Transcription
Learn more about the federal 340B programThanks to new rule changes, many healthcare organizations are examiningthe federal 340B drug program, which can help reduce costs and improvepatient care for hospitals and medical centers serving indigent patients. Thiswhite paper walks through some of the decisions that need to be made tohelp determine whether the 340B program is right for your organizationand what you need to know if you decide to implement the program.Making Sense of the340B Program:Should You Participate?Although it has been in place for nearly two decades, the 340B Drug Pricing Pro gram is assuming new importance to healthcare organizations. The combinationof the Patient Protection and Affordable Care Act (PPACA), declining reimburse ment rates and the overall economic environment is creating tighter financial times that areforcing hospitals to find new ways to reduce costs. As a result, healthcare entities that areveteran participants in the 340B program are looking for ways to expand and optimize theirparticipation, and newly eligible organizations are considering joining the 340B program.Healthcare organizations can use the 340B program to help increase their financial effi ciency and, more important, to help expand and improve patient care and outcomes,which is a key goal of the PPACA. The mission of the 340B program is to allow healthcareorganizations to capture and invest program savings into expanded care for indigent andunderserved patients. And with healthcare entities increasingly moving toward outpatientservices, the cost savings from 340B are expected to grow, since it applies specificallyto outpatient medications.Healthcare entities can manage their entry into the 340B program by breakingdown the process into four core steps:1.2.3.4.Make the decision to participatePrepare for participationAvoid 340B pitfallsBuild on 340B program successMaking Sense of the 340B Program April 2012 page 1reimbursement cutsMinimum disproportionateshare adjustmentpercentage a hospital musthave in order to qualify forthe 340B program. Thereare exceptions, however.See Exhibit A on page 2 fordetails on eligibility.
EXHIBIT A:About the 340B ProgramChanges under the PPACAThe 340B program was established in 1992 as a way to help healthcare providers manage the cost of serving vulnerable and low-income patients. In general, the 340B program requires pharmaceutical manufacturers that contractwith Medicaid to provide discounts on drugs dispensed for outpatient care.The Patient Protection and Affordable Care Act has injected new life into the340B program by expanding the list of healthcare entities eligible to participate. In fact, the PPACA has led to more changes to the 340B program in thepast 18 months than in the entire history of the program.Who can participate?Any nonprofit or government-owned hospital with an indigent patient population representing more than 11.75% disproportionate share adjustmentpercentage (DSH percentage) qualifies to participate in the 340B program.More recently, the PPACA expanded the list of eligible entities to include:– Children’s hospitals with DSH percentage of 11.75% or more– Free-standing cancer centers with DSH percentage of 11.75% or more– Critical-access hospitals (no DSH requirement)– Sole community hospitals with DSH percentage of 8% or more– Rural referral centers with DSH percentage of 8% or moreStep 1: Make the decision to participate.Before deciding to participate in the 340B program, it’s impor tant to determine if your organization meets the 340B eligibilitycriteria. The Federal Health Resources and Services Admini stration maintains a list of Frequently Asked Questions aboutthe 340B program, including details on eligibility criteria, atwww.hrsa.gov/opa/faqs/index.htm. See also “About the340B Program” above for more details on the 340B programand eligible entities. Organizations that are “almost eligible”might find it productive to examine their Medicare cost reportto secure their eligibility.Next, the organization must decide whether participation will gen erate enough financial return to justify investments in programadministration. Getting started with the 340B program requiresan investment of time and resources for setup and administration.However, even with these investments, most eligible healthcareentities benefit from participating in the 340B program.A well-managed 340B program can save a great deal of money:– Typically one-third to one-half of a hospital’s total drug spendMaking Sense of the 340B Program April 2012 page 2The PPACA included three key changesto the 340B program:1. Orphan drugs supplied by the newlyeligible facilities are not eligible fordiscounts under the 340B programbecause these drugs are not considered outpatient drugs. The exception is children’s hospitals, whichwill still be able to receive discountsfor orphan drugs.2. T he law requires new auditing,reporting and other compliancerequirements for pharmaceuticalmanufacturers and 340B coveredentities.3. The U.S. Government AccountabilityOffice must make recommendationsto Congress within 18 months forimprovements to the 340B program.is for outpatients and is therefore 340B eligible. 