Transcription
C E N T E R F O R H E A LT H S Y S T E M S E F F E C T I V E N E S SIssue Brief July 2018Oregon’s Effort to Reduce HealthDisparities Shows Signs of Early SuccessVast and pervasive health care disparities existfor most racial and ethnic minorities across theUnited States. Reducing health disparities was akey part of Oregon’s Medicaid reforms.McConnell KJ, CharlesworthCJ, Meath THA, et al. Oregon’sEmphasis On Equity ShowsSigns Of Early Success ForBlack And American IndianMedicaid Enrollees. Health Affairs.2018;37(3):386-393.Access to full articleMedicaid reform offers opportunities to addresshealth care disparities.Across the country, large differences in health and health care qualityexist among racial and ethnic groups. The average life expectancy forOregonians who identified as black, American Indian, or Alaska Nativewas two years lower than for those who identified as white in 2011, andmore than 35 percent of minority women in Oregon had no regular careprovider, compared with 18 percent of white women, in the same year.1Policymakers have begun using Medicaid reform as a tool to combatsuch disparities. Medicaid covers nearly 20 percent of the United Statespopulation, including a relatively large proportion of racial or ethnicminorities. 2This study evaluated the impact of Oregon’s Medicaid reforms onhealth disparities. The study team tracked disparities in health care useand quality between black and white enrollees, and between AmericanIndian/Alaska Native and white enrollees, before and after Oregon’sreform efforts began. They tracked measures of health care qualityand service use where a disparity existed prior to Oregon’s reforms,and used health care claims data from Oregon’s Medicaid program todetermine whether the disparities narrowed or widened following theintroduction of health equity policies in the state.KEY FINDINGS Disparities in primary careuse between black and whiteenrollees, and betweenAmerican Indian/AlaskaNative and white enrollees,narrowed significantly afterthe health equity policies wereintroduced. Disparities in access topreventive services betweenblack and white enrollees alsonarrowed significantly. Disparities in emergencydepartment use betweenblack and white enrollees, andbetween American Indian/Alaska Native and whiteenrollees, did not changesignificantly after the healthequity policies wereintroduced.Issue Brief July 20181
Medicaid reform may addresshealth disparitiesImportanceof MedicaidMedicaid coversalmost 20pecent of theUS population,including arelatively largeproportion ofracial and ethnicminorities.Across the country, large differences inhealth and health care quality exist amongracial and ethnic groups. For example, theaverage life expectancy for Oregonianswho identified as black, American Indian,or Alaska Native was two years lower thanfor those who identified as white in 2011,and more than 35 percent of minoritywomen in Oregon had no regular careprovider, compared with 18 percent of whitewomen, in the same year.1 Such disparitieshave become an important concern forpolicymakers.Medicaid reform offers opportunities toaddress health disparities. Medicaid coversalmost 20 percent of the United Statespopulation, and a substantially higher share insome states, including Oregon. 2 A relativelyhigh proportion of racial and ethnic minoritiesreceive health care coverage throughMedicaid, and racial and ethnic healthcaredisparities are particularly acute amongMedicaid recipients. States have a great dealof flexibility to design aspects of Medicaidprograms, and they are experimentingwith reforms to improve care and controlspending. These efforts may also provideopportunities to address health disparities.Oregon’s Medicaid reformstargeted health disparitiesIn 2012, Oregon established coordinatedcare organizations (CCOs) to serve asthe single point of accountability for thehealth care and outcomes of Medicaidmembers. CCOs were locally governed, withrepresentation from Medicaid members,health care providers, and other localstakeholders. They received a global budgetthat covered physical, behavioral, andoral health care services, and they wereresponsible for coordinating and integratingthese services.Oregon implemented specific policies to helpCCOs address health disparities: The state required each CCO to developand implement a transformation plan thatincluded efforts to reduce racial and ethnicdisparities among enrollees. CCOs were encouraged and given supportto stratify health care access and qualitymeasures by race and ethnicity. Oregon established Regional Health EquityCoalitions—community-led, regionallyorganized groups that provided CCOs withguidance on reducing disparities in theircommunities. Oregon trained and certified over 400community health workers. Communityhealth workers typically share race,ethnicity, or language with those theyserve, and help to form a bridge betweenlocal health care services and thecommunities in which they operate.Combined, these strategies were intendedto help CCOs reduce health disparities incommunities they served.CCOs were associated withreductions in some disparitiesTo understand the impact of CCOs onhealth care disparities, the study teamtracked disparities in health care qualityand access measures between black andwhite enrollees, and between AmericanIndian or Alaska Native (AI/AN) and whiteenrollees. The team focused on black andAI/AN enrollees because they experiencedthe most prominent disparities in health carequality and access (relative to other nonwhite minority groups) in the years beforethe establishment of CCOs.The study team selected eight measures ofhealth care service use and quality wheresignificant disparities existed before CCOswere established. They calculated eachmeasure using data from Oregon’s Medicaidprogram. They then compared the sizeIssue Brief July 20182
