Transcription
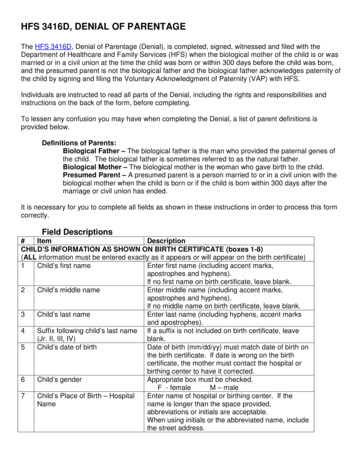
HFS Dental Program Fee Schedule for Children and Adult BeneficiariesEffective January 1, 2021All services not covered are noted as N/A and will not have prior authorization requirementProcedureCodeDescriptionD0120Periodic Oral Exam – Ages 0 thru 20D0120Periodic Oral Exam – Ages 21 and older and Pregnant WomenD0140Limited Oral Examination – Problem FocusedD0150Comprehensive Oral ExaminationD0210Intraoral-Complete Series (including bitewings)D0220Intraoral – periapical – first filmD0230Maximum Prior Approval dultsUpdated December 29, gnantWomenPrior ApprovalRequiredPregnantWomen 28.00NN/AN/AN 28.00N 28.00N 16.20N 16.20N 16.20N 21.05N 21.05N 21.05N 30.10N 30.10N 30.10N 5.60N 5.60N 5.60NIntraoral periapical – 1 additional film 3.80N 3.80N 3.80ND0270Bitewings Single Film 5.60N 5.60N 5.60ND0272Bitewings-Two Films 9.40N 9.40N 9.40ND0274Bitewings-Four Films 16.90N 16.90N 16.90ND0277Vertical Bitewings – 7-8 Films 16.90N 16.90N 16.90ND0330Panoramic Film 22.60N 22.60N 22.60ND0601Caries Risk Assessment - Low Risk 0.00N 0.00N 0.00ND0602Caries Risk Assessment - Moderate Risk 0.00N 0.00N 0.00ND0603Caries Risk Assessment - High Risk 0.00N 0.00N 0.00ND0999By ReportNBy ReportNBy ReportND1110Encounter Rate Code (Rate is Determined Annually By Encounter Clinic)(Must be onfirst line of all Encounter Clinic Claims)Prophylaxis - Adult - Ages 21 and Older and Pregnant WomenN/AN 41.00N 41.00ND1120Prophylaxis - Child – Ages 0 thru 20 41.00NN/AN/AD1206Topical Fluoride Varnish - Ages 0 thru 18 26.00NN/AN/AD1206Topical Fluoride Varnish - Ages 19 thru 20 26.00NN/AN/AD1208Topical Application of Fluoride (excluding prophy) – Ages 0 thru 18 26.00NN/AN/AD1208Topical Application of Fluoride (excluding prophy) – Ages 19 thru 20 26.00NN/AN/AD1351Sealant – Per Tooth 36.00NN/AD1354Interim Caries Medicament – per tooth - Silver Diamine 14.85N 14.85D1510Space Maintainer - Fixed Unilateral 70.60NN/AN/AD1516Space Maintainer – fixed – bilateral, maxillary 103.50NN/AN/AD1517Space Maintainer – fixed – bilateral – mandibularSpace Maintainer – Removable Unilateral 103.50NN/AN/A 70.60NN/AN/AD1520N/AN/AN 14.85N
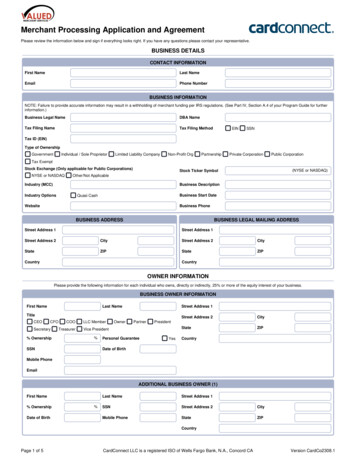
HFS Dental Program Fee Schedule for Children and Adult BeneficiariesEffective January 1, 2021All services not covered are noted as N/A and will not have prior authorization requirementProcedureCodeDescriptionMaximum Prior Approval dultsUpdated December 29, gnantWomenPrior ApprovalRequiredPregnantWomenD1526Space Maintainer – removable – bilateral, maxillary 74.70NN/AN/AD1527Space Maintainer – removable – bilateral, mandibular 74.70NN/AN/AD1551Recement Space Maintainer – Maxillary 