340B programparticipation could translate into an immediate savings of 15%to 35% on outpatient drug expense.– According to one study, 70% of 340B entities would see theirdrug costs increase by a minimum of 41% if they stopped par ticipating in the 340B program.1The 340B program creates value in three ways:Better overall drug pricing. Healthcare organizations that par ticipate in the 340B program gain access to better drug pricingand additional discounts. In addition, 340B participants benefitby pooling purchasing with other entities through the 340B PrimeVendor Program. Participating in the Prime Vendor Program allowsorganizations to use existing distributors, so that — aside fromadministrative expenses — there is no cost to participate in theprogram. Learn more.Pricing ceilings. The 340B Drug Pricing Program requires drugmanufacturers that participate in Medicaid to provide out patientdrugs at a reduced price. In some cases, drugs purchased underthe program are available at up to 50% below the Average
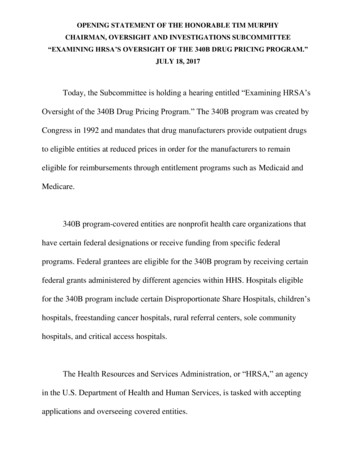
Wholesale Price or approximately 20% below group purchasingorganization (GPO) pricing.Expanded care. In addition to saving money, healthcare organi zations participating in the 340B program are able to use the pro gram to help better serve their overall patient populations, not just340B-eligible patients. For example, vaccines purchased throughthe Prime Vendor Program can be used to treat the entire eligiblepatient population. As a result, participating entities often findthat they can serve more patients and use money saved on drugsto expand other services.There are four key elements involved in setting up and managinga 340B program. Data cleanup should always be the first priority.The other three elements can occur concurrently or in an orderthat best fits the organization’s needs and situation.To obtain the full benefits of the 340B program, healthcare entitiesmust understand the program, how it works and their responsi bilities. Although setting up and administering a 340B programrequires a commitment of time and resources, it is often muchless than healthcare organizations expect. Moreover, the amountof time required and the challenges organizations face tend todecline once the program is up and running.1 There are also con sultants who can help guide an organization through setting upand administering a program.Cleaning up your data. Before enrolling in the 340B program,pharmacies must ensure their chargemaster, purchasing and bill ing data is up to date and well maintained. Clean and accuratedata makes it easier to make the business case for 340B participa tion by accurately calculating the potential financial payback andproviding support for a compliant and efficient implementation ofthe 340B program. Second, this type of cleanup helps to ensurethat all data and systems are 340B-ready. For example, pharmacychargemaster descriptions and links must be accurate and cur rent to ensure that 340B-eligible drugs have been dispensed to340B-eligible patients and that 340B drugs are ordered from thecorrect manufacturer. Clean data makes it easier for the pharmacyinformation system to clearly delineate which patients are 340Beligible and provides a strong foundation for the addition of splitbilling software to manage 340B transactions. Finally, a well-builtdata system provides the basis to support internal and externalaudits of 340B transactions.In many cases, healthcare organizations are able to enroll andadminister the program using existing internal systems supple mented by new software tools, such as split billing. This allowsthe hospital to account for drug purchases and expenditures forthe 340B program separately from non-340B activity. In fact, withthe right tools and technology and strong business management,it’s easy to set up and administer the program, and the payoff canbe considerable. (CHART 1)Data cleanup can be time-consuming, requiring a significantcommitment of staff time in some cases, but it can yield benefitsbeyond the 340B program. For one thing, a 340B-ready pharmacyis likely to support more consistent and reliable financial results inall pharmacy activities. Participating in the 340B program bringsa greater business focus to pharmacy operations because a suc cessful 340B program implementation requires greater focus andattention to detail on