Transcription
Confidential PhysicianFeedback Reports:Designing for OptimalImpact on PerformanceAgency for Healthcare Research and QualityAdvancing Excellence in Health Care www.ahrq.gov
This guide is a practical resource designed to inform readers, particularlydevelopers of confidential physician feedback reports (e.g., medical groups,health plans, payers, professional societies, regional collaboratives, anddissemination and implementation campaigns), about evidence-based strategiesto consider when developing or refining a feedback reporting system.The findings and conclusions in this document are those of the authors and donot necessarily represent the views of the Agency for Healthcare Research andQuality (AHRQ) or the U.S. Department of Health and Human Services(HHS). Mention of any products, Web sites, or related materials does not implyendorsement by AHRQ, HHS, or the U.S. Government.
Confidential Physician Feedback Reports: Designing forOptimal Impact on PerformancePrepared by:Peggy McNamara, Agency for Healthcare Research and QualityDale Shaller, Shaller Consulting GroupJan De La Mare, Agency for Healthcare Research and QualityNoah Ivers, Women’s College Research Institute and University of TorontoKey words: audit and feedback, performance feedback, data/feedback and benchmarking,practice profiling, relative social ranking, practice improvementAHRQ Publication No. 16-0017-EFMarch 2016
This document is in the public domain and may be used and reprinted without permission exceptthose copyrighted materials noted, for which further reproduction is prohibited without specificpermission of copyright holders. Citation of the source is appreciated.Suggested CitationMcNamara P, Shaller D, De La Mare D, Ivers N. Confidential physician feedback reports:designing for optimal impact on performance. Rockville, MD: Agency for Healthcare Researchand Quality; 2016. AHRQ Pub. No. 16-0017-EF.About the AuthorsPeggy McNamara, M.S.P.H., Senior Fellow at the Agency for Healthcare Research and Quality(AHRQ), Rockville, MD. Ms. McNamara codirected the Agency’s 7-year ‘Chartered ValueExchange’ learning network to provide technical assistance to 950 health sector leaders across 24regional collaboratives working to improve health care system performance. Her researchincludes a special focus on hospital and physician performance transparency for consumers inmaking health care decisions, and for physicians in assessing and improving their practices.Dale Shaller, M.P.A., Principal, Shaller Consulting Group, Minneapolis, MN. Mr. Shaller hasdevoted more than three decades to the design, implementation, and evaluation of health carequality measurement and improvement programs that support the information needs of bothpatients and clinicians. His research has focused primarily on the collection and use of patientexperience measures for public reporting as well as private feedback reporting to physicians.Jan De La Mare, M.P.Aff., Senior Research Scientist, AHRQ, Rockville, MD. Ms. De La Marecodirected the Agency’s ‘Chartered Value Exchange’ learning network and currently works aspart of AHRQ’s EvidenceNOW initiative, aimed at helping small primary care practices improvethe heart health of their patients. She also leads work on the Quality Indicators Toolkit, designedto help hospitals assess and improve their quality of care and patient safety.Noah Ivers, M.D., Ph.D., family physician at Women’s College Hospital, Scientist at Women’sCollege Research Institute, and Assistant Professor with the Department of Family andCommunity Medicine and the Institute for Health Policy Management and Evaluation at theUniversity of Toronto. Dr. Ivers’ research focuses on designing and evaluating interventionsusing existing data sources to drive quality improvement in primary and community caresettings, and he was lead author of the 2012 Cochrane Review on audit and feedback.AcknowledgmentsAlthough the authors take sole responsibility for this publication, the clarity and organization ofits content benefited greatly from thoughtful comments made by the following individuals whogenerously contributed their time and expertise in reviewing a formative draft: Jim Chase,Minnesota Community Measurement; Robbie Foy, University of Leeds; Michael Fischer,National Resource Center for Academic Detailing; Irene Fraser, formerly with AHRQ; JaniceGenevro, AHRQ; Courtney Gidengil, RAND; Tasneem Khan, University of Leeds; BruceLandon, Harvard Medical School; Rodney McCurdy, AHRQ; Robert McNellis, AHRQ; andStephanie Teleki, California HealthCare Foundation. A special thank you is extended to LynetteLilly, K4 (AHRQ contractor), for her capable and prompt assistance with references.ii