10.70NN/AN/AD1552Recement Space Maintainer – Mandibular 10.70NN/AN/AD1553Recement Space Maintainer – per quadrant 10.70NN/AD2140Amalgam-1-Surface, Primary or Permanent 30.85N 30.85N 30.85ND2150Amalgam-2-Surfaces, Primary or Permanent 48.15N 48.15N 48.15ND2160Amalgam-3-Surfaces, Primary or Permanent 58.05N 58.05N 58.05ND2161Amalgam-4 -Surface, Primary or Permanent 58.05N 58.05N 58.05ND2330Resin-Based Composite - 1-Surface, Anterior 34.60N 34.60N 34.60ND2331Resin-Based Composite - 2-Surfaces, Anterior 51.90N 51.90N 51.90ND2332Resin-Based Composite - 3-Surfaces, Anterior 61.80N 61.80N 61.80ND2335Resin-Based Composite – 4 surfaces, or involving Incisal Edge, Anterior 61.80N 61.80N 61.80ND2391Resin-Based Composite – 1-surface, Primary or Permanent 30.85N 30.85N 30.85ND2392Resin-Based Composite – 2-surfaces, Primary or Permanent 48.15N 48.15N 48.15ND2393Resin-Based Composite – 3-surfaces, Primary or Permanent 58.05N 58.05N 58.05ND2394Resin-Based Composite – 4 surfaces, Primary or Permanent 58.05N 58.05N 58.05ND2542Onlay - Metallic - two surfaces 235.20Y 235.20Y 235.20YD2543Onlay - Metallic - three surfaces 235.20Y 235.20Y 235.20YD2544Onlay - Metallic - four or more surfaces 235.20Y 235.20Y 235.20YD2642Onlay - Porcelain/Ceramic - two surfaces 235.20Y 235.20Y 235.20YD2643Onlay - Porcelain/Ceramic - three surfaces 235.20Y 235.20Y 235.20YD2644Onlay - Porcelain/Ceramic - four or more surfaces 235.20Y 235.20Y 235.20YD2740Crown – porc/ceramic 235.20Y 235.20Y 235.20YD2750Crown – porc/metal high noble 235.20Y 235.20Y 235.20YD2751Crown - Porcelain/Base Metal 235.20Y 235.20Y 235.20YD2752Crown – porcelain/metal noble 235.20Y 235.20Y 235.20YD2753Crown - Porcelain/Titanium 235.20Y 235.20Y 235.20YD2790Crown – full metal high noble 145.85Y 145.85Y 145.85YN/A
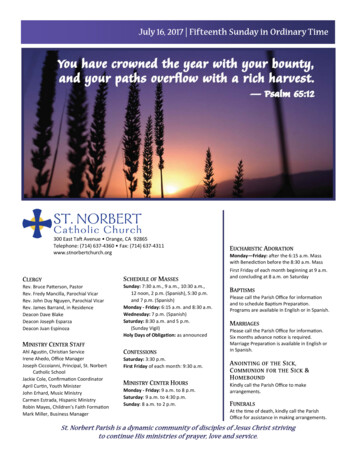
HFS Dental Program Fee Schedule for Children and Adult BeneficiariesEffective January 1, 2021All services not covered are noted as N/A and will not have prior authorization requirementProcedureCodeDescriptionMaximum Prior Approval dultsD2791Crown - Full Cast Base Metal 145.85D2792Crown – full metal nobleD2910Recement InlaysD2915D2920Updated December 29, gnantWomenPrior ApprovalRequiredPregnantWomenY 145.85YY 145.85 145.85Y 145.85Y 145.85Y 11.30N 11.30N 11.30NRecement cast or prefabricated post and core 23.50N 23.50N 23.50NRecement Crown 23.50N 23.50N 23.50ND2930Prefabricated Stainless Steel Crown (SSC) Primary Tooth 73.40NN/AD2931Prefabricated Stainless Steel Crown (SSC) Permanent Tooth 73.40Y 73.40Y 73.40YD2932Prefabricated Resin Crown 56.45Y 56.45Y 56.45YD2933Prefabricated Stainless Steel crown with resin window 56.45NN/AD2934Prefabricated esthetic