Transcription
15.04.2016DisclosureThe DANCE TrialNothing to discloseChristopher D. Owens, MD, MScAssociate Professor, SurgeryUniversity of California San FranciscoDirector, Vascular Integrated Physiology and ExperimentalTherapeutics (VipeRx) Laboratory1National Co-PIsUltrasound Core LaboratoryAngiographic Core LaboratoryBiomarker LaboratorySites:DANCE: Dexamethasone delivered to theAdventitia to eNhance Clinical EfficacyDANCE Trial OrganizationGeorge Adams, MD – UNC Healthcare, Rex Hospital,Raleigh, NCGuarav Aggarwala, MD – Palestine Regional Medical,Palestine, TXSam Ahn, MD – DFW Vascular Group, Dallas, TXVaquar Ali – First Coast Cardiovascular Institute,Jacksonville, FLGary Ansel, MD – OhioHealth - Riverside Methodist,Columbus, OHEhrin Armstrong, MD – Denver VA, Denver, CONelson Bernardo – MedStar Washington HospitalCenter, DCIan Cawich, MD – Arkansas Heart Hospital, Little Rock,ARMichael Curi, MD – Rutgers Univ. Hospital – Newark, NJTom Davis, MD – St. John Providence Hospital, Detroit,MISuhail Dohad, MD – Cardiovascular ResearchFoundation, Beverly Hills, CAChristopher Owens, MD, UCSF/SFVAMCMahmood Razavi, MD, St. Joseph’s, Orange, CA Open label, single arm trial Primary endpoints:Vascore, Boston, MADirector: Michael Jaff, DOCRF, New York, NYDirector: Philippe Genereux, MDQuest Diagnostics Clinical TrialsW. Britton Eaves, MD – Willis Knighton Medical Center,Bossier City, LAAndrey Espinoza, MD – Hunterdon Medical Center,Flemington, NJRobert Feldman, MD – Munroe Regional MedicalCenter, Ocala, FLStuart Harlan, MD – Coastal Vascular & InterventionalCenter, Pensacola, FLDonald Jacobs, MD – St. Louis University Hospital, St.Louis MORichard Kovach, MD – Deborah Heart & Lung, BrownsMills, NJLouis Lopez, MD – St. Joseph Hospital, Ft. Wayne, INAmir Malik, MD – Plaza Med Ctr., Ft. Worth, TXLuke Marone, MD – UPMC, Pittsburgh, PAChristopher Metzger, MD – Wellmont Health,Kingsport, TNChristopher Owens, MD – UCSF / SFVAMC, SanFrancisco, CAJohn Pacanowski, MD – PIMA Vascular, Tucson, AZRichard Powell – Dartmouth-Hitchcock Medical Center,Lebanon, NHAnthony Pucillo, MD – Columbia Presbyterian, NewYork, NYVenkatesh Ramaiah, MD – Arizona Heart Hospital,Phoenix, AZMahmood Razavi, MD - St. Joseph Hospital of OrangeHeart & Vascular Center, Orange, CABhavanada Reddy, MD – Alpine Research, Salt LakeCity, UTAndrez Shanzer, MD – UMass Medical Ctr., Worcester,MAImmad Sadiq, MD – Hartford Hospital, Hartford CTPeter Soukas, MD – Miriam Hospital, Providence RICezar Staniloae, MD – Gotham CardiovascularResearch, New York, NYJohn Taggert, MD – Albany Vascular Group, Albany, NYRobert Wilkins, MD – Hattiesburg Clinic, Hattiesburg,MSJohn Winscott, MD – Univ of Mississippi Med Ctr.,Jackson, MSJason Yoho, MD – Mission Research - GuadalupeRegional, Seguin, TX3– Efficacy: 12 month patency (duplex ultrasound PSVR 2.4and lack of CD-TLR)– Safety: MALE through 12 months, POD through 30 days Key eligibility criteria:––––Rutherford 2-4SFA or poplitealDe novo or restenotic lesions 15 cm length 30% residual stenosis after revascularization41
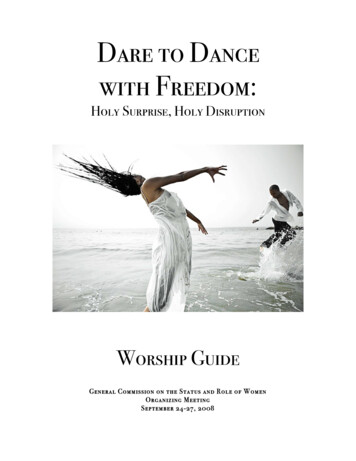
15.04.2016DANCE Trial Enrollment and DesignHow can you inhibit inflammation?1.2.3.4.Aspirin and NSAIDSMonoclonal antibodies –abs (anti-TNF)Glucocorticoid agonistResolution agonist6Inflammatory hypothesis ofrestenosisThe Bullfrog Micro-Infusion Device(Mercator MedSystems)20% contrast80% dexamethasoneCell recruitmentATVB 2011;31:15301539The Bullfrog Micro-Infusion Device is FDA 510(k)-cleared and CE-Marked7Inflammation –cytokine expressionProliferationNeointimaLumen Loss82
