Transcription
Society of Gynecologic Oncology2020 GENETICS TOOLKITIn collaboration with:
ContentsCase 1: BRCA1 and BRCA2 mutation-related ovarian cancer4Case 2: Daughter of BRCA1 mutation carrier7Case 3: Risk-reducing salpingo-oophorectomy11Case 4: Health outcomes after risk-reducing salpingo-oophorectomy14Case 5: Impact of hereditary breast and ovarian cancer gene mutations16on male family membersCase 6: Ambiguous test results and variants17Case 7: Lynch syndrome20General Resources23Collaborating Organizations24
The purpose of this toolkit is to provide access to critical, practical informationfor health care providers, our patients, their families, and anyone interestedin gaining a deeper understanding of the role of genetics in gynecologiccancers. As this is a collaborative effort of several societies, our membersand supporters cover a wide audience that includes gynecologic oncologists,medical oncologists, genetic counselors, obstetrician gynecologists, generalpractitioners, and the lay community.The toolkit comprises specific case studies telling an individual woman’s storyto illustrate common questions and challenges faced by practitioners and theirpatients. Key points are illuminated from each organization’s perspective. Eachcase history includes references, national guidelines and society statements. A“General Resources” section includes useful tools and websites of interest.
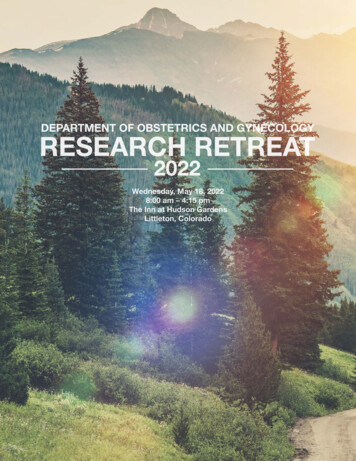
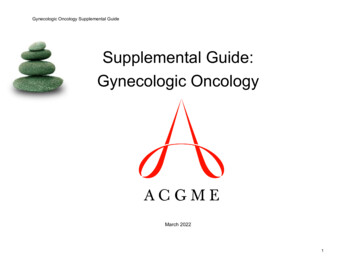
Case 1: BRCA1 and BRCA2 mutation-related ovarian cancerJanet is 58 years old and has a recent history of abdominal pain and bloating. Her primary care physician obtained a CTscan of her abdomen and pelvis. The scan showed a pelvic mass, thickening of the omentum (a fatty apron that hangsfrom the colon), and fluid accumulation (ascites). Janet was referred to a gynecologic oncologist due to the concern fora gynecologic malignancy. Her gynecologic oncologist performed surgery to remove the uterus, fallopian tubes, ovaries,and the visible tumor on other surfaces and to stage her cancer. The final pathology report diagnosed stage III highgrade serous ovarian cancer.After recovering from her surgery, Janet started the adjuvant chemotherapy that her oncologist recommended. She wassurprised that her oncologist also recommended that she undergo genetic risk evaluation and testing. She did not thinkshe was at risk for an inherited susceptibility to cancer since she has no family history of breast, colon, or ovarian cancer.She has concerns about the cost of genetic testing and the impact that it might have on her insurance status. Her30-year-old daughter, Susan, has been having a hard time accepting Janet’s cancer diagnosis. Janet worries that a resultshowing an inherited mutation might be too overwhelming for Susan.ovarian cancerother cancer50pancreaticcancer85congestiveheart failure838590dementiaFig. 1.Janet’s pedigree, or family historytree. Often inherited patterns willshow multiple family members withcancer, cancer at young ages andcancer in several generations butone-third (about 30%) of women whohave ovarian cancer and an inheritedgenetic risk do not have a strongfamily history.92845864Legend30FemaleMarriage lineTwinsMaleAffectedwith traitAdoptedLine ofdescentGenerationnumberSibling lineMiscarriageDeceasedSociety of Gynecologic Oncology 2020 Genetics Toolkit 4
Questionseffective.” Many experts would consider HBOC an exampleof an inherited syndrome where multiple genes can explainthe disease pattern seen.Why is Janet’s oncologist recommending geneticrisk evaluation and testing for her?About 20% of women with ovarian, fallopian tube, or primaryperitoneal cancer carry an inherited mutation in BRCA1,BRCA2, MSH2, MLH1, MSH6, PMS2, EPCAM, BRIP1,RAD51C, RAD51D, PALB2, and/or BARD1. Increasedhereditary risk is associated with young age at diagnosis,family history of breast and/or ovarian cancer, and someethnicities such as Ashkenazi Jewish ancestry. However,most experts feel these factors do not need to be present torecommend testing, since at least one-third of women withhereditary ovarian cancer have none of these risk factors.All histologic types of invasive (not borderline) epithelialovarian cancers should prompt consideration of referral forgenetic risk evaluation and