Transcription
GME in the United States:A Review of State InitiativesSeptember 2013Julie C. Spero, MSPHErin P. Fraher, PhD, MPPThomas C. Ricketts, PhD, MPHPaul H. Rockey, MD, MPHThis work was supported by the American College of Surgeons andThe North Carolina Area Health Education Centers Program.
Corresponding authors:Julie C. Spero, MSPH juliespero@unc.edu 919.966.9985Erin P. Fraher, PhD, MPP erin fraher@unc.edu 919.966.5012Program on Health Workforce Research and PolicyCecil G. Sheps Center for Health Services Research, The University of North Carolina at Chapel Hill.725 MLK Jr. Blvd, CB# 7590 Chapel Hill, NC 27599-7590 http://www.healthworkforce.unc.edu 919.966.7112Suggested citation:Spero JC, Fraher EP, Ricketts TC, Rockey PH. GME in the United States: A Review of State Initiatives. Cecil G.Sheps Center for Health Services Research, The University of North Carolina at Chapel Hill. September 2013.Acknowledgments:This work was supported by the American College of Surgeons and the North Carolina AHEC Program.The authors wish to thank the following experts and staff for their guidance, editorial comments and related work onthis project: Eddie Alcorn, former Graduate Research Assistant, Sheps Center, UNC; Suzanne Allen, Vice Dean forRegional Affairs, University of Washington; Tom Bacon, Director, NC AHEC Program; Sarah Brotherton, Director,Data Acquisition Services, American Medical Association; Logan Corey, Medical Student, UNC School of Medicine;Katie Gaul, Research Associate, Sheps Center, UNC; Phyllis Shaw, Business Services Coordinator, Sheps Center, UNC.Finally, the authors wish to thank all of the study interview participants for their generosity in sharing their knowledgeand expertise.Part of the impetus for this project came from George F. Sheldon, MD, FACS, former chair of the department ofsurgery at UNC Chapel Hill and our colleague. Dr. Sheldon served as a mentor to all of the team and was an activeparticipant in the planning and execution of the project to the time of his passing. Graduate medical education wasone of Dr. Sheldon’s many interests and he was committed to improving the training of all physicians. He workedhard to modernize and improve GME and served as a charter member of the Council of Graduate Medical Education(COGME) when it was founded in 1985. We owe much to Dr. Sheldon and we hope his wisdom is reflected in this work.iiGME in the United States: A Review of State InitiativesProgram on Health Workforce Research and Policy at the Cecil G. Sheps Center for Health Services Research
Executive SummaryThe debate on how best to fund and reform Graduate Medical Education (GME) has moved up thehealth policy agenda. The dominant public funder of GME is Medicare with Medicaid and the VeteransAdministration contributing significantly. Proposals to change GME have focused on funding, governance,and the prioritization of specialties. Most of these proposals come from national organizations offeringnational solutions. Generally absent from the discussion is the important role states play in reformingGME. Individual states have pioneered methods and organizational structures to target GME positionstoward state health workforce needs and offered creative mechanisms to support GME.The Program on Health Workforce Research and Policy, housed within the Cecil G. Sheps Center for HealthService Research at the University of North Carolina at Chapel Hill, with support from the American Collegeof Surgeons and the North Carolina Area Health Education Centers (NC AHEC) Program, conducted a studyof state-level GME initiatives to examine the extent to which states have or plan to: 1. use health workforce datato assess residency training needs; 2. implement novel GME financing initiatives, including all payer systems;3. create governance structures to allocate GME positions between specialties, geographies and training sites;and 4. establish policies or measures to encourage accountability of public funds invested in GME. Semistructured interviews were conducted in a nationally representative sample of 17 states. A total of 39 interviewswere conducted with 45 participants in California, Florida, Georgia, Illinois, Maryland, Massachusetts,Michigan, New Jersey, New York, North Carolina, Tennessee, Texas, Utah, Vermont, and WWAMI states.