coated stainless steel crown - primary 73.40NN/AD2940Protective Restorations 11.30N 11.30N 11.30D2950Core buildup, including any pins 58.05N 58.05N 58.05D2951Pin Retention-Per Tooth 9.40N 9.40N 9.40D2954Prefabricated Post and Core 32.90Y 32.90Y 32.90D3220Therapeutic Pulpotomy 52.70NN/AN/AD3222Partial pulpotomy 28.20YN/AN/AD3230Pulpal Therapy – (resorbable filling) – anterior, primary tooth (excl. final restoration) 52.70NN/AN/AD3310Anterior Root Canal (Excluding Final Restoration) 136.40N 136.40D3320Bicuspid Root Canal (Excluding Final Restoration) 155.25NN/AN/AD3330Molar Root Canal (Excluding Final Restoration) 202.30NN/AN/AD3351Apexification/Recalcification Initial Visit 28.20YN/AN/AD3352Apexification/Recalcification Interim Visit 14.10YN/AN/AD3353Apexification/Recalcification Final Visit 14.10YN/AN/AD3410Apicoectomy/Periadicular Surgery –– Per Tooth, First Root 112.90YN/AD4210Gingivectomy or Gingivoplasty –– 4 Teeth, Per Quadrant 131.70Y 131.70N 131.70ND4211Gingivectomy or Gingivoplasty –– 1 to 3 Teeth, Per Quadrant 65.85Y 65.85N 65.85ND4240Gingival Flap Procedure, w/ Root Planing – 4 Teeth, Per Quadrant 229.60Y 229.60N 229.60ND4241Gingival Flap Procedure, w/ Root Planing – 1 to 3 Teeth, Per Quadrant 114.80Y 114.80N 114.80ND4249Clinical Crown lengthening 138.80Y 138.80N 138.80NN/AN/AN/AN 136.40NNNYNN/A
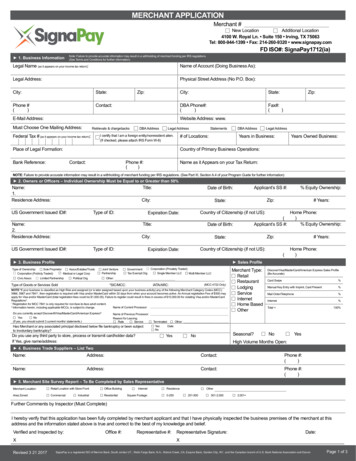
HFS Dental Program Fee Schedule for Children and Adult BeneficiariesEffective January 1, 2021All services not covered are noted as N/A and will not have prior authorization requirementProcedureCodeDescriptionMaximum Prior Approval dultsUpdated December 29, gnantWomenPrior ApprovalRequiredPregnantWomenD4260Osseous Surgery – 4 Teeth, Per Quadrant 277.60Y 277.60N 277.60ND4261Osseous Surgery – 1 to 3 Teeth, Per Quadrant 138.80Y 138.80N 138.80ND4263Bone Replacement Graft –– First Site in Quadrant 141.15Y 141.15N 141.15ND4264Bone Replacement Graft, Each Additional Site in Quadrant 70.60Y 70.60N 70.60ND4270Pedicle Soft Tissue Graft 141.15Y 141.15N 141.15ND4273Subepithelial Connective Tissue Graft Procedure 141.15Y 141.15N 141.15ND4274Distal or Proximal Wedge 70.60Y 70.60N 70.60ND4277 141.15Y 141.15N 141.15N 70.58Y 70.58N 70.58ND4320Free soft tissue graft procedure (including donor site surgery), first tooth or edentuloustooth position in graftFree soft tissue graft procedure (including donor site surgery), each additionalcontiguous tooth or edentulous tooth position in same graft siteProvisional Splinting, Intracoronal 188.20Y 188.20N 188.20ND4321Provisional Splinting, Extracoronal 56.50Y 56.50N 56.50ND4341Periodontal Scaling and Root Planing – 4 Teeth, Per Quadrant 122.00Y 122.00N 