Transcription
Disparities in child andadolescent mental health andmental health services in the U.S.Margarita Alegría,Harvard Medical School and Center for Multicultural Mental Health Research,Cambridge Health AllianceJennifer Greif Green, Ph.D.,Boston UniversityKatie A. McLaughlin, Ph.D.,University of WashingtonA William T. Grant Foundation Inequality PaperMarch, 2015Stephen Loder, BA,Center for Multicultural Mental Health Research,Cambridge Health AllianceWilliam T. Grant Foundation 2015 Disparities in child and adolescent mental health and mental health services in the U.S.I
Disparities in child and adolescent mental health andmental health services in the U.S.Margarita Alegría, PhD, Professor, Department of Psychiatry, HarvardMedical School, and Director, Center for Multicultural Mental HealthResearch, Cambridge Health Alliance, Somerville, MAJennifer Greif Green, Ph.D., Assistant Professor in the School ofEducation, Boston University, Boston, MAKatie A. McLaughlin, Ph.D., Assistant Professor, Department ofPsychology, University of Washington, Seattle, WAStephen Loder, BA, Research Coordinator, Center for MulticulturalMental Health Research, Cambridge Health Alliance, Somerville, MAWilliam T. Grant Foundation 2015 Intersecting Inequalities: Research to Reduce Inequality for Immigrant-Origin Children and Youth
IntroductionThe Institute of Medicine’s 2009 Report on child mentalhealth (O’Connell, Boat, and Warner 2009) recommendsthat the federal government prioritize the preventionof mental, emotional, and behavioral disorders in youthbecause of the enormous toll they take on the well-beingof young people and their families, with an estimated costof 247 billion annually. Mental health care accounts formuch of the spending on health care for children (up to age12) and youth (ages 13–18), and is one of the fastest areasof spending growth in child health care. Among Medicaidpatients, the 9.6 percent of children who use behavioralhealth services account for approximately 38 percent ofchild Medicaid expenditures (Pires et al. 2013). Between2007 and 2010, use of hospital-based mental health andsubstance abuse treatment for children with employersponsored insurance increased 24 percent, while use ofpsychiatric medications increased by almost 10 percent(Health Care Cost Institute 2012). The high individualburden and systemic costs due to child behavioralhealth problems underscore the need for more efectiveprevention eforts for children at risk of developingbehavioral health problems, but also raise the criticalissue of mental health equity for low-income and racialand ethnic minority children and youth.onset ampliies the importance of a developmentalperspective in understanding trajectories of mental healthand mental health service use. Results from the NationalComorbidity Survey-Adolescent Supplement (NCS-A)indicate that approximately half of respondents ages13–17 (48.3 percent of Latinos, 46.8 percent of blacks and41.9 percent of non-Latino whites) experienced a mentalhealth disorder before age 18, with 7 percent reportingserious emotional disturbance (i.e., disorders thatsigniicantly impaired their functioning in the past year)(Merikangas, He, and Burstein et al. 2010). In addition,psychiatric disorders in the NCS-A were associatedwith an increase in health risk behaviors and decreasededucational achievement (Merikangas, He, and Bursteinet al. 2010). For example, risk for smoking increases 9-foldin non-Latino white adolescents with serious emotionaldisturbance (SED) and over 25-fold in Latino adolescentswith (SED), indicating a possible diferential impactof psychiatric conditions by race and ethnicity. Earlyidentiication and intervention can therefore reducethe morbidity of psychiatric disorders, preventing thedevelopment of comorbid psychiatric conditions andattenuating their impact on functioning (Merikangas andAmes et al. 2007).Mental health is recognized as a central determinantof individual well-being, family relationships, andengagement in society (Wulsin and Singal 2003; Scott,Von Korf, and Angermeyer et al. 2011; Kessler, Walters,and Forthofer 1988; Breslau et al. 2011). Still, nearly 40-50percent of the U.S. population develops a mental disorderin their lifetime (Kessler et al. 2005; Kessler, McGonagle,Zhao et al. 1994). Most psychiatric disorders