*The interviews paint a picture of states having much to risk and much to gain but often missing out on importantopportunities to reform GME. Some states had rigorous data monitoring systems to identify workforce needs butdata were not linked to decisions about where, and in which specialties, to expand GME. Some states developedpolicy making bodies that attempted to coordinate GME training decisions at the state level but few of theseentities had a sustainable and coordinated role in state GME policy. Most states are investigating alternativefunding models to support GME expansion but Medicaid and all-payer payment systems are often implemented inthe same “hands off” way that Medicare dollars are treated, with individual teaching hospitals in the state drivingdecisions about how new dollars are allocated. In all states interviewed, efforts to track the accountability forspending of public GME dollars are minimal or are in a developmental stage. While state policymakers control amuch smaller GME purse than that of Medicare, there are opportunities for states to take significant action.Recommendations:1) States should develop ongoing physician workforce data collection systems that allowpolicy makers to continuously identify the changing workforce needs of the state.2) States should create a GME advisory entity that promotes discussion,coordination and education about Graduate Medical Education.3) All payer, third-party payer, Medicaid and state appropriations for GME need to be carefullyconsidered and designed to be responsive to the state’s population health needs.4) New GME funding should be tied to performance metrics and require monitoring about how funds are spent.5) State policymakers should coordinate efforts that touch on the physician’s entire career frommedical school admissions through graduate medical education and into practice.*WWAMI includes Washington, Wyoming, Alaska, Montana, and Idaho. The latter 4 states have an agreement whereby they send studentsto the University of Washington, which serves as a public medical school for all 5 states. We did not interview any experts from Alaska orWyoming for this study, but we did interview WWAMI experts who were familiar with GME policies and programs in all 5 states.GME in the United States: A Review of State InitiativesProgram on Health Workforce Research and Policy at the Cecil G. Sheps Center for Health Services Researchiii
Table of ContentsI.INTRODUCTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1II.METHODS. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2A. State SelectionB. Key Informant InterviewsIII. RESULTS. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4A. Assessing State Health Workforce Needs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41. General Surgery, Primary Care, Psychiatrist and Other Specialty Shortages2. Geographic Maldistribution3. A National versus Local Market for GME?B. Using Workforce Data to Inform GME Policy. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61. Data Collection and Analytical Challenges2. Growth in Undergraduate and Graduate Medical Education3. Use of Data by Policy Makers and State Legislators4. Exemplar Uses of Data to Shape State Medical Education PolicyC. Financing GME. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 101. Medicaid GME Financing2. HRSA’s GME Programs3. GME Training Supported by the Veterans Health Administration4. Third-Party Payers and All-Payer SystemsD. Coordinating GME Decision-Making to Match State Workforce Needs . . . . . . . . . . . . . . . . . . . . . . 181. Virgin Hospital Start-Up Funding in Georgia2. The Utah Medical Education Council3. Other Examples of State GME BoardsE. Measuring Accountability for Investment of Public Dollars in GME. . . . . . . . . . . . . . . . . . . . . . . . 22F. Looking Beyond GME: Other Strategies to Address Physician Workforce Issues . . . . . . . . . . . . . . . . 23IV.CONCLUSIONS AND RECOMMENDATIONS. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25References. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Appendix 1: State Selection Criteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Appendix 2: Structured Interview Guide. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35ivGME in the United States: A Review of State InitiativesProgram on Health Workforce Research and Policy at the Cecil G. Sheps Center for Health Services Research
GME in the United States: A Review of State InitiativesI. INTRODUCTIONMany pressing issues are facing the physicianworkforce in the United States, including a rapidconsolidation of health systems, new ways oforganizing health care delivery, experimentation withalternative payment models, malpractice reforms,and multiple initiatives to increase access, improvequality, and lower costs. In the face of so manychallenges, it is tempting to overlook the need toplan for the number, specialty mix, and geographicdistribution of the future physician workforce.There has been a rapid expansion in medical schoolenrollment (a combined 30% increase in first yearallopathic and osteopathic medical school positionsnationwide between 2002 and 2012)1,2 without aconcurrent plan to expand graduate medical education(GME) positions. Medicare is the largest singlecontributor of GME funds, in the amount of roughly 