122.00ND4342Periodontal Scaling and Root Planing – 1 to 3 Teeth, Per Quadrant 77.00N 77.00N 77.00ND4355Full mouth Debridement 41.00N 41.00N 41.00ND4910Periodontal Maintenance Procedure 67.00Y 67.00Y 67.00YD5110Complete Denture - Maxillary 376.35Y 376.35Y 376.35YD5120Complete Denture - Mandibular 376.35Y 376.35Y 376.35YD5130Immediate Denture – Maxillary 376.35Y 376.35Y 376.35YD5140Immediate Denture – Mandibular 376.35Y 376.35Y 376.35YD5211Maxillary Partial Denture –– Resin Base 376.35YN/AN/AD5212Mandibular Partial Denture –– Resin Base 376.35YN/AN/AD5213Maxillary Partial Denture –– Cast Metal Framework 376.35YN/AN/AD5214Mandibular Partial Denture –– Cast Metal Framework 376.35N/AN/AD5221Immediate Maxillary Partial Denture –– Resin Base 376.35YYN/AN/AD5222Immediate Mandibular Partial Denture –– Resin Base 376.35YN/AN/AD5223Immediate Maxillary Partial Denture –– Cast Metal Framework 376.35YN/AN/AD5224Immediate Mandibular Partial Denture –– Cast Metal Framework 376.35YN/AD5511Repair Broken Complete Denture Base, Mandibular 61.15N 61.15D4278N/AN 61.15N
HFS Dental Program Fee Schedule for Children and Adult BeneficiariesEffective January 1, 2021All services not covered are noted as N/A and will not have prior authorization requirementProcedureCodeDescriptionMaximum Prior Approval dultsUpdated December 29, gnantWomenPrior ApprovalRequiredPregnantWomenD5512Repair Broken Complete Denture Base, Maxillary 61.15N 61.15N 61.15ND5520Replace Missing or Broken Teeth, Complete Denture 38.10N 38.10N 38.10ND5611Repair Resin Partial Denture Base, Mandibular 51.75Y 51.75Y 51.75YD5612Repair Resin Partial Denture Base, Maxillary 51.75Y 51.75Y 51.75YD5621Repair Cast Partial Framework, Mandibular 79.05N 79.05N 79.05ND5622Repair Cast Partial Framework, Maxillary 79.05N 79.05N 79.05ND5630Repair or Replace Broken Clasp 71.50N 71.50N 71.50ND5640Replace Broken Teeth, Each Additional Tooth 37.65N 37.65N 37.65ND5650Add Tooth to Existing Partial 42.35N 42.35N 42.35ND5730Reline Complete Maxillary Denture, Chairside 70.60Y 70.60Y 70.60YD5731Reline Complete Mandibular Denture, Chairside 70.60Y 70.60Y 70.60YD5740Reline Maxillary Partial Denture, Chairside 70.60Y 70.60Y 70.60YD5741Reline Mandibular Partial Denture, Chairside 70.60Y 70.60Y 70.60YD5750Reline Complete Maxillary Denture, Laboratory 117.60Y 117.60Y 117.60YD5751Reline Complete Mandibular Denture, Laboratory 117.60Y 117.60Y 117.60YD5760Reline Maxillary Partial Denture, Laboratory 117.60Y 117.60Y 117.60YD5761Reline Mandibular Partial Denture, Laboratory 117.60Y 117.60Y 117.60YD5911Facial Moulage-sectionalBy ReportYBy ReportYBy ReportYD5912Facial Moulage-completeBy ReportYBy ReportYBy ReportYD5913Nasal ProsthesisBy