have an onsetin childhood or adolescence, increasing the risk for poorphysical health, problems in social relationships, reducedpsychological well-being, and inancial diiculties(Kessler et al. 2005). The relatively early age of disorderEvidence consistently suggests that, across the life course,mental disorder prevalence varies signiicantly accordingto race and ethnicity (Breslau et al. 2006; Alegría et al.2007; Williams and Earl 2007; Breslau et al. 2005), buta prominent scholar in this area recently noted that thisliterature has raised more questions than it has answeredbecause of two pervasive limitations (Williams and Earl2007). First, remarkably few studies have investigated themechanisms that underlie racial and ethnic disparities inmental health. Second, decomposition shows that racialand ethnic minorities are at elevated risk of persistentmental disorders in adulthood (Breslau et al. 2005;William T. Grant Foundation 2015 Disparities in child and adolescent mental health and mental health services in the U.S.1
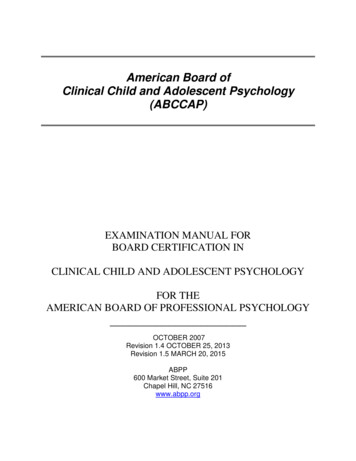
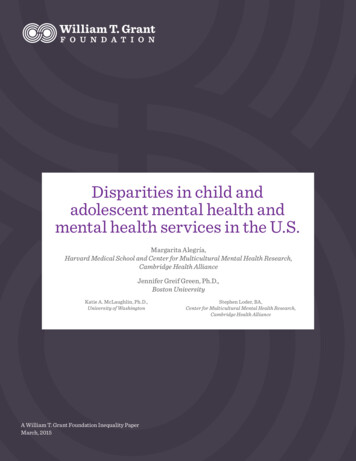
Williams, Gonzalez, and Neighbors et al. 2007), eventhough they demonstrate similar or lower prevalencerates in adolescence (Merikangas, He, and Bursteinet al. 2010). For example, although African-Americanchildren and adolescents are less likely to develop lifetimemajor depression than non-Latino whites as adults,their depression is signiicantly more likely to develop achronic course (Chatterji, Alegría, and Takeuchi 2009).This suggests that the efects of some risk factors mightaccrue incrementally over time to impede recovery frommental disorders (Gee and Payne-Sturges 2004), and alsohighlights the importance of research disentangling theassociations of race and ethnicity with diferent stages ofdevelopment for targeting interventions.In this paper, we focus on four mechanisms (see Figure1) possibly responsible for these disparities in mentalhealth outcomes as minority children and adolescentstransition into adulthood: (i) socio-economic status (e.g.,low education and income); (ii) childhood adversities(e.g., maltreatment, family violence); (iii) family structureacross development (e.g., single motherhood, earlychild-bearing, divorce, paternal involvement); and (iv)neighborhood-level factors (e.g., residential composition,stability, and segregation). Not only does exposure to thesefactors vary by race and ethnicity, but their efects mightdifer along the same lines.We also discuss the potential role of individual andneighborhood-level protective factors (e.g., social support,religiosity, neighborhood stability) as bufers against thenegative efects of these risk pathways. We then examinebarriers to mental health care that may lead to untreatedor poorly treated mental illness for minority childrenand youth, and propose a research agenda focused oninterventions that target the underlying mechanisms ofmental health and mental health service disparities.Throughout this review we adopt a developmentalperspective. This approach is consistent with researchindicating that rapidly developing biological systems ofchildren and adolescents are shaped by life experiences,which subsequently interact to inluence health andmental health trajectories (Mistry, Minkovitz, Riley etal. 2012). A framework developed by the Harvard Centerfor the Developing Child provides a particularly usefulstructure for examining these transactional relationshipsin the context of key social, cultural, and economic factors(Mistry, Minkovitz, Riley at al. 2012; Center on theDeveloping Child 2010).Figure 1: Conceptual Model for Child Mental Health and Mental Health Service DisparitiesProtective FactorsAdult SESReligiosity, Social andEmotional SupportEarnings, Educational Attainment for Self and Partner,Occupation, Perceived Social Class, Relative DeprivationChildhood SESParent Education,Parent Occupation,Food InsecurityRace/EthnicityDisorder PersistenceChildhood AdversityMaltreatment,Parent Maladjustment,Trauma ExposureMental Disorder OnsetFamily StructureFemale-Headed Household,Extended Family,Parent Marital StatusDisorder SeverityBarriers to TreatmentNeighborhood Risk and Protective FactorsFederal and State Government PoliciesNeighborhood Income and Composition, Income Inequality,Residential Stability, SegregationInsurance availablity/eligibility requirements, tax credits, socialservices, criminal justice involvement, immigration enforcementPsychosocial DevelopmentWilliam T. Grant Foundation 2015 Disparities in child and adolescent mental health and mental health services in the U.S.2