9.5 billion annually.3 Policy toward GME is verymixed; there are proposals to either cut GME funding(i.e. Deficit Reduction Commission recommendations)or increase GME funding (i.e. The Resident PhysicianShortage Reduction Act of 2013: H.R. 1180 & S. 577).Debates over how best to support GME have becomecontentious; numerous organizations including theMacy Foundation, the American College of Physicians,the American Academy of Family Practice, theAmerican Medical Association, and the Associationof American Medical Colleges have been assemblingdata and publishing evidence to support their positionson how to change GME and who should bear thecost. Numerous papers have recently been issuedcalling for increased accountability of GME dollarswith better alignment between funding of GMEpositions and the nation’s health workforce needs.3-9Often missing in these analyses and policy reports isthe recognition that states play an important role inaddressing GME. Individual states have pioneeredmethods and organizational structures to prioritize andtarget GME positions toward state health workforceneeds and offered creative mechanisms to supportGME. States have a strong stake in developing GMEprograms to meet the needs of special populationsand their constituents. To better understand whatstates are doing, the Cecil G. Sheps Center for HealthService Research at the University of North Carolinaat Chapel Hill, with support from the AmericanCollege of Surgeons and the North Carolina AreaHealth Education Centers (NC AHEC) Program,conducted a study of state-level GME initiatives.The objectives of this study were to examine the extentto which states have, or plan to:1) use health workforce data to assessresidency training needs;2) implement novel GME financing initiatives,including all payer systems;3) create governance structures to allocateGME positions between specialties,geographies and training sites; and4) establish policies or measures to encourageaccountability of public funds invested in GME.GME inin thethe UnitedUnited States:States: AA ReviewReview ofof StateState InitiativesInitiativesGMEProgramon HealthWorkforcePolicy at the Cecil G. Sheps Center for Health Services ResearchCecilG. ShepsCenterfor HealthResearchServicesandResearch1 1
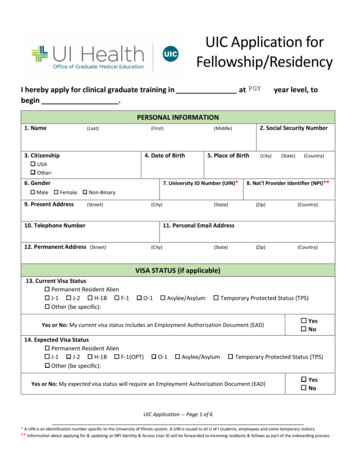
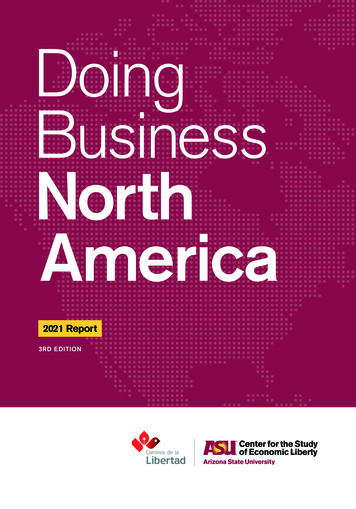
These states also represented a balance ofdemographic factors, including states with ahigh, low and average percent of urban and nonelderly uninsured populations. We also soughtto include states with a range of high, low andaverage supply of physicians and residents-intraining per population (Figures 2 and 3).iiII. METHODSWe interviewed a wide variety of GMEstakeholders in a nationally representativesample of states to capture perspectives on statebased initiatives to finance and expand GMEtraining. A total of 39 interviews were conductedwith 45 participants in 17 states using a semistructured protocol. The minimum number ofinterviewees per state was 2, the maximum was4, and the median was 2. Interviews occurredbetween March 1 and June 28, 2013.Because we sought to investigate states as policylaboratories where innovative GME initiativeswere underway, we also selected specific statesbased on information from subject matter expertsand from peer reviewed and grey literature.A. State SelectionB. Key Informant InterviewsStates selected to be in the sample representeda balance of census regions and included:California, Florida, Georgia, Illinois, Maryland,Massachusetts, Michigan, New Jersey, NewYork, North Carolina, Tennessee, Texas, Utah,Vermont, and WWAMI statesi (Figure 1).We used a purposive sampling strategy to identifykey informant interviewees in each state. Keyinformants were identified from the research team’scontacts, subject matter experts and stakeholderorganizations. The American Medical Associationsent an informational email about the study toFigure 1. States in the IStudy StateStudy State - WWAMINot in StudyAKFLiWWAMI includes Washington, Wyoming, Alaska, Montana, andIdaho. The latter 4 states have an agreement whereby they send studentsto the University of Washington, which serves as a public medicalschool for all 5 states. We did not interview any experts from Alaskaor Wyoming for this study, but we did interview WWAMI experts whowere familiar with GME policies and programs in all 5 states.2iiFor a fuller description of the sample selection criteria see Appendix 1.GME in the United States: A Review of State InitiativesProgram on Health Workforce Research and Policy at the Cecil G. Sheps Center for Health Services Research