ContentsForeword .vIntroduction .1Part One: Physician Feedback Report Fundamentals .21-1. What are confidential physician feedback reports and what is their purpose? . 21-2. Do physician feedback reports work? . 41-3. What types of organizations develop confidential physician feedback reports? . 4Part Two: Design of Physician Feedback Reporting Systems .142-1. Identifying a clinical focus . 142-2. Ensuring underlying data support aims of report . 162-3. Optimizing user functionality . 172-4. Delivering to promote impact . 20Part Three: Three Strategies for Continuous Improvement of Physician Feedback ReportingSystems .223-1. Systems that enable physicians to correct patient-level data . 223-2. Prerelease testing: Giving physicians the opportunity to make feedback reports work forthem . 233-3. Postrelease monitoring and evaluation . 24Part Four: A Research Agenda To Advance the Science of Physician Feedback ReportingSystems .254-1. Understanding key attributes of highly successful feedback reporting systems . 264-2. Understanding the implementation contexts that promote highly successful feedbackreporting systems . 264-3. Understanding factors that affect both the design and context of feedback reportingsystems . 27Concluding Remarks .28References .29Appendixes .33Appendix 1. Advantages of sharing “unblinded” performance data within a team, practice, ornetwork* . 33Appendix 2. Performance improvement messaging for physicians: lessons from marketresearch* . 34iii
ForewordConfidential feedback reporting is widely considered to be a precursor to and a foundation forperformance improvement. However, to enable change, the physician responsible for andcapable of change must receive, understand, and act on the information. Physicians need morethan mere data.In recent years, we’ve observed insufficient attention being given by organizers of variousperformance improvement activities to the particulars of how to effectively convey performancedata to physicians and other clinicians. In some cases, those in the field make no distinctionbetween confidential feedback reports for clinicians and public reports for consumers, yet thetwo audiences couldn’t be more different in their informational needs. Moreover, it appears thatinadequate attention is paid during the selection of measures and design of the reports to themechanisms by which the reports could lead to improvement through changes in clinicianbehavior.In addition, there is little acknowledgment that feedback reporting can be done either well orpoorly. Too often, it is wrongly viewed as a dichotomous variable; was performance data madeavailable to clinicians—yes or no? It is inappropriately dismissed as a small detail to be checkedoff instead of a bridge that can lead to either performance improvement success or failure,depending on its underlying architecture.It turns out that confidential feedback reporting for physicians is a well-studied topic; in fact it’sone of the most studied performance improvement interventions (Ivers, Grimshaw, et al., 2014).Yet some developers of feedback reports are surprisingly unaware that an evidence base of bestpractices exists to guide them. This is the case even for some well-resourced, large-scaleinterventions.Part of the problem is that different applications, most notably the fields of quality improvementand dissemination and implementation of clinical advances, use different terms for essentiallythe same activity of reporting, which undermines the spread of learning. Relatedly, academicjournals—the curators of the evidence—tend to use the term “audit and feedback,” which is notrecognizable to many working in the field, further limiting uptake.Last but certainly not least, we in the health services research community haven’t done a verygood job of translating and communicating what we do know to those who can benefit most fromthe evidence, i.e., developers of feedback reports.This applied resource seeks to address these shortcomings and inform developers of feedbackreports about evidence-based strategies to consider when developing or refining a feedbackreporting system. This guide is appropriate for many audiences, including medical groups, healthplans, payers, professional societies, regional quality improvement collaboratives, anddissemination and implementation campaigns. In pulling this resource together, we explicitlyseek to dismantle “language silos” and use terms readily understandable to all those working toimprove the performance of our health care system.v