Four Mechanisms for DisparitiesThe Diferential Role ofSocio-Economic Status (SES)in Mental Health Outcomes byRace and EthnicityPervasive diferences in family SES exist for childrenof diferent racial and ethnic groups in the U.S. Theproportion of black (39 percent) and Latino (33 percent)children and adolescents living in poverty is more thandouble that of non-Latino whites (14 percent) and Asians(14 percent) (Kids Count Data Center, Children in Poverty2014). As such, social class diferences are frequentlyposited to be a central factor explaining racial andethnic disparities in mental health outcomes. Indeed, inThe Declining Signiicance of Race, Wilson argued thatsocial class has become a more important predictor ofopportunity and life experiences for black Americans thanrace (1980). However, this argument is far from universallyaccepted and, in fact, has spurred controversy regardingthe relative importance of race and ethnicity versus SESin shaping social, economic, and health outcomes (Farmerand Ferrarro 2005; Hughes and Thomas 1998).Instead of seeing SES as the sole cause of disparities,recent theoretical models have taken an intersectionalapproach that views SES as interacting with a number ofother social and environmental factors to cause healthdisparities. Myers ofers an excellent example of this typeof model (2009). He argues that SES is the single mostimportant factor underlying racial and ethnic disparitiesin health because it leads to diferences in material andpsychological resources, environmental and behavioralrisks, and diferences in access to health care. However,Myers also emphasizes that many racial and ethnic healthdiferences are not explained by SES and concludes thatdisparities should be seen as resulting from a complexinteraction of factors (2009), including poverty andminority status.Kessler and Neighbors carried out secondary analysesof eight epidemiologic surveys and demonstrated thatfailure to test for race-by-SES interactions resultedin an underestimation of the efect of race and anoverestimation of the efect of SES in predictingnonspeciic psychological distress (1986). Studiesaddressing the controversy over the degree to whichSES causes racial and ethnic health outcome disparitieshave examined the mediating role of SES in explainingdisparities in various physical disorders (Farmer andFerraro 2005; Williams 1999, Feagin 1991), as well as inmental health outcomes (Williams, Takeuchi, and Adair1992). Findings typically show that disparities are reduced,but not eliminated, after accounting for SES, and thatthe efect of SES sometimes varies by race and ethnicity(Farmer and Ferraro 2005; Williams 1999). For example,Williams and colleagues examined the relationshipbetween SES and current and lifetime rates of mentaldisorder among black and white adults and found thatwhile depression was unrelated to SES among blacks,it was negatively related to SES among whites, leadingto variation in the association of race with depressiondepending on SES (Williams, Takeuchi, and Adair 1992).Interestingly, income was unrelated to either current orlifetime depression among black males in that study, whileeducation was a more critical element for understandinghow SES relates to mental health (Williams, Takeuchi,and Adair 1992). This is striking because most theoriesof the importance of SES for racial and ethnic disparitiesin health emphasize inancial resources, whereas theinding that education is a key component of SES formental health suggests its role in building cognitiveresources. Roberts et al. also examined racial and ethnicWilliam T. Grant Foundation 2015 Disparities in child and adolescent mental health and mental health services in the U.S.3