Figure 2: Total physicians per 100,000 population, 2010450Number of Physicians per 10K Pop400MA415Study StateStudy State - WWAMINot in StudyNational ource: AAMC Center for Workforce Studies State Physician Workforce Data Book. 2011.StateFigure 3: Total residents and fellows per 100,000 population, 201080MA83Study StateStudy State - WWAMINot in StudyNational TARKYMECOKSAZORINOKGAFLMSNDSDNVWYAKIDMTNumber of Residents & Fellows per 10K Pop90Source: AAMC Center for Workforce Studies State Physician Workforce Data Book. 2011.StateGME in the United States: A Review of State InitiativesProgram on Health Workforce Research and Policy at the Cecil G. Sheps Center for Health Services Research3
state medical association contacts, requestingreferrals to individuals knowledgeable aboutGME decision making. The American College ofSurgeons also provided a list of contacts. Oncean initial group of individuals was identified, weused a snowball sampling technique to identifyadditional key informants. In some instances,interviewees recommended contacts withspecific GME knowledge or expertise beyondthat of the interviewee (for example, in GMEfinancing), and other interviewees recommendedcontacts with a different perspective on GMEin their state (for example, in different medicaleducation systems, government branches, orGME related non-governmental organizations).The majority of our interview panel was comprisedof deans, assistant deans, and associate deans inmedical schools or directors of graduate medicaleducation programs at academic medical centers orteaching institutions. Other respondents includedGME stakeholders from non-governmentalorganizations with health workforce expertise,government employees with roles in state-levelGME policy, Area Health Education Center(AHEC) directors, medical association healthpolicy specialists, and hospital residency programdirectors. Key informants with insights into surgeryGME were included as suggested by the authors andleadership of the American College of Surgeons.We conducted phone interviews using a semistructured interview guide (see Appendix 2).Interview questions concentrated on four key studydomains related to whether and/or how states: assessed the mix of health workforce, includingtypes of physician specialties, needed in theirstate to meet population health needs; considered, or pursued, various fundingmodels to support an increase in GMEpositions, including all-payer systems; created governance structures that useworkforce data to inform decisionsabout developing and allocatingGME positions between specialties,geographies and training sites; and established (successfully or not) measuresto ensure accountability of public dollarsspent on GME for meeting the healthworkforce needs of the state’s population.Interviews lasted between 45 minutes and 1 hour.Interview questions were emailed to intervieweesin advance so they could prepare responses,assemble supporting documentation and askthe appropriate individuals to join the phoneinterview. We also requested any available greyliterature on state GME policy prior to interviews.Interview notes were shared with intervieweeswithin 10 business days of the interview.Interviewees were offered the opportunity to makecorrections to the notes and to mark commentsconfidential if desired. If interviewees did notrespond to the request for corrections,iii theoriginal interview notes were used in analysis.Our interview protocol was submitted tothe University of North Carolina InternalReview Board in February 2013 andwas exempted from IRB review.III. RESULTSA. Assessing State Health Workforce NeedsInterviewees in every state noted shortages ofphysicians in specific specialties and/or geographicareas. Respondents from all states reported thatrural areas had difficulty recruiting and retainingphysicians. Many also cited concerns about otherunderserved populations, including the urbanpoor and specific racial or ethnic groups.iii4Eighteen interviewees in 14 states did not respond to the request toprovide corrections to the interview notes.GME in the United States: A Review of State InitiativesProgram on Health Workforce Research and Policy at the Cecil G. Sheps Center for Health Services Research
1. General Surgery, Primary Care,Psychiatrist and Other Specialty ShortagesRespondents from two states (California and NorthCarolina) noted that pediatric shortages were lessof a concern than adult primary care, particularlygeneral internal medicine and family medicine. Arespondent from Michigan noted that the state’schanging demographics were an important driverof health workforce needs—Michigan’s pediatricpopulation is shrinking relative to growth in theelderly population, but few providers in the statespecialize in geriatric care. Interviewees from ninestates described specific population groups wholack access to care, most frequently those of lowsocioeconomic status or minority ethnic groups.Three states noted that pediatric subspecialists werein shortage, a trend that was recently