A secondary aim is to foster discussion among report developers, the broader qualityimprovement and dissemination and implementation communities, researchers actively workingon the topic, and funders of research and improvement initiatives. We hope they can worktogether to set research priorities that will collectively advance these reports as effectiveinstruments to influence clinician behavior and improve care. Subsumed in this aim is interest inactively discouraging research that uses scarce research dollars to retest what are consideredsettled areas of inquiry.Peggy McNamara, Dale Shaller, Jan De La Mare, and Noah IversMarch 2016vi
IntroductionConfidential physician feedback reports seek to make physicians aware of their individualperformance on one or more metrics in order to influence their clinical practice and improveperformance. There is growing interest in feedback reports and their potential to improveperformance, fueled in part by: Recognition that health care quality is not where we as a Nation want it to be, and thepace of improvement is unacceptably, unnecessarily slow;Concern about health care waste associated with inappropriate use, underuse, and overuseof services;Dissatisfaction with the time it takes to effectively integrate clinical advances into routinemedical practice;The reality that collective improvement is merely the sum of improvements made byindividual physicians, individual practices, and hospitals, one at a time;Belief that physicians’ awareness of their own performance builds a critical andnecessary foundation for improvement; andProliferation of payment incentives tied to performance metrics, which overlays afinancial imperative (Hysong, 2009) on top of the professional imperative to deliver highquality care.This resource is intended to support the evidence-based design of physician feedback reportingsystems. The focus is on developing and using feedback reports for individual physiciansworking in medical practices and acute care hospitals. But many of the design elements andengagement strategies discussed can be usefully applied to other clinicians in other health caresettings, making it a highly flexible intervention to improve performance (Hysong, 2009;Flottorp, et al., 2010).The guide is organized into four parts: Part One presents the “fundamentals” of physician feedback reports in a question andanswer format.Part Two lists evidence-based practices on how to design a physician feedback reportingsystem for maximal impact. The purpose of this section is to identify the factorsempirically associated with success so that future reports can be most effective. See TextBox 1 for a summary of methods used to identify best practices.Text Box 1. Summary of methodsThe primary source of evidence is the 2012 Cochrane Review on Audit and Feedback: Effects onProfessional Practice and Healthcare Outcomes, which identifies a limited number of evidence-basedpractices from a review of randomized trials (Ivers, et al., 2012). Because the evidence base on howbest to design physician feedback reports is still developing, authors supplemented the CochraneReview findings with additional evidence, including tips from report developers and users. Theresulting two categories of guidance—one based on rigorous outcome evaluations and the otherbased on experiential data—are clearly labeled and distinguished. A formative draft of this guide wasreviewed by a multidisciplinary panel that included research experts and physicians and otherpractitioners engaged in performance improvement.Confidential Physician Feedback Reports1
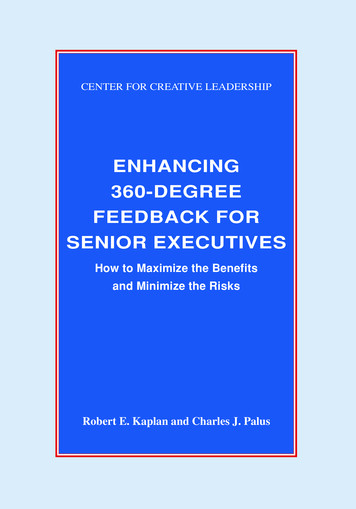
Part Three discusses three strategies available to developers of physician feedback reportsto support continuous improvement of their reporting systems.Part Four reviews research priorities needed to collectively advance the science ofconfidential feedback reporting. They derive in part from a panel discussion at the 2015AHRQ Research Conference (De La Mare, et al., 2015).Part One: Physician Feedback Report FundamentalsPart One presents basic information about physician feedback reports in a question and answerformat: Section 1-1: What are confidential physician feedback reports and what is their purpose?Section 1-2: Do confidential physician feedback reports work?Section 1-3: What types of organizations develop physician feedback reports?1-1. What are confidential physician feedback reports and what is their purpose?Confidential physician feedback reports refer to data that are shared with physicians on