testing. Mucinous ovarian cancerrepresents a potential exception since it has not beenshown to be part of hereditary breast and ovarian cancer(HBOC) syndrome and is rarely seen in Lynch syndrome.Genes that are part of HBOC syndrome increase the riskof breast cancer, ovarian cancer, and other cancers. Thegenes involved in Lynch syndrome increase the risk of colon,endometrial, ovarian, and other cancers.What types of genetic tests are available to Janet?Traditionally, genetic testing has been performed for 1 to2 genes at a time, starting with the gene(s) consideredmost likely to be involved based on the patient’s personaland family history. The testing looks for germline changes(mutations) in genes, meaning that the changes are inevery cell and can be passed on to children. This processcan be expensive and time-consuming if multiple genesare tested. More recently, multi-gene panel tests havebeen developed that include anywhere from a handful toseveral dozen cancer predisposition genes. These panelshave the advantage of testing for many potential genemutations simultaneously at a lower cost than traditionaltesting. Because so many genes in a panel are beinginvestigated, however, there is also a higher likelihood ofdiagnosing a variant of uncertain significance (VUS), whichis a genetic change without any clear association with ahealth problem. Changes in a gene that are known to beassociated with a health problem like cancer are calleddeleterious mutations or pathogenic variants. According tothe National Comprehensive Cancer Network (NCCN) 2019guidelines, all women with epithelial ovarian, fallopian tube,and primary peritoneal cancer should be offered geneticrisk evaluation and testing. The Society of GynecologicOncology (SGO) has endorsed that recommendation.NCCN guidelines include the statement that “when morethan one gene can explain an inherited cancer syndrome,then multi-gene testing may be more efficient and/or cost-Clinical recommendations like enhanced cancer screeningor risk-reducing surgery are reserved for those individualswho have a deleterious mutation or who have a strongfamily cancer history. Because most VUS are ultimatelyfound not to be associated with health problems, medicaldecisions should not be based on the presence of a VUS.The decision to pursue gene-by-gene testing versus paneltesting is a complex one that benefits from discussion witha genetics professional. In addition to germline testing,patients may benefit from having the tumor itself testedfor mutations. Mutations that occur in the tumor are calledsomatic mutations and cannot be passed through thefamily (unlike germline mutations). Knowledge of eithergermline or somatic mutations may help direct treatment.How might the genetic test results affect Janet’streatment? Would they affect her eligibility forclinical trials?Janet’s treatment might be affected in several ways ifgenetic testing shows a gene mutation. Survival fromovarian cancer is higher for women who have a BRCA1 orBRCA2 mutation compared with those who do not havea mutation, at least partially due to the fact that BRCA1and BRCA2 mutation-related ovarian cancer may be moresensitive to platinum chemotherapy. If her ovarian cancergoes into remission, the presence of a BRCA1 or BRCA2mutation might influence her decision to receive enhancedbreast cancer screening. She might choose to take a PARPinhibitor as part of maintenance therapy or treatment if herovarian cancer recurs. This new class of drugs called PARPinhibitors is particularly effective in women with BRCA1and BRCA2 mutations. Currently, 3 PARP inhibitor drugsare FDA-approved in the United States for use in womenwith ovarian cancer in specific clinical situations. This isan active area of research with ongoing clinical trials andfrequent updates to the indications for PARP inhibitors, soconsultation with an oncologist who is an expert in theiruse is recommended for ovarian cancer patients.Society of Gynecologic Oncology 2020 Genetics Toolkit 5
