Transcription
Wamoyi et al. Reproductive Health 2014, ntent/11/1/88REVIEWOpen AccessA review of interventions addressing structuraldrivers of adolescents’ sexual and reproductivehealth vulnerability in sub-Saharan Africa:implications for sexual health programmingJoyce Wamoyi1*, Gerry Mshana1†, Aika Mongi2†, Nyasule Neke1†, Saidi Kapiga2,3† and John Changalucha1†AbstractBackground: Young people particularly women are at increased risk of undesirable sexual and reproductive health(SRH) outcomes. Structural factors have been reported as driving some of these risks. Although several interventionshave targeted some of the structural drivers for adolescent’s SRH risk, little has been done to consolidate such work.This would provide a platform for coordinated efforts towards adolescent’s SRH. We provide a narrative summary ofinterventions in sub-Saharan Africa (sSA) addressing the structural drivers of adolescents’ SRH risk, explore pathwaysof influence, and highlight areas for further work.Methods: 33 abstracts and summary reports were retrieved and perused for suitability. Fifteen documents met theinclusion criteria and were read in full. Papers and reports were manually reviewed and 15 interventions that metthe criteria for inclusion were summarised in a table format.Results: Most of the interventions addressed multiple structural factors, such as social norms, gender inequality,and poverty. Some interventions focused on reducing economic drivers that increased sexual risk behaviours.Others focused on changing social norms and thus sexual risk behaviours through communication. Social normsaddressed included gender inequality, gender violence, and child socialisation. The interventions includedcomponents on comprehensive sexuality and behaviour change and communication and parenting, using differentdesigns and evaluation methods. Important lessons from the narrative summary included the need for a flexibleintervention design when addressing adolescents, the need for coordinated effort among different stakeholders.Conclusion: There are encouraging efforts towards addressing structural drivers among adolescents in (sSA). Thereis, however, a need for interventions to have a clear focus, indicate the pathways of influence, and have a rigorousevaluation strategy assessing how they work to reduce vulnerability to HIV. There is also a need for coordinatedeffort among stakeholders working on adolescent vulnerability in sSA.Keywords: Structural drivers, Structural interventions, Young people, Sexual and reproductive health, AdolescentSRH programmingBackgroundSub-Saharan Africa (sSA) continues to bear the brunt ofthe Human Immuno-deficiency Virus (HIV) epidemic,with two thirds of those infected residing in the region[1]. Women and girls are the most affected accountingfor 60% of the people living with HIV from the region.* Correspondence: jwamoyi@hotmail.com†Equal contributors1National Institute for Medical Research, P.O Box 1462, Mwanza, TanzaniaFull list of author information is available at the end of the articleYoung people aged 15-24 years account for an estimated45% of new infections globally. In this age group, womenaged 15-24 years are eight times more likely to be infected than young men (ibid), pointing to the urgentneed for prevention efforts to focus on girls to abate theepidemic.Young people’s sexual behaviour is influenced by theirsocial and economic context. Aspects of this contextthat increase or decrease susceptibility of young people 2014 Wamoyi et al.; licensee BioMed Central. This is an Open Access article distributed under the terms of the CreativeCommons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, andreproduction in any medium, provided the original work is properly credited. The Creative Commons Public DomainDedication waiver ) applies to the data made available in this article,unless otherwise stated.
Wamoyi et al. Reproductive Health 2014, ntent/11/1/88to these outcomes include: gender issues in relationshipsand families, social norms and poverty [2,3]. Most familiesin rural sSA are poor [4]. Studies in Tanzania [5,6] havenoted that in order to satisfy their material needs, youngwomen from poor families may engage in transactionalsexual activity with multiple partners or casual partners oragree to have sex without a condom. Desmond et al., [7]found that in an endeavour to maximise financial gainsfrom sex, women engaged in high risk sexual practicessuch as anal sex.Several approaches have been employed to address thesituation of HIV in young people. These comprise individual (biomedical and behavioural) approaches as wellas those that go beyond the individual. Published literature on sexual health interventions have emphasised the importance of changing young people’s riskprofiles (especially their knowledge level and attitudes),but have consistently failed to produce long-term behaviour change or improved sexual health outcomes at thepopulation level [8-11]. For example, their emphasis hasbeen on assessing individual level risk factors such ascontraception and condom use knowledge. As much asunwanted pregnancy and STIs pose serious problems toyoung people, an exclusive reliance