theirclinical performance over a specified period, as captured by various quality and resource useindicators. In contrast to public performance reports aimed at supporting the information needsof consumers and purchasers, confidential feedback reports are designed to support theimprovement goals of physicians, other clinicians, and health care organizations. Feedbackreports also are distinct from electronic “reminders” designed to provide clinical decision supportto physicians at the time of a medical encounter with a patient.While this guide uses the term “confidential feedback reporting,” other terms (e.g., audit andfeedback, performance feedback, data/feedback and benchmarking, relative social ranking,practice profiling) represent the same or similar types of reports. Feedback reports are nottypically made available to the public, although the extent to which the performance reportsremain “confidential” within an organization varies. See discussion of “unblinded” reports inappendix 1.Physician feedback reports can be print, Web-based, or embedded in electronic medical records.Although the content, design, and delivery of feedback reports vary widely, most include someway to compare the performance of an individual or group of physicians to that of a comparatorgroup. See discussion of comparators in section 2-3.Figure 1 is an excerpt of a feedback report comparing six physicians in the same primary carepractice site with each other and with a target goal for each of five specific clinical indicatorsrelevant to diabetes care. Scores that are shaded indicate performance below the target goal. Forexample, the percentage of Physician C’s patients achieving low-density lipoprotein (LDL)cholesterol 100 (28.6%) is below the target goal of 35 percent.2Confidential Physician Feedback Reports
Figure 1. Excerpt of feedback report to convey primary care physicians’ performance in treatingpatients with diabetesPhysicianTarget GoalPhysician APhysician BPhysician CPhysician DPhysician EPhysician FPractice SiteNetworkN of Patients-1131711073082542071,1605,596A1C 8%40%48.7%66.1%57.1%75.0%61.4%56.5%63.4%63.6%BP DL %82.0%Source: University of Cincinnati Physicians, 2016. Report layout modified with permission.Physician feedback reports are designed to facilitate assessments of care that will lead toimprovements in clinical care quality, patient experience, appropriate resource use or costreduction, and timely uptake of new clinical advances.Objectives typically include: Enabling physicians, other clinicians, and health care organization leaders to assess theirperformance, which is a prerequisite to improvement.Facilitating dialogue among team members to identify and prioritize areas of health caredelivery needing improvement, and in some cases to shift clinical or organizationalattention to areas of relative deficit.Motivating efforts to improve, specifically by shifting attention to areas of relative need.Evaluating efforts to improve, perhaps in response to an earlier feedback report.Other objectives that may be supported by feedback reports, depending on how they aredesigned, include: Identifying clinical teams or interventions associated with high performance, which caninform improvement plans.Supporting patient care management, i.e., when patient-level data are included, byproviding access to data that enable clinicians to track whether individual patients aremeeting their specified management goals or may be overdue for specific services orfollowup care.Providing linkages and facilitating access to additional improvement-related tools andresources.Data sources used in creating feedback reports include medical records, registries, administrativeor claims databases, observations, and patient surveys. Feedback reports can be deliveredperiodically or can be designed for ongoing, real-time access if they are built into electronichealth information systems. See also related discussion in section 2-2.Confidential Physician Feedback Reports3