ReferencesB.M. Norquist, M.I. Harrell, M.F Brady, T. Walsh, M.K. Lee, S. Gulsuner, et al. Inherited mutations in women with ovariancarcinoma. JAMA Oncol. 2 (4) (2016). 482-490.Angelina Jolie Pitt: My Medical Choice (New York Times, May 14, 2013). Angelina Jolie Pitt: Diary of a Surgery (New YorkTimes, March 24, 2015).National Comprehensive Cancer Network https://www.nccn.org/professionals/physician gls/pdf/genetics screening.pdfJ.M. Lancaster, C.B. Powell, L. Chen, D. L. Richardson; SGO Clinical Practice Committee. Society of GynecologicOncology statement on risk assessment for inherited gynecologic cancer predispositions. Gynecol Oncol. 136 (1) (2015)3-7.Society of Gynecologic Oncology Clinical Practice Statement: Next Generation Cancer Gene Panels versus Gene byGene Testing, March 2014.How is Ovarian Cancer Staged? American Cancer Society. Accessed 4/7/16.Society of Gynecologic Oncology 2020 Genetics Toolkit 6
Case 2: Daughter of BRCA1 mutation carrierSusan is Janet’s daughter. Susan is now 34 years old and is trying to get pregnant. She has unexplained infertilityand is planning to undergo her first cycle of in vitro fertilization (IVF) with her husband next month. Janet was recentlydiagnosed with ovarian cancer at age 58 and has undergone genetic testing with a panel test including HBOC genes thatdocumented a mutation in BRCA1. Susan is tearful while discussing her mother’s cancer and is questioning whether sheshould move forward with IVF, both due to fear of her own risk of cancer and the possibility that her future children couldbe at increased risk. She and her husband are self-employed; their insurance does not cover her fertility treatments, soshe is not sure she can afford genetic testing. She also worries that she might lose her insurance if she is found to carrya gene mutation that increases her risk of cancer.QuestionsWhat is the potential psychological impact ofundergoing genetic testing?Although genetic testing can be stressful for patients in theshort term, most patients have a sense of relief in knowingtheir genetic status and can then move forward with theirlong-term health planning based on additional informationabout their personal risk level. For those patients who testnegative for a mutation that is known to run in the family,there is often significant relief of stress. For those who testpositive, there is opportunity to establish a risk-reductionplan moving forward with renewed certainty about theutility of such a plan. Taking action to modify a known riskcan feel more empowering than the sense that cancer“might be coming” at any time.While genetic testing has the potential to reduce anxiety bygiving a concrete result, it is important to note that geneticrisk evaluation does not infer that genetic testing mustbe done. Some patients are not ready to move forwardwith testing immediately; genetic counseling gives theminformation to use at any place in their process of comingto terms with their hereditary risk.What are Susan’s options for obtaininggenetic testing?Many experts prefer a model where patients receivegenetic counseling from a genetics professionalbefore choosing to proceed with genetic testing. Therelative scarcity of these genetics professional has ledto alternative models with primary care providers ortelehealth providers provide access to genetic testingwith variable amounts of genetic counseling. Yet anotheroption is direct-to-consumer (DTC) testing. Typically, theDTC entities are using models that are not validated formaking clinical decisions and may have a substantial errorrate in their interpretations. Results from DTC entitiesproviding ancestry and health-based services need tobe reviewed carefully with an experienced professionalbefore being used to make clinical decisions. The U.S.Preventive Services Task Force (USPSTF) recentlyupdated its guidelines for women who have never beendiagnosed with BRCA mutation-related cancer and thosewith BRCA-mutation related cancer who have completedtreatment and are in remission. USPSTF recommends thatspecifically BRCA1 and BRCA2 mutation testing be offeredto women with a personal and/or family history of breast,ovarian, fallopian tube, and/or primary peritoneal cancerwho have a positive result on a risk assessment tool. Theyacknowledge the availability of multi-gene panel testing butfeel their use requires further investigation. USPSTF did notreview evidence about the benefit of genetic counselingand testing in men.In this setting where Susan knows her mother carries aBRCA1 mutation, Susan could be tested for the single sitemutation carried by her