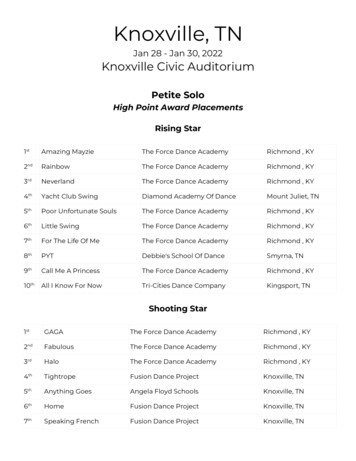
15.04.2016INVADER MRIDANCE DemographicsN73Age68.9 10.5Male52.1%Caucasian78.1%African American20.5%DiabetesCoronary artery I (kg/m2)Creatinine (mg/dL)hsCRP, baseline (mg/dL)DEX 32 mg delivered to the popliteal artery43.1%31.6 18.11.04 0.355.2 5.4910Putting DANCE into Perspectiveversus Published Drug DeliveryInterim DANCE DataInterim: 73 DANCE Atherectomy SubjectsRutherford 2Rutherford 3Rutherford 4Severe CalcificationPopliteal InvolvementTASC II ClassificationRestenosisLesion Length (cm)%DS (Pre)Total OcclusionsGrade B-D DissectionStent Utilization%DS (Post)23.3%Safety (0-360 Days)15.1%Drug-related SAE61.6%Device-related SAE26.6%Major Adverse Limb EventsAmputationBypassThrombolysis0/83 (0%)2/83 (2.4%)0/83 (0%)Death 0-360 Days5/88 (5.7%)20.5%36% A; 59% B; 6% C8.2%8.8 5.269% 17%15.4%25.0%34.2%20% 7%Death 0-30 Days0/83 (0%)0/83 (0%)0/97 (0%)Efficacy (Interim update as of 3/4/2016)TLR at 360 DaysPatency at 360 Days85.3%Patency at 390 Days82.2%TLR at 390 DaysLesion Length8.3%Ruth 4 %TASCII A:B:C %8.6%Popliteal %11Severe Ca2 %8.8 cm15.1%36:59:620.5%26.6%7.5 cm0%15.3%8.9 cm8.8 cm6.3 cm6.3 .0%6.8%5.4%7.1%7.9%9.8%8.1%7.5%123
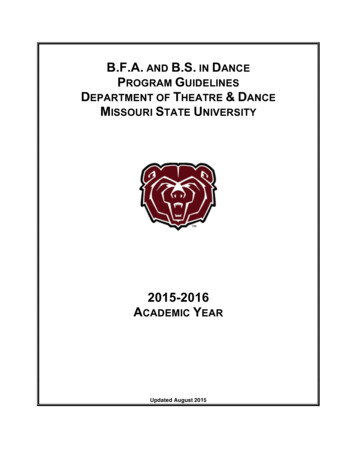
15.04.2016Novel DANCE Endpoints BiomarkersNovel DANCE Endpoints BiomarkersC-Reactive Protein (CRP)Monocyte ChemoattractiveProtein-1 (MCP-1)No DexNo Dex Circulating levels rise in response toinflammatory cytokines (e.g. IL-6)expressed in response to local triggers(e.g. inflammation) Physiologic role: bind to dead or dyingcells to activate the complement systemvia C1Q complex Elevations tied to restenosis [Schillinger etal. Radiology 2002; 225:21-26.]Bullfrog/Dex13Novel DANCE Endpoints BiomarkersMatrix Metalloproteinase-92500 Degrades extracellular matrix Short-term: aids in healing Long-term: linked withincreased neointimalhyperplasiarestenosisno restenosis140012001000800600400200**0**150014MMP9 antigen (ng/ml) before and after PCIMMP-9 PlasmaConcentration (ng/mL)2000Bullfrog/Dex Recruits monocytes, memory T cells, anddendritic cells to the sites of inflammationproduced by either tissue injury or infection Dexamethasone destabilizes the mRNAthat codes for MCP-1, shutting off itsproduction Elevations tied to restenosis [Cipollone F, etal. Arterioscler Thromb Vasc eline24 hr4 wkNon-Dex Control (DANCE-PARTNERAtherectomy, N 9)Dex Treated (DANCE Atherectomy, N 37)**P 0.05 vs prior timepoint15DES PTXDES LimusMultiple intervention164
15.04.2016Summary Next Phase: LIMBO TrialsBullfrog delivery of GR-agonist (dexamethasone) after atherectomy reducesproduction of pro-inflammatory cytokines and acute phase reactants compared toatherectomy aloneLIMBO-ATX Below-Knee 2 trials: AdventitialDexamethasone added toPTA (Germany) oratherectomy (U.S.) Anticipated start: Q1 2016The first 73 eligible patients reaching their endpoint in the atherectomy group ofDANCE have demonstrated strong patency results, with 85% remaining patent at360 days and 81.5% remaining patent at 390 daysBaseline angiogram and biomarker blood draw120 ATX (U.S.)60 controls LIMBO-PTA PI: DierkScheinert, MD, UniversityHospital Leipzig, GermanyThe DANCE trial enrolled a challenging cohort with a high