Transcription
3/30/2017A Review of 340B Program Landscape,Risk, and Software OptimizationWilliam Pong, PharmD, MBAAdministrative Director, Pharmacy ServicesLoyola University Health SystemMarch 31st, 2017Objectives Review the 340b program landscape complexity Identify and focus on high risk areas Discuss opportunities to improve operations andprocurement savings Explain strategies to maximize regulatory compliance Describe functionalities that enhance program performanceI have no actual or potential conflict of interest inrelation to this program/presentation340B program LandscapeBackgroundLoyola University Medical Center is an 570 bed academic medical center located in Maywood,IL 20 minutes west of Chicago.On campus: Main Hospital Ambulatory clinics & surgical centers Outpatient oncology center Outpatient retail pharmacy Cover Entity (CE) – Disproportionate share hospitalChild sites – Outpatient clinics or centersContract Pharmacy – National or single VendorsIn house Pharmacy – within the hospitalOff campus: Ambulatory specialty clinics Outpatient oncology centers Home infusion pharmacyLUMC 340B Program LandscapeLandscape Key Elementsnanny EligibilityDiversionDuplicate discountRisk and Compliance1
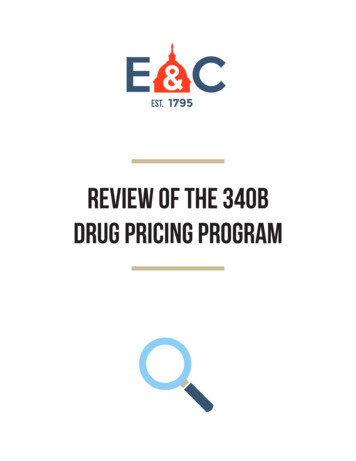
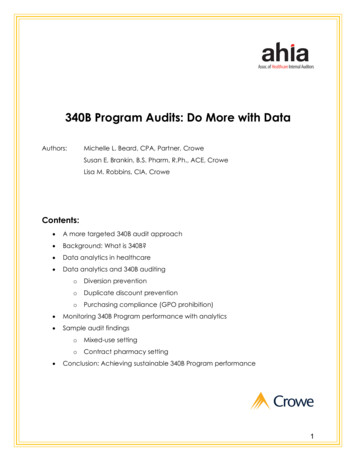
3/30/20172015 HRSA Audit Results100%90%80%70%60%50%40%30%20%10%0%2016 HRSA Audit ResultsBased on 200 Completed Audits (As of Jan 27, nLandscape – Eligibility Medicare cost report (MCR)HRSA OPA database registrationPatient definitionCover Entity – Vendor contractsAccumulation methodology (Software/Manual)Eligibility Risk Areas Cover Entity Vendor Contracts – Retail storeaccuracy in database, contract, and operations.Registration changes and eligibility identification. Accumulation methodology – Software / manual,various electronic health record data feed,Prescriber list, Wholesaler data feed, and specificfilters.1009080706050403020100Based on 148 completed audits (as of Jan 27, nEligibility Risk Areas MCR (annually) – DSH percentage, qualifyinglines, child site listings, changes (additions,deletion, relocations, etc.) HRSA OPA Database (quarterly) – Child sitesand/or contract pharmacy changes Patient definition – Prescriber, clinic, and/orcontract changesLandscape – Diversion Definition – Diversion of 340b drugs to individualswho are not patients of the covered entity. Does violation in eligibility result in diversion?2
3/30/2017Diversion Risk AreasExample ViolationsResultsDiversionProvided drugs to child site not on site not 340beligibleyesMedicare cost report (MCR) current MCRProvide drugs to Child site listed inMCR but not registered and listed site not 340beligiblein HRSA OPA databaseyesHRSA OPA database340b accumulations from a drug accumulation isdispensed / administered to anot 340bpatient prescribed by a noneligible foremployee or contracted provider. replenishmentPatient definitionyesRetail contract pharmacy listed onthe contract but not registered and Contractpharmacy is notlisted in HRSA databaseCover Entity (CE) - Vendor processed 340b prescriptions for eligible toparticipateContractthe CEyesaccumulation isInpatient drugs charges incorrectly not 340bcoded as outpatient in the EMReligible forreplenishmentyesAccumulation methodology patient encounter feedDiversion Risk - DataEligibility Key Elements NODiversion Risk - Inventory Virtual (negative 340b accumulations)Physical (Quantity dispense, on-hand inventory vs. purchases)Loan & borrow (340b to 340b sites, 340b to non 340b sites, etc.)Expired medications (replacement