supply chain and data management.Step 2: Prepare for participation.Contract Pharmacy RefresherThe Prescription ProcessPharmacyprocesses anddispenses 340BprescriptionPayorClaim isadjudicatedPayor paysclaimHospitalreplenishesretail 340BstockHospital paymentPaymentallocatedProprietary Information of McKesson CorporationCHART 1Making Sense of the 340B Program April 2012 page 3These new demands can require pharmacy technicians to developnew skills and knowledge. However, those skills and attributes arelikely to become increasingly important in a post-PPACA pharmacy.In particular, pharmacy technicians should have a general businessand supply-chain background to effectively manage pharmacyoperations, regardless of whether the pharmacy participates inthe 340B program.Preparing for setup. Establishing processes and systems for 340Bprogram activities varies in complexity based on the pharmacy’s340B program goals. For example, setting up systems for a rela tively new outpatient activity separate from the core pharmacybusiness is a straightforward matter of creating accounts andtraining the staff to use new ordering tools and processes. Largedisproportionate-share hospitals and children’s hospitals also mustcomply with the GPO exclusion rule, which forbids participating
entities from purchasing any covered outpatient drugs through aGPO or other group purchasing arrangement. Setting up businessprocesses and controls to prevent errors can be complex. Likewise,critical-access hospitals and other newly eligible entities mustcomply with the orphan drug exclusion.The common denominator for any 340B setup should be phar macy staff who are well trained on the available systems andsoftware tools and are well grounded in overall pharmacy opera tions and business processes. The hospital’s business and financedepartments and the compliance officer should also participate inprogram setup and oversight decisions.Enrolling. Enrollment in the 340B program is straightforward. TheFederal Office of Pharmacy Affairs (OPA) allows eligible entities toregister for the program online at http://opanet.hrsa.gov/opa/default.aspx. Hospitals can either register outpatient facilities atDeadlines for registrationDecember 1 for the quarter beginning January 1March 1 for the quarter beginning April 1June 1 for the quarter beginning July 1September 1 for the quarter beginning October 1the same time or add them later once the initial hospital registrationis approved. Registration requirements can change at any time. Itis important to check the OPA’s website for the latest information.Newly registered entities can begin program participation on thefirst day of the next calendar quarter (see “Deadlines for regis tration” above). However, the OPA recommends registration wellbefore the deadline to allow time for OPA staff to evaluate theregistration and required documentation. This documentationincludes the most recently filed Medicare Cost Report, documen tation showing public or private ownership and operation, andcertification showing nonparticipation in a GPO (DSHs, children’shospitals and free-standing cancer hospitals only).Identifying technology needs. When it comes to managingthe data flow of the 340B program, healthcare entities havethree choices — do it manually, purchase split-billing softwareor contract with a full-service third-party vendor. The best can didates for manual data management are entities that serveonly 340B-eligible patients. Split-billing software is an appro priate choice for larger hospitals and entities that serve a mix ofMaking Sense of the 340B Program April 2012 page 4340B-eligible and non-eligible patients while also providing a mixof inpatient and outpatient care.Having a full-service 340B vendor contract often makes sense onlyfor very large hospitals and those that have retail contract pharma cies and need detailed, extensive reporting.Make organizational changes. Because 340B program par ticipation, administration and compliance require strong businesspractices, pharmacies new to the 340B program must devotemore resources, including staff time, technology upgrades andmanagement oversight to manage procurement. This allows thehospital to optimize savings under the program and meet pro gram compliance requirements and regulations. Utilizing softwarethat integrates with the hospital’s existing supply-chain solutionsmakes stronger 340B-related supply-chain management and pro curement much easier to implement.Ask for help. For the 340B program to work, it needs the sup port of key individuals in the organization. For example, the chiefmedical officer and chief nursing officer can be important advo cates for the program and take steps to make 340B program inte gration and training as easy and seamless as possible. The chiefinformation