diferences in depression and reported that while lowSES was associated with depression, only MexicanAmerican adolescents had signiicantly higher rates ofdepression after controlling for SES and other factors(Roberts RE., Roberts CR., and Chen 1997). Interventionimplications could vary dramatically depending on therelative importance of these aspects of SES, making itcritical to determine what aspects are associated withmental disorders by race and ethnicity for children andadolescents of color.and mental health outcomes. Future research shouldemploy models such as the Integrative Model for the Studyof Developmental Competencies in Minority Children(Coll, Crnic, Lambert et al. 1996), developed by GarcíaColl and colleagues, which emphasizes the central role ofminority status in how children perceive their world and,consequently, their social position. Minority status, as wellas experiences with prejudice, discrimination, racism, andoppression, can impact one’s self-worth and, thus, mentalhealth outcomes.Previous research has shown that perceptions of one’sstatus in society—termed subjective social status—areassociated with health independent of income or education(Goodman, Slap, and Huang 2003; Murphy and Athanasou1999; Repetti, Matthews, and Waldron 1989). Indeed,numerous studies have documented associations betweenperceived social status and mental health disorders,particularly depression and anxiety (Goodman, Slap,and Huang 2003; Murphy and Athanasou 1999; Repetti,Matthews, and Waldron 1989; Felitti, Vincent, and Adnaet al. 1998; Chapman et al. 2004; Edwards et al. 2003).However, measures commonly used to operationalizesocial position (e.g., income, education, occupation, andclass) do not encompass the range of socio-culturalfactors associated with perceived social position (Kessler,Davis, and Kendler 1997). Status characteristics at theindividual level—attributes such as ethnicity and race,or, more importantly, minority status, education, income,nativity, and the corresponding values attached to theseattributes—are not only outward markers of social status,but factors in determining how the individual decipherssocial location in society (Murphy and Athanasou 1999;Mullen at al. 1996; Collishaw 2007). Among childrenand adolescents, parental education and occupation(Goodman, Slap, and Huang 2003; Johnson et al. 1999;Goodman 1999), employment (Murphy and Athanasou1999; Repetti, Matthews, and Waldron 1989), and socialmobility (Das-Munshi et al. 2012) are related to mentalhealth outcomes even after controlling for income,although variation in residual efects has not beenexamined systematically by race and ethnicity. There isreason to believe that the efect of income and perceivedsocial status on mental health outcomes might diferby race and ethnicity (Johnson et al. 1999), althoughthis possibility has seldom been considered in previousquantitative studies of the extent to which SES mediatesor modiies the association between race and ethnicityOther studies have found that the link between raceand socioeconomic status in children is complex anddiicult to measure. For example, multiple studies havefound that the relationship between both subjectiveand objective measures of SES and poor mental healthseems to be strongest for white children and adolescents.A study of the efects of poverty on the mental healthoutcomes of rural black and white children found thatthe association between poverty and psychopathologywas stronger for white children, but that multiple moves,lack of parental warmth, and lax supervision were moreimportant predictors of child mental health problemsthan SES (Costello, Keeler, and Angold 2001). In areview of literature on race, ethnicity, and poverty onchild mental health, Samaan concluded that childrenand adolescents from some non-white racial and ethnicgroups may have a lower likelihood of developing mentalhealth problems than white children and adolescents ofthe same SES, and speculated that cultural factors mayinluence behaviors and perceptions associated with SES(2000). Another recent study looking at the relationshipbetween SES, subjective social status, and adolescentmental disorders found that documented associationsbetween mental disorders and SES are most directly dueto diferences in subjective social status for white andLatino adolescents, but that neither SES nor subjectivesocial status were associated with mental disordersamong black youth (McLaughlin et al. 2012). In addition,measures of SES may inluence health through diferentpathways (Galobardes et al. 2006; Krieger, Williams, andMoss 1997), highlighting the importance of consideringmarkers of social status, such as material deprivation orfood insecurity, that go beyond a simple income measure(Melchior, Caspi, Howard et al. 2009).William T. Grant Foundation 2015 Disparities in child and adolescent mental health and mental health services in the U.S.4