Ultimately the success of physician feedback reporting depends on actions taken on the basis ofthe feedback. The critical outcomes that measure success are not whether a report has been readand understood, but whether it has contributed to better care (Shaller and Kanouse, 2014). Seealso related discussion in sections 3-2 and 3-3.1-2. Do physician feedback reports work?The potential of feedback reports to support physician behavior change and performanceimprovement is well documented in the research literature. However, the size of the effect variesconsiderably across implementation contexts. In contrast, some of the more widely used medicaleducation techniques—didactic educational programs (i.e., lectures) and provision of printedtext—have little to no effect on physician behavior and performance (Bloom, 2005).A recent systematic review of randomized clinical trials examining the effect of qualityimprovement interventions that included feedback reporting compared with usual care found anoverall positive effect on measured outcomes. Particularly promising, out of 98 studycomparisons in one review, 27 showed an improvement of at least 10 percent (Ivers, et al.,2012). See illustrative case example in Text Box 2.An important conclusion emerging from the systematic review of the evidence is that, whilefeedback reporting can work, the design and manner in which feedback reports are implementedappear to have a major impact on the extent of their effectiveness.Part Two of this guide identifies evidence-based design practices, with the aim of increasing theeffectiveness of future feedback reports, nudging them toward improvement in outcomes of 10percent or more, as was the case in 27 studied interventions cited above.Text Box 2. Case study illustrating the impact of clinician feedback reporting on quality of Type 2diabetes careThe power of feedback reporting to influence professional behavior can be illustrated by the results ofa randomized, controlled trial evaluating the effect of electronic feedback reporting on the behavior ofclinicians treating patients with Type 2 diabetes. Clinicians in a Danish county caring for similar typesof diabetic patients were randomized to receive or not to receive electronic feedback on their quality ofcare. Clinicians receiving feedback showed significant improvements in care quality as measured bytheir adherence to treatment according to guidelines on evidence-based process of care. Forexample, physicians in the intervention practices succeeded in motivating their patients to fillprescribed medications for Type 2 diabetes treatments at nearly three times the rate of patients in thecontrol group (Guldberg, et al., 2011).1-3. What types of organizations develop confidential physician feedbackreports?The number and variety of organizations that develop feedback reports have greatly expandedbeyond health care providers, such as hospitals and medical groups. They also includeorganizations such as health plans, the Medicare and Medicaid programs, professional societiesand boards, and regional health improvement collaboratives. Feedback reports are also used byeducational campaigns focused on expediting the adoption of a particular new clinical advance(van der Weijden, et al., 2005; Grol, et al., 2005; Flottorp, et al., 2010).4Confidential Physician Feedback Reports
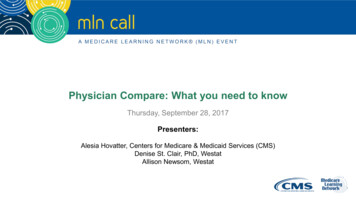
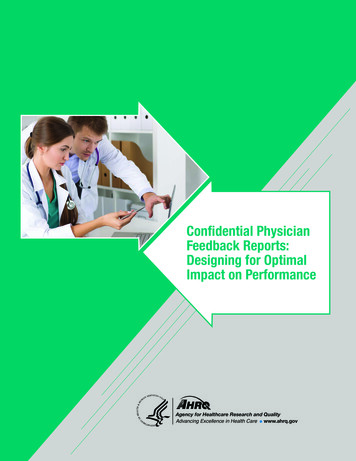
It is important to note that the “type” of developer has potential implications for the impact afeedback report might have on physician behavior. For example, the developer may be perceivedas biased toward a particular goal (e.g., reducing costs) that is not aligned with the goals of therecipient physicians (e.g., improving quality of care). In this case, the uptake of the reports maybe affected negatively (Ivers, Sales, et al., 2014). See also related discussion in section 2-4.Feedback reports developed by health care providersHospitals and large medical practices have developed data collection systems to supportperformance improvement. Feedback reports are a natural extension of such activities. SeeTtextBox 3 below.Text Box 3. Medical group perspective on the value of feedback reportsHealthPartners Medical Group (HPMG), based in Bloomington, Minnesota, consists of a network of 55clinics providing both primary and specialty care. It structures its feedback reports to provideactionable information on clinical quality, patient experience, and total cost of care. Performance onmore than 80 metrics is reported each month for each of the following levels: medical group, division,clinic location, individual physician, and individual patient. The ability to review these reports monthlyenables team members to identify both successes and missed opportunities quickly so that neededchanges can be made and then monitored. It also provides a sense of ownership so that teammembers can work together to reach their goals (contribution by Nancy Salazar, Director of CareInnovation and Measurement, HPMG, to Shaller and Kanouse, 2014).Figure 2 below displays an excerpt of a feedback report developed by HPMG, which set animprovement goal of having 62 percent of a clinic’s patients achieve the optimal vascular care(OVC) measure. The results for the top 10 clinics are listed on the left; for example, Clinic Cexceeded the goal, with 70 percent of its eligible 100 patients meeting the OVC goal. The resultsfor the top 25 physicians are listed on the right; for example, Dr. G exceeded the goal, with 88.9percent of his 36 eligible patients meeting the goal.Confidential Physician Feedback Reports5