officer has an important role in buying or developingsoftware tools to help manage the 340B program and its pro cesses. The organization’s legal counsel is another key partner inthe 340B program. Because patient eligibility under the 340B pro gram is often unclear, hospitals sometimes need to consult withlegal counsel to clarify these eligibility issues.Because the potential savings opportunity is significant, efforts bypharmacy directors should include the chief financial officer (CFO)and controller to leverage their financial expertise in support of theprogram. Even if pharmacy leaders have not had a strong relation ship with the CFO, the business process and financial accountingfor 340B can be an excellent way to begin collaboration.Step 3: Avoid 340B pitfalls.Concerns about the resources and expertise required to admin ister the program, potential program-related costs, and the risksand penalties associated with noncompliance are reasons hospi tals cite for not participating in the 340B program. To avoid thesepitfalls, hospitals should invest in the program to enhance itsefficiency and effectiveness, carefully manage compliance, andmaintain the program.Focus on maintenance. Ongoing 340B program management isstraightforward, but it is often ignored. The function and efficiency
of the program can quickly deteriorate without appropriate main tenance, policies and procedures, and retention of key employeesto manage the program. Everything from formulary changes topharmacy-service modifications should be integrated into businessprocesses and into the way the pharmacy does business.It is essential to commit sufficient staff time each month to pro gram and system maintenance to capture all available 340Bsavings. This time is most often spent on maintaining separaterecords for inpatient/outpatient drugs, maintaining separaterecords for Medicaid/340B drugs, resolving vendor issues, andupdating purchase records. Seemingly small administrative tasks,such as properly tracking a switch in purchasing from one drugprovider to a different company, are critical to achieving savings ina 340B program and require constant attention.If a pharmacy has invested in the necessary data cleanup requiredfor 340B participation, however, it might have stronger data anddata-management processes that could generate enough stafftime to cover 340B requirements.Audit and review the program regularly. To realize the fullpotential savings from the 340B program, healthcare organiza tions must be prepared to make340B administration a priority.That means allocating sufficientresources to make sure the pro gram is operating at optimumeffectiveness and efficiency. Hos pitals should train staff in 340Bprogram review and audit activi ties and then undertake reviewsand audits on a regular basis.Without ongoing program review,a typical hospital tends to realizeonly about 80% of the total sav ings opportunity available underthe 340B program. Experts estimate that few participatingpharmacies expend the effort to reap those remaining savings.Examples include: regular updating of the pharmacy charge master with connections to current purchased products, reviewof purchasing procedures for specialty items to establish 340Bpurchasing when available, and establishing buyer accountabilityfor the regular review and maintenance of item accumulationsand purchase histories. Creating some sort of financial incentivefor pharmacy directors to make program review a priority can bea good way to ensure that these reviews take place.While a general audit focuses on internal controls, a 340B programaudit should also involve analyzing program data to help ensurethat the healthcare entity received the full discount to which itwas entitled, that current data is correct, and that the program isin compliance. Hospitals that make it a point to examine changesto their 340B portfolios each month and adjust administrativeprocedures accordingly can add up to 5% in additional savings,according to McKesson estimates. Those that look for the lowestcost alternative within each category and make formulary changesas a result might be able to achieve an additional 2% to 5% insavings, according to McKesson estimates.Manage compliance. When it comes to compliance, healthcareorganizations’ concerns tend to be greater than the burden of thecompliance itself. However, the 340B program’s limited programoversight means that participants must be self-policing. Coveredentities generally must take the opportunity to rectify any prob lems without direct support or intervention from HRSA/OPA.In September 2011, the U.S. Government Accountability Officeissued a report recommending greater oversight of the 340B pro gram but acknowledged that HRSA lacks the necessary fundingto do so. Even if