mother. However, the potential forinherited cancer risk must always be assessed for bothsides of a person’s family to make sure the best test toaddress that risk is offered. If Susan’s father’s personaland family cancer history is concerning for a mutation inthe paternal lineage, broader testing may be indicated. Inaddition, if Susan only knew about her mother’s ovariancancer diagnosis without specific knowledge of genetictesting, panel testing (such as her mother had) would be areasonable option. NCCN guidelines include the statementthat “when more than one gene can explain an inheritedcancer syndrome, then multi-gene testing may be moreefficient and/or cost-effective”. Many experts wouldconsider HBOC an example of an inherited syndromewhere multiple genes can explain the disease pattern seen.Is genetic risk evaluation and testing typicallycovered by insurance? What is the typical cost ofgenetic testing?Genetic risk evaluation and testing for individuals at risk forBRCA mutations are considered preventive services underthe Affordable Care Act (ACA), and thus are a coveredbenefit for qualifying patients with ACA health plans.Private insurers typically follow similar guidelines; however,Society of Gynecologic Oncology 2020 Genetics Toolkit 7
plans can vary in their requirements and qualifications fortesting (e.g., number of affected relatives).The number of companies offering testing has increasedover the last few years, with the price of testing varying bycompany. Without insurance coverage, the cost of a fullBRCA1 and BRCA2 analysis varies from about 249 to 3,500 depending on the company conducting the testing.Many laboratories offer panel testing for multiple genesthat have been associated with breast and/or ovariancancer risk, rather than BRCA1 and BRCA2 alone, atsimilar cost to BRCA1/2 testing. While comprehensivetesting is required if a patient is the first in their family toundergo testing, a single site analysis (test that looks onlyfor the family’s known mutation) can be done for relativesof a patient who knows their specific mutation, frequentlyat a lower cost than comprehensive sequencing.If a woman carries a BRCA1 or BRCA2 mutation,what surveillance and risk-reduction strategies arerecommended for her?When a woman is found to carry a BRCA1 or BRCA2mutation, heightened surveillance and risk-reductionoptions are available for her. Risk-reduction strategiesare also available for some but not necessarily all of thegenes that might be included in a panel test. For breastcancer risk, increased surveillance is recommended,including annual magnetic resonance imaging (MRI) andmammography. Such screening can detect cancer earlybut does not prevent cancer. She would also have theopportunity to reduce her risk of breast cancer by up 97%through a risk-reducing mastectomy (surgical removalof breasts). Women with BRCA2 mutations who morecommonly develop estrogen receptor-positive breastcancer can be offered a type of chemoprevention drugcalled selective estrogen receptor modulators (SERMs),which are associated with breast cancer risk reduction ofup to 50%.For ovarian cancer risk, using oral contraceptives, having atubal ligation, or having a hysterectomy have been shown todecrease risk. However, surgical risk reduction with bilateralsalpingo-oophorectomy (removal of the fallopian tubesand both ovaries), is recommended for all high-risk womenafter the conclusion of any desired childbearing as themost effective risk-reduction option. Because Susan is stillinterested in conceiving a child, she could consider twiceyearly high-risk surveillance if she has a mutation. However,surveillance with pelvic exams, transvaginal ultrasound, andCA-125 blood test starting at the age of 30 has not beenshown to prolong survival in mutation carriers.When Susan has completed childbearing, she can considerrisk-reducing surgery. Removing tubes and ovaries willreduce the risk of ovarian, fallopian tube and peritonealcancer by more than 80% and the risk of breast cancer by50%. There is growing interest in earlier salpingectomies(removal of the fallopian tubes) with delayed oophorectomy(removal of the ovaries) in order to delay the onset ofmenopause; however, clinical trials using this strategy ofsalpingectomy and delayed oophorectomy are not yetcompleted, so the