The Diferential Role ofChildhood Adversities (CAs) inMental Health Outcomes byRace and EthnicityAdverse childhood experiences are importantdeterminants of mental disorders (Felitti, Vincent, Andaet al. 1998). Exposure to early toxic stress, includingmaltreatment, family violence, and parental instability,has immediate and lasting disruptive efects onphysiological development, health, and mental health(Chapman et al.; Kessler, Davis, and Kendler 1997;Shonkof 2012; Shonkof, Garner, Siegel et al. 2012).Retrospective studies consistently identify higher ratesof these childhood adversities among individuals witha mental disorder (Edwards et al. 2003; Kessler, Davis,and Kendler 1997), and this link has been conirmed byprospective studies (Fergusson, Horwood, and Lynskey1996; Finkelhor, Ormrod, Turner et al. 2007). Importantly,CAs are associated with new disorder onsets in adulthood(Jafee et al. 2002; Green, McLaughlin, Berglund etal. 2010), even after accounting for disorders withearly-childhood onset, as well as with persistence andseverity of mental disorders (McLaughlin et al. 2010). CAsare important from a public health perspective becausethey are common in minority populations (Kessler,Davies, and Kendler 1997; Finkelhor, Ormrod, Turneret al. 2007; Gree, McLaughlin, Berglund et al. 2010).They also strongly predict mental disorders (Fergusson,Horwood, and Lynskey 1996; Cohen, Brown, and Smailes2001; Molnar, Buka, and Kessler 2001), and account fora substantial proportion of mental disorders (up to 30percent) (Green, McLaughlin, and Berglund et al. 2010).CAs also predict role constellations that may driveracial and ethnic disparities in mental health outcomes,including teenage pregnancy (Fergusson, Horwood, andLynskey 1997; Hillis et al. 2004), marital instability anddivorce (Nelson, Heath, Madden et al. 2002), and singleparenthood (Roberts et al. 2004). National data suggestthat racial and ethnic minorities have high rates of CAexposure (Turner, Finkelhor, and Ormrod 2006; Finkelhorand Asdigian 1996). This diferential exposure has beeninvoked as a potential explanation for ethnic and racialdisparities in mental health outcomes (Williams andCollins 1995), but little empirical research has directlyexamined this possibility in children—a critical omissiongiven the importance of the timing of CAs (Braveman andBarclay 2009; Shonkof 2012).One hypothesis, supported by a growing body ofevidence, is that these factors contribute to disparitiesslowly over the course of an individual’s life, througha process of “weathering (Gee and Payne-Sturges2004).” Thus, disparities can be seen as resulting inpart from “cumulative adversity” due to factors thatdisproportionately afect minorities (including childhoodtrauma, stress, pollution, poor housing, lack of education,low SES, exposure to community violence, and others) orcultural hardship (discrimination, prejudice, stereotyping,unfairness, sense of not belonging) that, over the long term,cause poor health and mental health outcomes (Keinan,Shrira, and Shmotkin 2012). While cumulative adversitycan be diicult to measure, studies have documentedassociations between prolonged exposure to adverseconditions, particularly during childhood, and risk formental illness (Ford, Clark, and Stansfeld 2011). MRIstudies have even documented possible neurophysiologicdiferences associated with cumulative adversity(Ansell et al. 2012). But less has been documented oncultural diiculties and how they impact mental healthby encapsulating commonly held views about socialstratiication that afect how one experiences socialposition as a minority.The Diferential Role of FamilyStructure in Mental HealthOutcomes by Race and EthnicityIn The Truly Disadvantaged, Wilson argues that U.S.macro-social and economic trends have led to changesin family structure for racial and ethnic minorities,including a dramatic increase in single-headed households,and that these changes are a primary contributor toincreases in concentrated urban poverty and a wide rangeof social problems in high-poverty