noted by theAmerican Academy of Pediatrics.10 Nationally, thepercentage of children who require subspecialistpediatric care is very small, so pediatric subspecialtyGME programs are located at large academic healthcenters with a wide referral region to generate thepatient volume required for training. As a result, fewpediatric subspecialists graduate from GME trainingeach year and their recruitment is a challenge.A hospital that loses a pediatric subspecialistfrequently has difficulty finding a replacement,necessitating the transfer of those patients to otherhospitals. An interviewee from Texas noted thatlosing just one or two pediatric subspecialists in amajor metropolitan area would create an overnightshortage. A respondent from North Carolinanoted that because there are so few pediatricsubspecialists in the country, if a large AcademicHealth Center (AHC) in the state lost one of theirphysicians, a pediatric subspecialist from one of thestate’s competing AHCs would provide coverageduring the recruitment period, and vice versa.The supply of psychiatrists was mentioned as aconcern by nearly all (14) states. A respondentfrom California noted that there was a shortageof psychiatrists in several parts of the stateand the situation was “crisis-like” for manycommunities. A respondent from Idaho notedthat all forty-four counties in the state qualifiedas Mental Health Professional Shortage Areas.2. Geographic MaldistributionAll states except Vermont noted concerns aboutthe availability of general surgeons in rural andunderserved areas. General surgeons are particularlycritical in rural areas to care for trauma and acutecare general surgery issues. Management ofthese urgent surgical problems, including manytraumatic injuries, appendicitis, incarceratedhernias, intestinal perforation, and necrotizing softtissue infections, is time-sensitive and thereforeideally managed without the delay of transferto other hospitals. In Montana, one respondentnoted that there were only 2 or 3 general surgeonsin the entire state that were not practicing in ametropolitan area. Another interviewee notedthat all five WWAMI states were in a “horriblesituation” due to the lack of rural general surgeons.Interviewee comments substantiated the findings ofprior studies on rural general surgeon shortages.9,11,12A respondent from Georgia noted that generalsurgeons were the oldest cohort of physicians inthe state, and stakeholders were concerned aboutthe future availability of general surgeons. Manyrespondents noted that most general surgeryresidents went onto specialty training and that fewof the graduates who remained in general surgerysought positions in rural areas. One respondent at anacademic health center in New Jersey reported thatin the last 3 years, only one graduate had gone onto practice in general surgery, while all others wenton to subspecialty training. A few respondents citedconcerns that the trend of subspecialization may inpart be due to the change in duty hour regulationsbecause graduates from surgical residency programshad performed fewer procedures and were lessconfident going directly into practice, preferringinstead to pursue ongoing training in fellowships.GME in the United States: A Review of State InitiativesProgram on Health Workforce Research and Policy at the Cecil G. Sheps Center for Health Services Research5
Most surgical training occurs in large, academichealth centers, rather than rural practiceenvironments that prepare trainees for the realitiesof, and broad scope of, rural general surgery.13Interviewees described difficulties recruitinggeneral surgeons to rural areas due to the lackof mentorship, limited abilities to consult withpeers, call burden and lack of cross coverage, lackof job opportunities for a spouse, and concernsabout local amenities and school systems. A fewrespondents noted that, in addition to being acritical provider of care to the community, generalsurgeons are an important economic force in ruralareas. Rural hospitals are often the largest employersin small communities and a general surgeon isan essential economic driver for the hospital.14Without a general surgeon on staff, hospitalsmust resort to hiring locum tenens surgeons,which is expensive, or they may risk closing.An interviewee shared an analysis of the ruralphysician workforce in Texas that showed thatbetween 1999 and 2009 the number of generalsurgeons in rural areas declined by 8%. Duringthe same period, the number of cardiologists inrural areas doubled and the number of orthopedicsurgeons increased by 25%. The respondent notedthat, in the absence of general surgeons, subspecialty surgeons, some without general surgerypreparation, were beginning to fill roles that wereonce taken by general surgeons in more remoteparts of the state. The respondent did not commenton