ReportYBy ReportYBy ReportYD5914Auricular ProsthesisBy ReportYBy ReportYBy ReportYD5915Orbital ProsthesisBy ReportYBy ReportYBy ReportYD5916Ocular ProsthesisBy ReportYBy ReportYBy ReportYD5919Facial ProsthesisBy ReportYBy ReportYBy ReportYD5922Nasal Septal ProsthesisBy ReportYBy ReportYBy ReportYD5923Ocular Prosthesis, interimBy ReportYBy ReportYBy ReportYD5924Cranial ProsthesisBy ReportYBy ReportYBy ReportYD5925Facial Augmentation implant ProsthesisBy ReportYBy ReportYBy ReportYD5926Nasal Prosthesis, replacementBy ReportYBy ReportYBy ReportY
HFS Dental Program Fee Schedule for Children and Adult BeneficiariesEffective January 1, 2021All services not covered are noted as N/A and will not have prior authorization requirementProcedureCodeDescriptionMaximum Prior Approval dultsUpdated December 29, gnantWomenPrior ApprovalRequiredPregnantWomenD5927Auricular Prosthesis, replacementBy ReportYBy ReportYBy ReportYD5928Orbital Prosthesis, replacementBy ReportYBy ReportYBy ReportYD5929Facial Prosthesis, replacementBy ReportYBy ReportYBy ReportYD5931Obturator Prosthesis, surgicalBy ReportYBy ReportYBy ReportYD5932Obturator Prosthesis, definitiveBy ReportYBy ReportYBy ReportYD5933Obturator Prosthesis, modificationBy ReportYBy ReportYBy ReportYD5934Mandibular Resection Prosthesis with guide flangesBy ReportYBy ReportYBy ReportYD5935Mandibular Resection Prosthesis without guide flangesBy ReportYBy ReportYBy ReportYD5936Obturator Prosthesis, interimBy ReportYBy ReportYBy ReportYD5937Trismus ApplianceBy ReportYBy ReportYBy ReportYD5951Feeding AidBy ReportYBy ReportYBy ReportYD5952Speech Aid Prosthesis, pediatricBy ReportYN/AD5953Speech Aid Prosthesis, adultBy ReportYBy ReportYBy ReportYD5954Palatal Augmentation, ProsthesisBy ReportYBy ReportYBy ReportYD5955Palatal Lift Prosthesis, definitiveBy ReportYBy ReportYBy ReportYD5958Palatal Lift Prosthesis, InterimBy ReportYBy ReportYBy ReportYD5959Palatal Lift Prosthesis, modificationBy ReportYBy ReportYBy ReportYD5960Speech Aid Prosthesis, modificationBy ReportYBy ReportYBy ReportYD5982Surgical StentBy ReportYBy ReportYBy ReportYD5983Radiation CarrierBy ReportYBy ReportYBy ReportYD5984Radiation ShieldBy ReportYBy ReportYBy ReportYD5985Radiation Cone LocatorBy ReportYBy ReportYBy ReportYD5986Fluoride Gel CarrierBy ReportYBy ReportYBy ReportYD5987Commissure SplintBy ReportYBy ReportYBy ReportYD5988Surgical SplintBy ReportYBy ReportYBy ReportYD5999Unspecified Maxillofacial ProsthesisBy ReportYBy ReportYBy ReportYD6210Pontic crown – metal high noble 178.80YN/AN/AD6211Pontic crown – metal base 178.80YN/AN/AD6212Pontic crown – metal noble 178.80YN/AN/AN/A
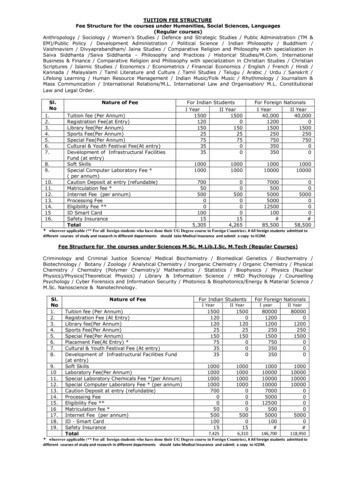