degree of risk reduction is not known.In addition, many women are candidates for hormonereplacement after BSO to minimize the side effects ofmenopause. Patients with a BRCA1 mutation shouldconsider removing tubes and ovaries after childbearingand between ages 35 and 40. For women with BRCA2mutations, the risk of ovarian cancer occurs later; they maydelay salpingo-oophorectomy until 40-45 years of age.This strategy reduces the risk of ovarian and fallopian tubecancer, but does not confer additional risk reduction forbreast cancer until the time of oophorectomy. In patientswho choose mastectomy for breast cancer risk reduction,and who have not been previously diagnosed withbreast cancer, estrogen replacement therapy is safe andreasonable. Hysterectomy (removal of the uterus) alongwith salpingo-oophorectomy is also an option based onpersonal factors discussed in Case 3.Is fertility altered by a BRCA1/2 mutation? Does IVFincrease her risk of ovarian cancer?Fertility treatment does not in itself increase the risk ofcancer, but patients who are infertile are at greater riskof ovarian cancer. In addition to having an elevated riskof ovarian cancer, infertile BRCA1 and BRCA2 mutationcarriers may have decreased ovarian reserve and struggleto conceive even with IVF. However, if fertilization issuccessful, preimplantation genetic diagnosis (PGD) canbe utilized to select embryos without the mutation andavoiding passing on the mutation to offspring if that is apriority to the parents. Some studies have suggested thatwomen with BRCA1 mutations may go through menopausea year earlier than the general population but a decrease infertility has not been proven.Many BRCA1/2 mutation carriers choose not to pursuePGD, at least partly because the mutations are associatedprimarily with risk of cancer in adulthood. One childhoodcondition that can occur in rare circumstances is Fanconianemia, which happens when a person inherits a BRCA2mutation from each parent. For this reason, carefulattention should be given to the family history of bothpartners when family planning is being considered. It issometimes appropriate to offer BRCA2 gene testing (at aminimum) to the mutation carrier’s partner in this situation.Society of Gynecologic Oncology 2020 Genetics Toolkit 8
What protections are in place against insurancediscrimination?The Genetic Information Nondiscrimination Act (GINA)is a federal law that protects against discrimination byemployers or health insurers based on genetic information.GINA does not cover disability or life insurance. Theseinsurers often request information about family healthhistory, so patients considering genetic testing couldpotentially face difficulty obtaining disability or lifeinsurance whether they have tested or not. Some plans willoffer coverage in the face of familial cancer risk but placea rider on disability or death from a cancer common to afamily. Riders are often required for a period of time aftersurgeries as well, so patients may be excluded from fullcoverage until several years after a risk-reducing surgery.Given the potential implications, some individuals chooseto obtain disability or life insurance prior to testing.ReferencesJ. Balmaña, O. Díez, I.T. Rubio, F. Cardoso; ESMO Guidelines Working Group. BRCA in breast cancer: ESMO ClinicalPractice Guidelines. Ann. Oncol. 22 (Suppl. 6) (2011) vi31-34.J.L. Berliner, A.M. Fay, S.A. Cummings, B. Burnett, T. Tillmanns. NSGC practice guideline: risk assessment and geneticcounseling for hereditary breast and ovarian cancer. J. Genet. Couns. 22 (2) (2013) 155-163.S.M. Domchek, T.M. Friebel, C.F. Singer, D.G. Evans, H.T. Lynch, C. Isaacs, et al. Association of risk-reducing surgery in BRCA1 or BRCA2 mutation carriers with cancer risk and mortality. JAMA. 304 (9) (2010) 967-975.A. Finch, K.A. Metcalfe, J. Chiang, L. Elit, J. McLaughlin, C. Springate, et al. The impact of prophylactic salpingooophorectomy on quality of life and psychological distress in women with a BRCA mutation. Psycho-Oncology 22 (1)(2013) 212-219.A. Finch, A. Valentini, E. Greenblatt, H.T. Lynch, P. Ghadirian, S. Armel, S.L. Neuhausen, C. Kim-Sing, N Tung, B.Y.Karlan, W.D. Foulkes, P. Sun, S. Narod; Hereditary Breast Cancer Study Group. Frequency of premature menopause inwomen who carry a BRCA1 or BRCA2 mutation. Fertil Steril. 