whether this was an appropriate trend.All states reported a maldistribution of primarycare providers. Respondents from Maryland,Massachusetts, and New York noted that eventhough their states had some of the highestphysician-to-population ratios in the country,the maldistribution of physicians had resulted inpockets of the state, particularly in more rural areas,lacking primary care physicians. Respondents inIllinois noted that access to care was limited inthe southern, more rural portion of the state.6Nine states reported concerns about the supply anddistribution of obstetricians/gynecologists(OB/GYNs). In Tennessee, one respondentnoted that in one major metropolitan area,OB/GYNs complained that they did not haveenough work while a rural county about anhour’s drive away had no OB/GYNs.3. A National versus Local Market for GME?The market for graduate medical education isnational—programs generally recruit residents froma national pool of applicants and produce traineeswho practice all over the country. Even respondentsfrom AHCs that receive annual appropriations fromthe state legislature noted that their focus tendedto be on serving national, rather than state needs.For highly specialized fields, a national perspectiveon training is logical. Highly specialized fieldslike neurosurgery, cardiac surgery and pediatricsubspecialties require large patient volumes thatare only available at AHCs in metropolitan areasand recruitment for these specialties tends to drawfrom a national pool. However, for core specialties,particularly general adult primary care, generalsurgery, and psychiatry, the market is local. Thesepositions are needed across a wide variety of settingsand training programs and rotations can be placedin a broader geographical area within the state.Interviewees expressed frustration with nationalorganizations that advocate for GME expansionand an increase in federal funding for GME withoutadvocating that new funds be tied to local andnational population health needs. Intervieweesnoted that GME monies would be best used notjust to increase the overall supply of physiciansbut as a way to address the maldistributionof physicians by specialty and geography.B. Using Workforce Data to Inform GME PolicyOne hypothesis of this study was that manystates were expanding GME programs basedon anecdotal evidence and political/financialGME in the United States: A Review of State InitiativesProgram on Health Workforce Research and Policy at the Cecil G. Sheps Center for Health Services Research
considerations and not using workforceanalyses to identify where GME expansion wasneeded by specialty and geographic area.1. Data Collection and Analytical ChallengesMany states noted how difficult it is to determinethe “right” number of residents needed in differentspecialties. Some interviewees reported usingnational data sources to benchmark their state’sphysician-to-population ratios to the national averageand neighboring states. But states noted that nationaldata were of limited use because average ratios donot account for the maldistribution of providers.For example, a respondent from Vermont noted thataccording to the AAMC data, VT has the highestprimary care physician to population ratio in thenation, but because the state’s primary care physiciansare highly concentrated in a few areas, Vermontershave difficulty accessing primary care in rural areas.The quality of physician workforce data collectedvaried considerably state-to-state. Some states, likeNorth Carolina, Florida, and Texas, have a robustinfrastructure in place to annually collect andanalyze licensure data on the physician workforce.Physician specialty counts are available at thecounty level, providing a detailed understanding ofthe state’s workforce. Other states conduct routinesurveys of the physician workforce to gather databut survey response rates vary, from 80% to 100% inGeorgia, to 65%-75% in Utah, and 16% in Michigan.New Jersey recently passed legislation requiringphysicians to complete a workforce survey everytwo years. New York and New Jersey also conductregular GME exit surveys, which provide specificdata on the specialty, setting, and geographiclocation of practice for new GME graduates.Several states noted challenges in physician workforcedata collection. In California, legislation requires theDepartment of Health and Human Services to collecthealth workforce data, but no funding is attached tothe mandate and training institutions are
Macy Foundation, the American College of Physicians, the American Academy of Family Practice, the American Medical Association, and the Association of American Medical Colleges have been assembling data and publishing evidence to support their positions on how to change GME and who should bear the cost. Numerous papers have recently been issued