for outpatient areas)Crash carts (drugs used in outpatient areas)Controlled substances (used in outpatient areas)Review Question 2A CE provided 340b drugs to a new clinic that is not listed onthe current MCR and not registered with HRSA. What areas didthe CE violated?A.B.C.D.E.DiversionEligibilityIncorrect databaseA and BAll of the aboveEMR data accuracy (Charges, encounter feed, prescribers)Split billing software accuracy (Crosswalk and filters)Purchase data accuracy (Wholesalers, direct purchases)Retail pharmacy data accuracy (adjudication vs. sale, returns) Review Question 1According to HRSA OPA 2015 Audits, what was the mostprevalent violation finding?A.B.C.D.E.DiversionNo adverse findingsIncorrect databaseDuplicate discountContract pharmacy violationsLandscape -Duplicate Discount Duplicate Discount Prohibition. 42 USC 256b(a)(5)(A)(i)prohibits duplicate discounts; that is, manufacturers are notrequired to provide a discounted 340B price and a Medicaiddrug rebate for the same drug. Covered entities must havemechanisms in place to prevent duplicate discounts.3
3/30/2017Landscape -Duplicate Discount Carve in – CE bills Medicaid for outpatient drugs at340b acquisition cost. Carve out – CE does not bill Medicaid foroutpatient drugs at 340b acquisition cost.Landscape - CompliancePolicy and procedures (Established, following)Eligibility audit (340b prescriptions or orders)Database audit (child sites, cost report, contracts)Dispense vs. purchase audit (Virtual, physical)Duplicate discount audit (340b prescriptions / orders)GPO prohibition Review Question 3Which of the following areas should be included for routineaudits to ensure 340B program compliance?A.B.C.D.E.EligibilityDatabaseDuplicate discountA and CAll of the aboveDuplicate Discount – Risk Areas Medicaid rules vary from state to stateCarve in vs. carve out (CE services, contract pharmacies)UD modifier accuracy (Cover entity and child sites)Medicaid Fee for service & MCO Plan accuracy(Retail) Contract pharmacy vendor (Data transparency)Compliance - Risk Areas Auditable recordsCharge and dispense accumulations340B Drug purchasesPatient medical recordVendor contractsVendor data (dispense, accumulations, purchases)Self audit results and record keepingMaterial breach (acceptable threshold)Improve Operational Methodologies andProcurement SavingsCase # 1 background: Relates to mixed use practice areaGPO prohibition regulationCharges & accumulations captureData analyticsReport functionalities4
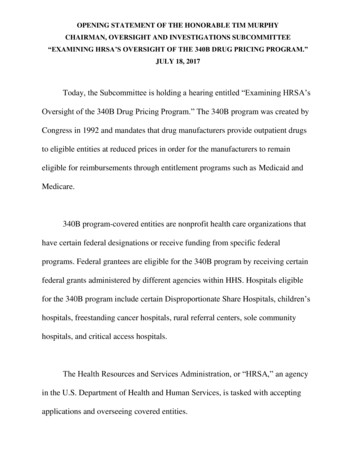
3/30/2017What Happened?The call for pharmaceutical cost savings?Top 10 drug spend .“ISUPREL” Story How it was found?The use of Wholesaler Reports:Top 10 drug spendsAssumes utilization problemRequires further investigationManipulation of 340b/WAC/GPO purchasesLimited value InvestigationBig dollar spend NDC & recent price hike impact 210 to 1,670 per vialAverage (GPO WAC) month spend of 100,000Initial goal to address appropriate usage and/oridentify alternatives Confirmed 90% of Cath/EP Lab are outpatients & missing charges Confirmed the cost difference between 340B, GPO, and WAC“WAC GPO Negative Savings” or“340B missed opportunities” Reports Example ReportNOConsolidates all purchase dataCalculates WAC / GPO to 340b savings (- / )Identifies date and time of purchasesIdentifies NDCs with WAC, GPO, 340B costIdentifies high volume & high cost purchased NDCs5