HFS Dental Program Fee Schedule for Children and Adult BeneficiariesEffective January 1, 2021All services not covered are noted as N/A and will not have prior authorization requirementProcedureCodeDescriptionMaximum Prior Approval dultsUpdated December 29, gnantWomenD6240Pontic crown – porc/metal high noble 178.80YN/AN/AD6241Pontic crown - porc/base Metal 178.80YN/AN/AD6242Pontic crown – porc metal noble 178.80YN/AN/AD6251Pontic-Resin/Base Metal 103.50YN/AN/AD6721Retainer Crown - Resin/Predominately Base Metal 136.40YN/AN/AD6750Retainer Crown – porc/metal high noble 159.95YN/AN/AD6751Retainer Crown - Porcelain/Predominately Base Metal 159.95YN/AN/AD6752Retainer Crown – porc/metal noble 159.95YN/AN/AD6753Retainer Crown – porc/metal noble 159.95YN/AN/AD6790Retainer Crown – full metal high noble 159.95YN/AN/AD6791Retainer Crown - full metal base 159.95YN/AN/AD6792Retainer Crown - full metal noble 159.95YN/AN/AD6930Recement Fixed Partial DentureD6999Unspecified, fixed prosthodontic procedure, by reportD7140D7210Prior ApprovalRequiredPregnantWomen 32.90N 32.90N 32.90By ReportYBy ReportYBy ReportNYExtraction – Erupted Tooth or Exposed Root 39.12N 39.12N 39.12NSurgical Removal of Erupted Tooth 57.40N 57.40N 57.40ND7220Removal of Impacted Tooth –– Soft Tissue 66.80Y 66.80Y 66.80YD7230Removal for Impacted Tooth –– Partially Bony 86.60Y 86.60Y 86.60YD7240Removal of Impacted Tooth –– Completely Bony 100.70Y 100.70Y 100.70YD7250Surgical Removal of Residual Roots 57.40Y 57.40Y 57.40YD7270Tooth reimplantation and/ or stabilization 88.00Y 88.00Y 88.00YD7280Surgical access of unerupted tooth 50.80YN/AN/AD7283Placement of device to facilitate eruption of impacted tooth 45.00YN/AN/AD7310Alveoloplasty in Conjunction with Extractions –– per quadrant 64.00Y 64.00Y 64.00YD7311Alveoloplasty w/ extraction – 1-3 teeth/spaces per quad 64.00Y 64.00Y 64.00YD7320Alveoloplasty Not in Conjunction With Extractions –– per quadrant 64.00Y 64.00Y 64.00YD7321Alveoloplasty w/o extractions – 1- 3 teeth/spaces per quad 64.00Y 64.00Y 64.00YD7450Removal of Odontogenic Cyst or Tumor up to 1.25cm 94.30Y 94.30Y 94.30YD7451Removal of Odontogenic Cyst or Tumor over 1.25cm 199.60Y 199.60Y 199.60Y
HFS Dental Program Fee Schedule for Children and Adult BeneficiariesEffective January 1, 2021All services not covered are noted as N/A and will not have prior authorization requirementProcedureCodeDescriptionMaximum Prior Approval dultsUpdated December 29, gnantWomenPrior ApprovalRequiredPregnantWomenD7460Removal of Non-Odontogenic Cyst or Tumor up to 1.25cm 94.30Y 94.30Y 94.30YD7461Removal of Non-Odontogenic Cyst or Tumor over 1.25cm 199.60Y 199.60Y 199.60YD7510Incision and Drainage – Abscess 36.70Y 36.70Y 36.70YD7511Incision & drainage – intraoral - complicated 36.70Y 36.70Y 36.70YD7610Maxilla Open Reduction, Teeth Immobilized 657.95Y 657.95Y 657.95YD7620Maxilla Closed Reduction, Teeth Immobilized 471.50Y 471.50Y 471.50YD7630Mandible-Open Reduction, Teeth Immobilized 824.65Y 824.65Y 824.65YD7640Mandible-Closed Reduction, Teeth ImmobilizedD7710Maxilla-Open ReductionD7720 706.95Y 706.95Y 706.95Y 1,059.35Y 1,059.35Y 1,059.35YMaxilla-Closed Reduction 706.35Y 706.35Y 706.35YD7730Mandible-Open Reduction 1,059.35Y 1,059.35Y 1,059.35YD7740Mandible-Closed Reduction 706.20Y 706.20Y 706.20YD7810Open Reduction of Dislocation 438.60Y 438.60Y 438.60YD7820Closed Reduction of Dislocation 177.65Y 177.65Y 177.65YD7961Buccal/labial frenectomy 77.15YN/AN/AD7962Lingual frenectomy 77.15YN/AN/AD7963Frenuloplasty 77.15YN/AN/AD7999Unspecified Oral Surgery ProcedureBy ReportYBy ReportD8080Initial Orthodontic Appliance Placement 900.00YN/AN/AD8660Initial Examination, Records, Radiographs & Facial Photographs 100.00YN/AN/AD8670Periodic Adjustments (11 maximum) 240.00YN/AN/AD8680Removal of Appliances, Construction, and Placement of Retainers 150.00YN/AN/AD8999Initial Orthodontic Evaluation/Study Models 47.05YN/AN/AD9110Palliative (emergency) Treatment of Dental Pain-Minor Procedures 55.00N 55.00N 55.00ND9222Deep Sedation / General Anesthesia – first 15 minute increment 38.35Y 38.35Y 38.35YD9223Deep Sedation / General Anesthesia – each 15 minute increment 38.35Y 38.35Y 38.35YD9230Inhalation of nitrous oxide/anxiolysis, analgesia 26.00N 26.00N 26.00NIntravenous Moderate (conscious) Sedation / Analgesia – First 15 minute increment 38.35Y 38.35Y 38.35YD9239YBy ReportY
HFS Dental Program Fee Schedule for Children and Adult BeneficiariesEffective January 1, 2021All services not covered are noted as N/A and will not have prior authorization s Moderate (conscious) Sedation / Analgesia – Each 15 minute incrementMaximum Prior Approval dultsUpdated December 29, gnantWomenPrior ApprovalRequiredPregnantWomen 38.35Y 38.35Y 38.35Y 48.00Y 48.00Y 48.00Y 17.10N 17.10ND9248Non-intravenous conscious sedation – Require Dental Sedation Permit A to billD9310Consultation 17.10ND9610Therapeutic Drug Injection 8.00Y 8.00Y 8.00YD9630Other Drugs and Medicaments 23.50Y 23.50Y 23.50YD9999Unspecified Procedure, By ReportBy ReportYBy ReportYBy ReportY
HFS Dental Program Fee Schedule for Children and Adult Beneficiaries Effective January 1, 2021 All services not covered are noted as N/A and will not have prior authorization requirement Updated December 29, 2020 Procedure Code Description Maximum Allowance Children Prior Approval Required Children Maximum Adults