on “risk factor” explanation enhances the likelihood that our understandingof these problems is denuded of social meaning [12] andthat interventions to address such issues remain focusedexclusively on reducing adolescent risk behaviour ratherthan understanding the social environment facilitatingrisk.There have been several suggestions concerning HIVprevention efforts moving beyond individualistic approaches towards new approaches that engage withunderlying socio-structural drivers of patterns of practicesthat influence vulnerability to HIV infection [13-16].Structural drivers of HIV/AIDS have been conceptualisedas ‘physical, social, cultural organizational, community,economic, legal or policy aspects of the environment thatinfluence the risk and vulnerability environment and thusacting as barriers to, or facilitators of, HIV prevention andtreatment behaviour’ [14,17]. Causal pathways link structural factors (social, economic, political, and environmental factors) and risk of HIV. Efforts to address theseunderlying factors are commonly referred to as structuralapproaches and seek to change the root causes or structures that affect individual risk and vulnerability to HIV[16]. Hence, structural approaches to HIV preventionrecognise the limitation of the biomedical/behaviouralparadigm, and take a broader approach to the nature oftransmission, arguing that “HIV prevention behaviour isaffected by the environment as well as by the characteristics of individuals at risk” [18].There is limited published work summarising interventions addressing structural drivers for young people’sPage 2 of 15SRH risk from sSA. We aimed to fill this gap by conducting a review and summary of such interventionsamong young people aged 14-24 from sSA. We furtherexplore pathways of influence, reflecting on interventionstrengths and weaknesses and lessons learnt highlightingareas for further work. This review provides informationthat may be helpful in the identification of gaps forfuture young people’s SRH programming.MethodsPublished studies were found by searching the following electronic databases: web of knowledge, PubMed,International Bibliography of Social Sciences, and Googlescholar. A combination of search terms were used, including: sSA; adolescent and/or young people interventions,adolescent and/or structural interventions, transactionalsex; sexual behaviour; HIV risk, HIV/AIDS, HIV prevention; adolescents; young women; adolescent health; adolescent and/or reproductive health; cash transfers; adolescentand young people livelihoods; adolescent and/or youngpeople poverty; norms; and parental socialisation.Unpublished studies and non-indexed reports weresought through searches using Google Scholar, targetedsearches of websites of relevant organisations. Key scholarsand interventionists at LSHTM, UNDP, UNICEF, andseveral non-governmental organisations (NGOs) werealso approached and asked to recommend interventions.Examples of the NGOs contacted were: populations council, International Centre for Research on Women, Globalgiving and TIOS. We only searched for English languagepapers.All searches were for articles dating from 2000 to 2013.The scope of the review was limited to interventions conducted in sSA that attempted to tackle gender norms orinequities and livelihoods or poverty and were aimed atvulnerable young people (aged 14-24 years). The interventions included had either HIV or HIV risk outcomes (suchas condom use, multiple partners, intimate partner sexualviolence, intergenerational sex and STIs) and broader behaviour change and interaction skills. Interventions wereonly included if they reported atleast one outcome. Due tothe small number of interventions identified, interventionswere included whether or not they reported outcomes inpeer reviewed journals and some that were not exclusivelyfocused at young people but also age groups beyond 24years.Titles and abstracts of studies identified through electronic searches were reviewed to determine whetherthey met the inclusion criteria. Most of the articles wereexcluded based on the title alone. Thirty three abstractsand summary reports were retrieved and Thirty threeabstracts and summary reports that met the inclusioncriteria were retrieved and screened by two researchers inorder to select potentially relevant articles and reports.
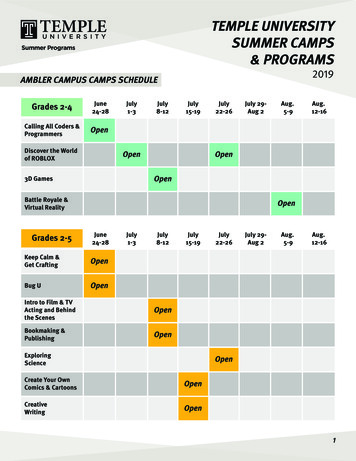
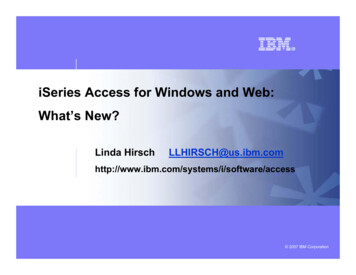
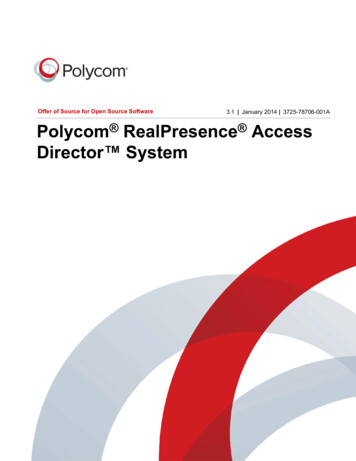