3/30/2017Savings ResultsResolution Engage Cath/EP Lab leader, establish charge captureprocess and ongoing monitoring I.T. Manager & 340B specialist monitor and confirmcharge capture in split billing software accumulation Biweekly outpatient charges to 340B accumulationsreconciliation Process hardwired and sustained after 3 monthsNO6 month savings 551,000Splitting Billing Software (SBS) ReportsConsiderations Identifying reporting needsStandard vs. custom reportsAccessibilityMeeting objectives / goalsUnique advantagesReview frequencyOptimize performance and/or complianceSBS Functionalities that enhanceprogram performance & complianceCase #2 Contract & hospital retail Pharmacies Split billing software (SBS) system filters Patient encounter feed (diagnosis code match) * Charge capture feed (depts, cdms) Prescriber list Capture rate, Lost savings, ComplianceReview Question 4Accurate drug charge capture and review of a 340Bprogram “missed opportunities” report can improveoperations and procurement savings?A. TrueB. FalsePatient Encounter Feed ICD 9 to ICD 10Software requirementsData feed acceptance / modificationsCharacter alignmentTest to productionImpacts prescription eligibility, capture volume, andsavings6
3/30/2017Data Feed OptimizationConsiderationsWhy is it important ?no Separate mixed used & retail data feed Contract pharmacy & retail data feed accuratelocations (i.e. hospital units, clinics, etc.) Automated surveillance mechanism – ensurecharge / dispense data deliver to split billingsoftware Determine optimal upload frequency (i.e. daily)ICD 10 Feed Impact on ContractPharmacy PerformancenoICD 10 Data Patient Encounter FeedElementsno Post ICD 10 Feed Fix – impact on acontract pharmacyPatient MRN#Diagnosis codeDate of ServicePatient locationPatient statusProvidersProgram Filters Are they important ?no7
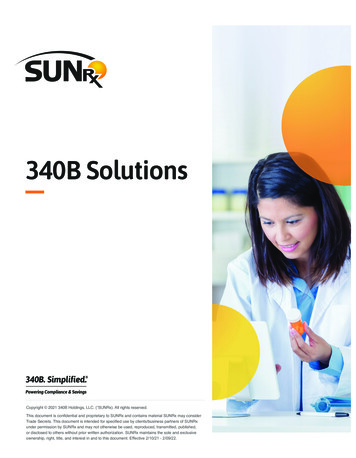
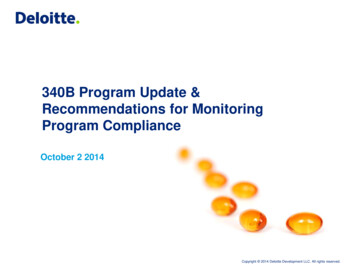
3/30/2017Split Billing Software Filtersno PrescribersDiagnosis codeMedicaidDrug class specificationsNon-covered drug rulesExample FiltersnoHow does it work noPrescriber listno ICD 10 Diagnosis Code Matchno Diagnosis code matchingConfirms visit associationDefault daysSpecific match (i.e. pain meds,antibiotics) Balance between restrictive & loose Impacts volume capture,complianceAccuracyFrequencySystem format to uploadTest NPI, DEA, or bothImpacts prescription eligibility,capture volume, savings, andcomplianceSplit Software Filters – BothTot Count820717717717Diagnosis Code match Prescriber match651651651651699729699699Prescribermatchmatch diagnosisdiagnosis 3763763763June6226226226228
3/30/2017NPI/DEA & Code Match Impact onvolume, compliance and performanceOptimization Take-awaysnonoFilters NPI & DEA match only(at risk for non‐compliance) Filters on NPI & DEA match andCode match, rules, etc.(Ensures program compliance)Review Question 6Review Question 5The effective use of prescriber DEA and diagnosiscode match in the 340b split software system canimprove program compliance and/or performance.Which of the following data elements are critical to aneffective 340B split software system?A. TrueB. FalsePrescriber list (DEA / NPI)Wholesaler purchasesPatient encounter feedProgram filtersA, C, and DA, B, C, and DContact William Pong atwpong@lumc.edufor more information.noA.B.C.D.E.F.Actionable reportsFiltersData feedsData integrityCompliance, performance, & savings9
effective 340B split software system? A. Prescriber list (DEA / NPI) B. Wholesaler purchases C. Patient encounter feed D. Program filters E. A, C, and D F. A, B, C, and D Review Question 6 The effective use of prescriber DEA and diagnosis code match in the 340b split software system can improve program compliance and/or performance. A. True B .