99 (6) (2013) 1724-8B. Fisher, J.P. Costantino, D.L. Wickerham, R.S. Cecchini, W.M. Cronin, A. Robidoux, et al. Tamoxifen for the preventionof breast cancer: current status of the National Surgical Adjuvant Breast and Bowel Project P-1 study. J. Natl. CancerInst. 97 (22) (2005) 1652- 1662.J.M. Lancaster, C.B. Powell, N.D. Kauff, I. Cass, L.M. Chen, K.H. Lu, et al; Society of Gynecologic Oncologists EducationCommittee. Society of Gynecologic Oncologists Education Committee statement on risk assessment for inheritedgynecologic cancer predispositions. Gynecol. Oncol. 107 (2) (2007) 159-162.E.M. Mikkelsen, L. Sunde, C. Johansen, S.P. Johnsen. Psychosocial consequences of genetic counseling: a populationbased follow-up study. Breast J. 15 (1) (2009) 61-8.H.D. Nelson, M. Pappas, B. Zakher, J.P. Mitchell, L. Okinaka-Hu, R. Fu. Risk assessment, genetic counseling, andgenetic testing for BRCA-related cancer in women: a systematic review to update the U.S. Preventive Services TaskForce recommendation. Ann. Intern. Med. 160 (4) (2014) 255-266.Society of Gynecologic Oncology 2020 Genetics Toolkit 9
H.D. Nelson, L.H. Huffman, R. Fu, E.L. Harris; U.S. Preventive Services Task Force. Genetic risk assessment and BRCAmutation testing for breast and ovarian cancer susceptibility: systematic evidence review for the U.S. Preventive ServicesTask Force. Ann. Intern. Med. 143 (5) (2005) 362-379.H.D. Nelson, M.E. Smith, J.C. Griffin, R. Fu. Use of medications to reduce risk for primary breast cancer: a systematicreview for the U.S. Preventive Services Task Force. Ann. Intern. Med. 158 (8) (2013) 604-614.A.H. Pieterse, M.G. Ausems, P. Spreeuwenberg, S. van Dulmen. Longer-term influence of breast cancer geneticcounseling on cognitions and distress: smaller benefits for affected versus unaffected women. Patient Educ. Couns. 85(3) (2011) 425-431.M.E. Robson, C.D. Storm, J. Weitzel, D.S. Wollins, K. Offit; American Society of Clinical Oncology. American Society ofClinical Oncology policy statement update: genetic and genomic testing for cancer susceptibility. J. Clin. Oncol. 28 (5)(2010) 893-901.A.B. Skytte, D. Crüger, M. Gerster, A.V. Laenkholm, C. Lang, K. Brøndum-Nielsen, et al. Breast cancer after bilateral riskreducing mastectomy. Clin. Genet. 79 (5) (2011) 431-437.V.G. Vogel, J.P. Costantino, D.L. Wickerham, W.M. Cronin, R.S. Cecchini, J.N. Atkins, et al; National Surgical AdjuvantBreast and Bowel Project. Update of the National Surgical Adjuvant Breast and Bowel Project Study of Tamoxifen andRaloxifene (STAR) P-2 trial: preventing breast cancer. Cancer Prev. Res. 3 (6) (2010) 696-706.American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 103: hereditary breast and ovariancancer syndrome. Obstet. Gynecol. 113 (4) (2009) 957-966.E.T. Wang, M.D. Pisarska, C. Bresee, Y.I. Chen, J. Lester, Y. Afshar, C. Alexander, B.Y. Karlan. BRCA1 germlinemutations may be associated with reduced ovarian reserve. Fertil. Steril. 102 (6) (2014) 1723-1728. doi: 10.1016/j.fertnstert.2014.08.014. Epub 2014 Sep 23.K. Otkay, J.Y. Kim, D. Barad, S.N. Babayev. Association of BRCA1 mutations with occult primary ovarian insufficiency: apossible explanation for the link between infertility and breast/ovarian cancer risks. J. Clin. Oncol. 28 (2) (2010) 240–244.Published online 2009 Dec 7. doi: 10.1200/JCO.2009.24.2057 PMCID: PMC3040011.M. Sagi, N. Weinberg, A. Eilat, E. Aizenman, M. Werner, E. Girsh, et al. Preimplantation genetic diagnosis for BRCA1/2--anovel clinical experience. Prenat. Diagn. 29 (5) (2009) 508-513. doi: 10.1002/pd.2232.M. Drüsedau, J.C. Dreesen, I. Derks-Smeets, E. Coonen, R. van Golde, J. van Echten-Arends, et al. PGD for hereditarybreast and ovarian cancer: the route to universal tests for BRCA1 and BRCA2 mutation carriers. Eur. J. Hum. Genet. 21(12) (2013) 1361-1368. doi: 10.1038/ejhg.2013.50. Epub 2013 Mar 27.National Comprehensive Cancer Network n gls/pdf/genetics screening.pdfC.A. Shu, M.C. Pike, A.R. Jotwani, et al. Uterine cancer after risk-reducing salpingo-oophorectomy withouthysterectomy in women with BRCA mutations. JAMA Oncol 2(11) (2016) 1434-1440.U.S. Preventive Services Task d-genetic-testing1Society of Gynecologic Oncology 2020 Genetics Toolkit 10