representation ofRutherford 4 (15%), severe calcification (27%), popliteal involvement (21%), andTASCII B lesions (59%)The early results of GR-agonist micro-infusion in peripheral arteries at the time ofatherectomy appears promising, particularly given the inherent safety profile ofcurrently approved steroids17LIMBO-PTA60 DEX120 PTA (Germany)60 controls60 DEX24-hour blood draw for biomarkers LIMBO-ATX coPIs: GeorgeAdams, MD, UNC-Rex,Raleigh, NCDon Jacobs, MD, St. LouisUniversity, MOConclusions1-month blood draw for biomarkersClinical, hemodynamic and angiographicfollow-up at 6 monthsINVADER MRIAbout UsThe Vascular Integrated Physiology andExperimental Therapeutics (VipeRx Lab) isdedicated to creating knowledge of bloodvessels, the diseases that affect them, andimproving the quality of our patientslives. The DANCE trial is a proof-of-principle study ofendovascular adventitial delivery as an alternative tointimal-based delivery systems.Contact UsPhone: 415 750 2115Email: Christopher.Owens@UCSF.eduWeb: WWW.VipeRxLab.ORGMaking Angioplastybetter GR-agonist therapy delivered into the vessel wallproduces nuclear immunomodulation & a reduction ininflammatory biomarkers. We believe that thisrepresents a reduction in arterial tissue inflammationproducing a more physiologic healing response. But theexact mechanisms of how this might be is to be yetdiscovered.19Intimal versus Adventitial Drug Deliveryto Elucidate Mechanisms of Restenosis:Magnetic Resonance ImagingWho are we looking for?Inclusion Criteria: Questions that this study will answer Does blocking inflammation in the artery improve thedurability of angioplasty? Why do arteries close back down after treatment? Can locally applied medications improve angioplastyresults? Does the composition of the atherosclerotic plaqueinfluence the outcome of the procedure? Can we tailordrug delivery to individual plaques? Can we predict long term outcomes by the blood flowpattern through the artery immediately after theprocedure? Can we use MRI guide therapy into the arteries of theleg?Patients with peripheral artery disease and arescheduled for femoral or popliteal endovasculartreatment Patients who can tolerate a MRI examination Patients with an estimated Glomerular FiltrationRate 45 mL/min/1.73 mm2 Exclusion Criteria:Drs. Saloner and Haroldssonexamine INVADER MRI imagesWhat do we hope to find?We believe that inflammation of the arteryproduced by the angioplasty treatmentitself causes excessive scar formationand re-narrowing of the artery. By directlyinfusing Dexamethasone into the arterywall, we believe that we can block theinflammation and produce improvedoutcomes. The comparator will be apaclitaxel-coated balloon angioplasty.VIPERXLABORATORYContraindication to MRI examinations*Prior treatment of the target blockage Patients who have an estimated GlomerularFiltration Rate 45 mL/min/1.73 mm2 History of solid organ transplant Life expectancy less than one yearVIPERX LABORATORY4150 Clement StreetSan Francisco, CA 94121Physiology and ExperimentalMedicine5
15.04.2016 2 How can you inhibit inflammation? 1. Aspirin and NSAIDS 2. Monoclonal antibodies -abs (anti-TNF) 3. Glucocorticoid agonist 4. Resolution agonist DANCE Trial Enrollment and Design 6 The Bullfrog Micro-Infusion Device (Mercator MedSystems) 7 20% contrast 80% dexamethasone The Bullfrog Micro-Infusion Device is FDA 510(k)-cleared .