6Confidential Physician Feedback ReportsSource: Health Partners Medical Group, 2014.*All clinics met goal.Excludes clinics with 25 patientsTop 10 Primary Clinics or Specialty Dept forVascular CarePrimary CareClinic/# Eligible% MetSpecialty 60%70%GoalCardio OVCGoalOptimal Vascular Care Measure - CardiologyPC OVCVascular Care Measure - Primary CareHPMG Vascular Care Summary*All providers met goal.Excludes providers with 10 patientsGKABEFDHIJCMNRLOSPQTXWYUVTop 25 Providers for Vascular Care# Eligible% .0%Eligible Population: All patients age 18 to 75 with a diagnosis of ischemic vascular or cardiovascular disease and 2 or more ambulatory visits inthe last 24 months and a visit for any reason in the last 12 months.Aim: To improve to 62% the percentage of patients who meet the Optimal Vascular Care by December 31, 2013.Measure: % of patients with ischemic vascular or cardiovascular disease who have had an LDL screen in last 15 months with a value 99, lastrecorded blood pressure 139 and 89, documented non-tobacco user, and documented regular aspirin use.Aims & MeasuresOptimal Vascular Care – December 2013 Summary ReportFigure 2. HealthPartners Medical Group feedback report excerpt on vascular care
Some reports developed by providers are driven exclusively by their own internal performancegoals. Others, at least in part, adopt and include metrics explicitly selected to mirror measuresused in accountability programs external to their organization. For example, measures may bebased on accreditation and certification requirements, public reports for consumers, pay forperformance targets, and national and regional campaigns to promote uptake of new clinicaldiscoveries from the field of clinical effectiveness research.When providers develop their own reports, depending on the metrics used, they may not haveaccess to data external to their organization that they need to produce performance comparisonswith others outside their organization. Such data could be an important feature in engaging andmotivating physicians. See also related discussion in section 2-3.Feedback reports developed by organizations external to providersA wide variety of organizations external to providers develop and disseminate confidentialphysician feedback reports to support improvement aims (Grol, et al., 2005). These should not beconfused with quality reports available in the public domain and designed for use by consumers.This section discusses confidential reports designed for use by physicians in assessing andimproving their performance but developed by organizations external to the provider, i.e., usingexternally sourced data. Private/public health plans and purchasers, including accountable careorganizations. Commercial insurers have access to large administrative databasescontaining utilization and financial information on affiliated physicians that can be andoften are used to develop performance reports. United Healthcare, for example, hasdeveloped a feedback report for its affiliated physicians on HEDISi measures. In thepublic sector, the Centers for Medicare & Medicaid Services (CMS) produces feedbackreports for physicians and physician groups through its Quality and Resource UseReports program. CMS also is producing feedback reports featuring key cost and qualitymetrics for its affiliated accountable care organizations.At the State level, a growing number of Medicaid agencies are producing performancefeedback reports; an informal poll of a subset of Medicaid Medical Directors identified10 State Medicaid agencies that develop some type of feedback report for affiliatedphysicians. Other State Medicaid agencies rely on the managed care organizations withwhom they contract to develop and implement feedback reports for physicians in theirnetworks (Shaller and Kanouse, 2014).Figu
includes a special focus on hospital and physician performance transparency for consumers in making health care decisions, and for physicians in assessing and improving their practices. Dale Shaller, M.P.A., Principal, Shaller Consulting Group, Minneapolis, MN. Mr. Shaller has . settings, and he was lead author of the 2012 Cochrane Review on .