Case 3: Risk-reducing salpingo-oophorectomySusan is now 40 years of age with a feisty 4 year-old and has decided to undergo a risk-reducingsalpingo-oophorectomy (RRSO) because she carries a BRCA1 mutation. Susan’s gynecologist performs a laparoscopicRRSO. After surgery, Susan meets with her doctor to review the pathology report, which shows some atypical cells in thefallopian tubes, called serous tubal intraepithelial carcinoma (STIC).QuestionsAre any special procedures part of a RRSO?Should hysterectomy be performed alongwith RRSO?RRSO is usually performed as a minimally invasive(laparoscopic) surgery that takes approximately 60 to 90minutes. This outpatient surgery usually requires severalsmall incisions. The abdomen is inspected thoroughly anda pelvic wash is collected for cytology to see if abnormalcells are present before the fallopian tubes and ovaries aremanipulated. The blood supply to the ovary and tube isinterrupted at 2 cm or more away from the ovary to ensurethat all the ovarian tissue is removed. As much fallopiantube as possible is carefully removed from its junctionwith the uterus. An initial inspection by the pathologist isperformed during the procedure to see if obvious canceris present. After surgery, the ovaries and tubes are cut into2-3 mm sections so that each section can be carefullyexamined by the pathologist for early cancer or pre-cancer.This special pathology procedure is critical to detectmicroscopic cancer and differs from the typical processingof tubes and ovaries for benign gynecologic surgery. Theentire fallopian tube must be examined in careful detail asmost of the pre-cancer and early cancer changes are foundin the fallopian tube rather than the ovary.What is the benefit of RRSO?RRSO prevents approximately 80% of ovarian/fallopiantube and peritoneal cancer in women who carry BRCA1and BRCA2 mutations. Current guidelines recommendRRSO for women between the ages of 35 and 40, althoughdelaying until mid-forties in women with BRCA2 mutationsmay be considered because the incidence of ovariancancer is approximately 1% for women under age 50.Breast cancer risk may also be reduced by premenopausalRRSO. One study has shown that RRSO surgery alsoreduces death from all causes in women with BRCA1 andBRCA2 mutations as well as deaths specifically from breastand ovarian cancer. One caution is that women can still getprimary peritoneal carcinoma, an ovarian-like cancer, afterRRSO; however, the risk is very low, particularly when theovaries and fallopian tubes are removed in their entiretyand carefully examined for early cancers.Generally, the uterus and cervix are not at high risk forcancer in the same way the fallopian tubes and ovaries arein patients with BRCA1 and BRCA2 mutations, althoughdata have suggested a small increased risk of serousendometrial cancer in BRCA1 mutation carriers. Sinceserous uterine cancer is difficult to detect early, somewomen choose to have a hysterectomy at the time ofRRSO in order to have maximum gynecologic cancer riskreduction. Another potential advantage of hysterectomyperformed at the time of risk-reducing surgery is tofacilitate postoperative hormonal therapy; if hysterectomywere performed, only estrogen would be needed, whichconfers lower risk of hormone therapy complicationscompared to combined therapy with estrogen andprogestin. Some women choose hysterectomy becausethey are on tamoxifen for breast cancer risk reduction,which is associated with an increased uterine cancer risk.Still others may have gynecologic reasons for desiringhysterectomy, such as fibroids or abnormal Pap smears.An argument against hysterectomy is a small increase inrecovery time and surgical complications associated withthe addition of hysterectomy to salpingo-oophorectomy.Generally, the decision to include hysterectomy with RRSOin BRCA1 and BRCA2 mutation carriers should be basedon a full discussion of risks and potential benefits in shareddecision-making between the patient and her surgeon.What is the significance of serous tubalintrae
Society of Gynecologic Oncology 2020 Genetics Toolkit 4 Janet is 58 years old and has a recent history of abdominal pain and bloating. Her primary care physician obtained a CT scan of her abdomen and pelvis. The scan showed a pelvic mass, thickening of the omentum (a fatty apron that hangs from the colon), and fluid accumulation (ascites).