neighborhoods (1987),many because of a lack of institutional supports. Thisargument has been supported by numerous studies sinceWilson’s seminal work was published (Dupéré, Leventhal,and Lacourse 2009; Mair, Roux, and Galea 2008; Xue et al.2005; Cassiano and Massey 2008). However, few studieshave examined the contribution of family structure, roleconstellations, or changes in those structures across thelife course as a contributor to racial and ethnic disparitiesin mental health outcomes of children and youth.Family structure may contribute to mental healthdisparities through a variety of pathways. First, familystructure is strongly related to exposure to CAs. Childrenliving in single-parent homes and in step-families, forexample, are more likely to experience maltreatment,family violence, parental instability, and a range of otherWilliam T. Grant Foundation 2015 Disparities in child and adolescent mental health and mental health services in the U.S.5
traumatic events in childhood than children living withboth biological parents (Brown and Moran 1997; Wang2004). Indeed, data from the Justice Bureau suggest thatliving in a single-headed household is among the strongestrisk factors for child victimization (Wang 2004) andelevated risk for behavior problems over and above theefects of SES (Sampson, Raudenbush, and Earls 1997),although we are unaware of systematic research on theextent to which this is equally true for various racial andethnic minority groups.Second, being raised in a single-headed household isassociated with subsequent role conigurations inadolescence, including teenage pregnancy, maritalinstability, divorce, and single parenthood (Fergusson,Herwood, and Lynskey 1997; Ellis, Bates, Dodge et al.2003), that may further contribute to mental healthdisparities (Molina, Alegría, and Chen 2012). Analysisof data from the National Comorbidity Replication(NCS-R) revealed that childhood adversities relatedto parental mental illness, substance abuse, familyviolence, physical abuse, sexual abuse, and neglect weremost strongly correlated with onset of mental illness,but that no particular factors within this grouping weremore signiicant when considered individually (Green,McLaughlin, Berglund et al. 2010). One study examiningthe relationship between socioeconomic status, residentialstability, and family disruption found that 3 or more moves(residential instability) or parental separation or divorce(family disruption) before the age of 7 increased risk ofmajor depression independently of socioeconomic status,and that this efect was most pronounced for depressionwith onset by age 14 (Gilman et al. 2003). Furthermore,both residential instability and family disruption wereassociated with increased recurrence and lower likelihoodof remission of major depression (Gilman et al. 2003). Asubstantial literature, moreover, has documented strongassociations between being a single parent and risk fordepression among minority mothers (Brown and Moran1997; Wang 2004).Given evidence of increased risk for childhood adversitiesand of mental health problems among children of parentswith mental disorders (Weissman, Gammon, John etal. 1987; Goodman and Gotlib 1999), there is reason tosuspect a link between family structures and disparitiesin children’s mental health outcomes. In terms offathering roles, data from the longitudinal National ChildDevelopment Study suggest that father involvement atthe age of seven serves to protect against adolescentpsychological distress in non-intact families (Flouriand Buchanan 2003). As an increasing number of U.S.families include unmarried parents, understandingfather involvement and co-parenting dynamics isparticularly important (McHale, Waller, and Pearson2012; Cabrera et al. 2007). Yet there has not been acomprehensive assessment of whether the efects ofrole constellations vary across racial and ethnic groups,although some evidence suggests that the adverse efectsof disadvantaged role constellations difer by race andethnicity (Cohen et al. 1992; Thomas, Farrell, and Barnes1996). This is especially signiicant given that 67 percentof Black children and 42 percent of Latino children live insingle-parent households, compared with only 25 percentof non-Latino whites, according to data from the 2012American Community Survey (Kids Count