funding is secured, it could take years to developthe systems and regulatory structure necessary to supportgreater compliance enforcement. Nevertheless, the GAOreport indicates a focus on 340B compliance. Participat ing entities should pay attention to new developments in340B compliance and enforcement.Withoutongoingreviews,a hospitaltypically seesonly 80% oftotal savings.Making Sense of the 340B Program April 2012 page 5One issue with the program is the lack of claritysurround ing some of the program’s rules and implemen tation requirements and the limited resources the federalgovernment has dedicated to 340B program support.For example, the GAO report notes that hospitals mightstruggle to determine whether they’ve been chargedthe correct price for 340B medications, since there’s noreliable database of that information. As of now, the fed eral agencies in charge of the program offer little more than anonline list of Frequently Asked Questions. As a result, healthcareentities that enroll and participate in the 340B program will needto develop their own internal expertise or turn to consultants forsupport. Even factoring in the additional costs of outside sup port, however, the financial return on 340B program participa tion is often significant.Step 4: Build on 340B program success.Once a healthcare organization gets its 340B program up andrunning, it can start looking for opportunities to enhance the
CASE STUDY:THE MEDICAL UNIVERSITY OF SOUTH CAROLINAAlthough its campus retail pharmacies and cancer centerhad been participating in the 340B program for severalyears, the Medical University of South Carolina in Charleston, S.C., had not extended its program participationbeyond the basics.However, by investing in split-billing technology to handle those requirements, the medical center managed toreduce its drug-purchasing costs by 1.4 million in thefirst year of its expanded participation with little disruption to its operations.The concern was that expanding the 340B program intomixed-use settings, such as the radiology and emergency departments, would create an administrativeheadache by requiring manual processes for identifying340B patients, tracking medications dispensed to thosepatients and reordering at 340B pricing.Disclaimer: This information is for informational purposes only. The resultsabove depend on a variety of factors that are unique to particular businesses. There is no guarantee that your results will be similar to theseresults. Each party’s results will depend on the factors of its business. Thesuccess of other businesses with this program cannot be used as an indication of future success with this program.program’s impact. Entities that limit the 340B program tooutpatient-only areas of operations might find opportunities toexpand into operations that provide both inpatient and outpatientcare, as the Medical University of South Carolina did with supportfrom split-billing software (see page 6).Perhaps the most important element of a successful 340B programis a willingness to commit to the program over the long term andto keep an open mind about how far to pursue the savings oppor tunities the program represents. As financial pressures build, thiscan be a significant opportunity that few healthcare organizationscan afford to pass up.In addition, the federal Office of Pharmacy Affairs has issued regu lations that allow partnerships under the 340B program. That hasled one large hospital to consider an opportunity to generate 5 million facilitating the delivery of 340B medications to otherhospitals in its area. Other hospitals are exploring partnershipswith retail pharmacies to maximize 340B savings.ConclusionAs many healthcare organizations have found, 340B programparticipation can yield significant savings. Yet the program is anincreasingly dynamic one. Healthcare organizations that makea commitment to the 340B program must also commit to stay ing informed about new developments, some of which have thepotential to offer significant benefits. For example, one bill pend ing in Congress could expand 340B coverage by including drugsdispensed for inpatient care.References1. Rita Lewis, Roger Schwartz and Susan Sumrell, NACHC Study: Benefits of the 340B Drug Pricing Program for Health Centers,National Association of Community Health Centers, May 2011.McKesson Health Systems800.571.2889 bop@mckesson.com mckessonbop.com 2012 McKesson Health Systems. All Rights Reserved. MHS-05977-04-12
340B eligible patients and that 340B drugs are ordered from the correct manufacturer. Clean data makes it easier for the pharmacy information system to clearly delineate which patients are 340B eligible and provides a strong foundation for the addition of split billing software to manage 340B transactions. Finally, a well built