal AQGsCritical potential confoundersOther potential confoundersLong-term studies: cohort, case-control Age Year of enrolment Sex Ethnicity Individual- or area-level socioeconomic status (SES) (at least one of thefollowing):– educational level (individual)– employment status (occupational class) (individual)– individual income– mean income (area-level)– deprivation index (area-level) or other SES indices Diet Physical activity Marital status Smoking Body mass indexShort-term studies: time series, case crossover,a panel Temperature Holidays (not vacations) Seasonality Influenza epidemics Day of the week Long-term trendsaThe case-crossover approach may control for seasonality and long-term trends by design.Risk of bias assessment instrument for systematic reviews informing WHO global air quality guidelines7
Specific guidance to complete the risk of biasassessmentFor each domain of risk of bias, related subdomains and guidance are provided to assist raters in making ajudgement about whether the study presents “low”, “moderate” or “high” risk of bias. Since raters will make ajudgement as to the risk of bias for each subdomain, it is important that a rationale is provided in the risk of biasinstrument.ConfoundingIn addition to the guidance on confounding provided above, it is important to consider some issues on controllingfor long-term trends.While the PECOS may be asking for the relationship between the exposure of interest and short-term variation inthe outcome, long-term trends may dominate the potential confounders. It is therefore essential to demonstrate aseparation between short- and long-term trends to have certainty in the assessment of the relationship betweenthe exposure and outcome. Regression models may be appropriate to demonstrate that long-term trends arecontrolled for in the analysis. Some options available include: (i) a time stratified model (simple indicator variables);(ii) periodic functions; or (iii) flexible spline functions. The use of one of these models to adjust for potential longterm confounders allows for the isolation of the exposure of interest (8).It is also necessary to think in which direction the long-term trend would potentially bias the effect (i.e. toward oraway from the null).Selection biasSelection bias occurs when some eligible participants are excluded in a way that leads to the association betweenexposure and outcome differing from the association that would have been observed in the PECOS.Exposure assessmentThe variable of interest in the exposure measurement domain is the personal exposure to outdoor pollutants asthe outdoor concentration near the homes of studied populations. Most people spend over 70% of their time athome. A high percentage of this time is spent indoors, so a legitimate question is how well spatial and temporalvariations in outdoor concentrations are correlated with spatial and temporal variations in indoor and personalexposure to outdoor pollutants. A sizeable literature shows these correlations to be moderately to very high. Aspersonal or indoor monitoring is impossible in the typically large study populations in air pollution epidemiology,the focus is therefore on assessment of the risk of bias associated with the various ways in which outdoorconcentrations have been assessed in the studies included in the systematic reviews. However, raters should alsobe aware – for the case of PM2.5 – of the systematic reviews of residential outdoor-personal and ambient-personalcorrelations by Avery et al., 2010 (9,10). Again here the basic idea is to make a distinction between studies at highrisk of bias because the assessment of exposure in the study at hand was inadequate, and studies at low risk ofbias because the exposure assessment was performed in an adequate way.Studies of the effects of short-term, day-to-day variations in air pollution on the day-to-day variations in mortalityand hospital admissions typically rely on routine measurements of air poll
Risk of bias assessment instrument for systematic reviews informing WHO global air quality guidelines 1 With the release of the Risk of Bias In Non-randomized Studies - of Interventions (ROBINS-I) (1) and the subsequent publication of an equivalent instrument to evaluate ROBINS-I of exposures (2), research is progressing to assist systematic review authors and guideline developers.