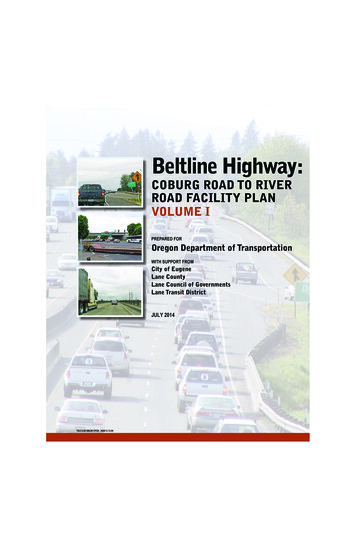
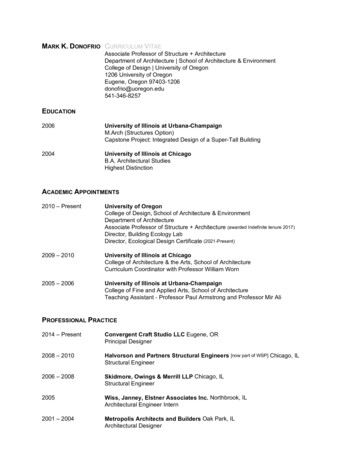
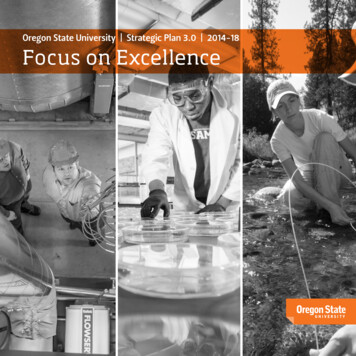
of the disparity between black and whiteenrollees, and between AI/AN and whiteenrollees, in the years 2010 and 2011 (thepre-CCO period) to the years 2013 and2014 (the post-CCO period). The study teamused statistical techniques to control for theeffect of factors other than the introductionof CCOs, such as geography and healthconditions, on measures.Disparities in access to primary care andother outpatient services narrowedDisparities in use of primary care and otheroutpatient services between black and whiteenrollees, and between AI/AN and whiteenrollees, decreased substantially from thepre-CCO period to the post-CCO period.Most notably, the disparity in primary carevisit rates between black and white enrolleesnarrowed by one-third, from a differenceof 40 visits per 1,000 member months to25 visits per 1,000 member months (Figure1). However, use of primary care and otheroutpatient services among black and AI/ANenrollees remained lower than among theirwhite counterparts.The disparity in access to preventive servicesbetween black and white enrollees alsonarrowed substantially from the pre-CCOperiod to the post-CCO period. Such adisparity did not exist between AI/AN andwhite enrollees before the establishment ofCCOs.Disparities in emergency departmentuse persistedThe disparity in emergency department (ED)use between black and white enrollees, andbetween AI/AN and white enrollees, didnot change substantially from the pre-CCOperiod to the post-CCO period (Figure 2).While the ED visit rate declined amongblack, AI/AN, and white enrollees, disparitiesbetween black and AI/AN enrollees and whiteenrollees did not change substantially.ImplicationsThe establishment of CCOs was associatedwith reduced disparities in use of primarycare between black and white enrollees,and between AI/AN and white enrollees.Concurrently with CCOs, Oregon adoptedspecific policies to raise awareness ofdisparities and encourage CCOs to addressthese disparities. Evidence from Oregonsuggests that these strategies may helpother states address health disparities in theircommunities.The establishment of CCOs was notassociated with a reduced disparity in EDuse. While the ED visit rate declined amongFigure 1. The disparity in primary care visitrates between minority and white enrolleesdecreased substantially from before CCOsto after CCOs.Figure 2. The disparity in emergencydepartment visit rates between minority andwhite enrollees did not change substantiallyfrom before CCOs to after CCOs.However, the primary care visit rate was still higherfor white enrollees than for minority enrollees afterCCOs.Emergency department visit rates fell for all groupsfrom before CCOs to after CCOs, but the gapbetween groups did not narrow .9Black-20-2.9-104.8AI/AN0016.06.01020304050Visit rate visits per 1,000 member months. Disparity in visit rates rate for black and AI/AN enrollees minus rate for white enrollees.Issue Brief July 20183
black, AI/AN, and white enrollees, disparitiesbetween black and white enrollees, andbetween AI/AN and white enrollees, didnot narrow substantially from the pre-CCOperiod to the post-CCO period. This suggeststhat reducing the number of visits made tothe ED may not be tied directly to increasingprimary care use, at least in the populationwe studied. States may need to employdiverse strategies to address disparities indifferent aspects of health care use andquality.Many health care quality and outcomemeasures are available to help states monitorand address health disparities. Selecting theright measures for each state will dependon its Medicaid population and priorities foraddressing disparities. An important task forOregon and other states will be continuingto refine their choice of metrics to use inmonitoring and incentivizing efforts to reducedisparities.Issue Brief July 20184
REFERENCES1 Oregon Health Authority. Oregon HealthCare Innovation Plan. Oregon HealthAuthority; 2012. s/Oregon%20Health%20Care%20Innovation%20Plan.pdf.2 Berchick E, Hood E, Barnett J. HealthInsurance Coverage in the United States:2017. United States Census Bureau; rary/publications/2018/demo/p60-264.pdf.C E N T E R F O R H E A LT H S Y S T E M S E F F E C T I V E N E S SWritten by Anna Levy of the Center for Health Systems EffectivenessCite as: Levy A. Oregon’s Effort to Reduce Health Disparities Show Signs of Early Success. Center for Health SystemsEffectiveness, Oregon Health & Science University; 2018.Original article: McConnell KJ, Charlesworth CJ, Meath THA, George RM, Kim H. Oregon’s Emphasis On EquityShows Signs Of Early Success For Black And American Indian Medicaid Enrollees. Health Affairs. w.ohsu.edu/chse CHSE-info@ohsu.edu @OHSU CHSEIssue Brief July 20185
Vast and pervasive health care disparities exist for most racial and ethnic minorities across the United States. Reducing health disparities was a key part of Oregon's Medicaid reforms. Medicaid reform offers opportunities to address health care disparities. Across the country, large differences in health and health care quality