Data Center,Children in Single-parent Families 2014). This suggeststhe importance of institutional supports to facilitateco-parenting to contend and reduce the opportunities forchildhood adversity.The Diferential Role ofNeighborhood-level Factorsin Mental Health Outcomes byRace and EthnicityConsistent evidence shows that socio-ecological context isan important predictor of the prevalence and diferentialcourse of mental disorders (Dupéré, Leventhal, andLacourse 2009; Mair, Roux, and Galea 2005; Xue et al.2005). As ethnic minorities disproportionately reside inhigh-poverty, segregated neighborhoods with high levelsof concentrated disadvantage (Casciano and Massey2008; Williams and Collins 2001), understanding thecontribution of neighborhood context as a mechanismfor explaining disparities in mental health outcomesis particularly critical. Indeed, Williams argues thatresidential segregation is a central social determinantof racial and ethnic disparities in health outcomes(Williams and Jackson 2005). Research on such efectsexists in the literature on health disparities involvingphysical disorders. For example, Morenof et al. foundthat pronounced racial and ethnic disparities in adulthypertension became non-signiicant when adjustingfor indicators of neighborhood context (e.g., economicdisadvantage, aluence and gentriication, racial andethnic composition, and age composition) (2007). Theextent to which neighborhood context explains ethnic andracial disparities in mental health outcomes for childrenand adolescents is mostly unknown, but we do knowthat neighborhood context inluences ethnic and racialinequities in education, access to formal and informalinstitutional structures, social norms, and exposure toWilliam T. Grant Foundation 2015 Disparities in child and adolescent mental health and mental health services in the U.S.6
a variety of risk factors ranging from violence and crimeto ambient noise (Sampson, Raudenbush, and Earls 1997;Sampson, Morenof, and Gannon-Rowley 2002)—all ofwhich are associated with mental disorders in childrenand adults.Numerous ecological models of mental health havebeen proposed in an attempt to map out the relationshipbetween social and environmental context and mentalhealth, but most focus on several key areas. Gee andPayne-Sturges clearly outline three primary waysin which neighborhood context can afect health: (1)structural factors, such as tax incentives, zoning laws, andinfrastructure investment; (2) psychosocial conditionssuch as social disorganization, crowding, discrimination,economic deprivation, and crime; and (3) neighborhoodresources, which include factors such as the concentrationof political power, social capital, and a sense of collectiveeicacy (the existence of mutual trust allowing forcoordinated group action to solve a problem) (2004). Someof these factors can beneit minority communities andcontribute to well-being of minority children (i.e. zoninglaws that improve housing quality and enable greateraccess to space for recreation), while others may negativelyimpact health and mental health (i.e. negative psychosocialconditions). For example, discrimination related stressorssuch as federal and local immigration policies, extensiveworkers’ rights abuses, and marginalization have beenrelated to psychological distress (Negi 2013).Research into the relationship between neighborhoodcontext and mental health has revealed several potentialmechanisms for mental health disparities. Dupéré et al.tested the relationship between neighborhood context,self-eicacy, and adolescent mental health amongadolescents in Chicago and found that adolescents livingin violent neighborhoods reported lower self-eicacydue to fear, and that this led to more internalizingbehavior problems (Dupéré, Leventhal, and Vitaro2012). Those adolescents who moved to less violentneighborhoods, however, showed greater self-eicacy andlower internalizing behavior problems. A similar socialexperiment studying the efects of living in low-incomeneighborhoods found that the menta
of i247 billion annually: Mental health care accounts for much of the spending on health care for children Wup to age 12X and youth Wages 13Q18X; and is one of the fastest areas of spending growth in child health care: Among Medicaid patients; the 9:6 percent of children who use behavioral