Wamoyi et al. Reproductive Health 2014, ntent/11/1/88When summaries were judged to have met inclusion criteria, full length texts were then reviewed. Where the tworesearchers disagreed on relevance of the retrieved articlea consensus was reached by consulting other co-authorswho are very experienced in the subject area. Fifteen publications were retained after meeting the inclusion criteria,five of which were derived from our search of greyliterature.For all the 15 studies, data were manually compileddescribing the following features: aim of the intervention, intervention design, target group and sample size,duration of the intervention, outcomes including thoserelated to HIV. Owing to significant differences in thepopulations studied, settings, outcomes, data analyses andreporting of included interventions, no attempts weremade to combine the data in a meta- analysis.Due to a limited number of interventions addressingour objective, studies were selected to reflect differentdesigns and hence the nature of studies reviewed were notreviewed to address general guidelines of research qualityand risk of bias as described according to Jaeshcke [19]criteria guidelines. Publication bias was therefore notassessed in the current review.The interventions were reviewed and grouped accordingto the following themes: economic empowerment ofwomen, economic empowerment plus school attendance,gender empowerment and safe spaces, comprehensivesexuality and behaviour change communication, and parental socialisation. These categories were subsequentlyused to structure the presentation of the results. It isworth highlighting that several interventions presentedfindings that fitted into more than one category.ResultsA total of 33 interventions were reviewed. Fifteen interventions met the selection criteria and are included in thesummary here. Eight of the interventions were evaluatedquantitatively while five used a combination of qualitativeand quantitative approaches. Two interventions were evaluated mainly by qualitative approaches. The interventionswere conducted in both rural and urban settings andparticipants were recruited both from schools andwithin communities. The age range of the interventionparticipants was 10-44 years, with two interventionshaving participants who were older than 24 years. Overhalf of the interventions (8/15) have an explicit focus ongirls. Nine of the interventions had their results published in peer review journals. The rest were publishedin reports.An overview of the interventions included in this reviewdescribing their primary and secondary aims is presentedin Table 1.With regards to measuring effects of the intervention,different statistical tests were used for various studies.Page 3 of 15Some authors provide a computation of the effect sizefor the differences between groups and some provideOdds Ratios, confidence intervals and p-values. On theother hand, some studies provided descriptive statisticswhich offered a perspective on the type and size ofdifference [29,30], while others reported positive improvements in their outcomes of interest e.g. increased autonomy, increased parent-child communication but nostatistics were provided.Most of the interventions seemed to have more thanone focus. Seven of the interventions had some focus onHIV prevention through changing gender norms, improving school attendance, improving economic situation ofparticipants’ and creating safe spaces. Eight of the interventions focused on either economic empowerment aloneor economic empowerment and school attendance. Threefocused on livelihoods and safe spaces, three on comprehensive sexuality and behaviour change and communication, while two took a parenting perspective.Interventions with a focus on economic drivers of SRH risksEconomic empowerment of womenSix of the interventions addressed economic empowermentof women. These were: Shaping the Health of Adolescentsin Zimbabwe (SHAZ!) [20], Intervention with Microfinancefor AIDS and Gender Equity (IMAGE) [42], The Tap andReposition Youth (TRY) (Kenya) [24,25], incentivising safersex [26], and the combined stepping stones and creatingfutures intervention [28] and Survival skills training fororphans (SSTOP) [27].SHAZ! and TRY targeted women aged 16-24 yearswhile IMAGE looked at the age group 14-44. The mostcommon characteristic for the girls in the interventionswas that they were economically inactive due to orphanhood, living in low income environments.SHAZ!, IMAGE, and the incentivising safer sex interventions were evaluated using a randomised controlled trial design. TRY used evaluations that were purely qualitative.The intervention on incentivising safer sex used conditional cash transfers as a HIV/STI prevention strategyamong both men and women aged 18-30 years, whileSSTOP focused at improving income generation skillsamong 14-19 year old young women.Overall, the interventions report positive impact. Anotable positive result across the interventions was theincreased knowledge in reproductive health and improvedfinancial management skills. The combined creating futures and stepping stones intervention targeted youngwomen and men of average age 21 years [28]. The intervention aimed to strengthen young people’s livelihoodsand economic power through reflection and action and toreduce women’s experience and men’s perpetration ofphysical or sexual IPV. The programme was evaluatedusing quantitative and qualitative methods.
Intervention/countryAimIntervention method/design &durationTarget group &Sample sizeOutcomes/resultsIncreased knowledge, Increasedeconomic empowerment,Reduced inter-generational TSPilot study- 50 poor orphaned, out-of-school,girls aged 16-19 years- Increase in HIV-related knowledgeand relationshipEconomic empowerment of women1) Shaping the Health of Adolescentsin Zimbabwe (SHAZ!) Program [20]- Uncontrolled study for 6 months- Power, no significant change incurrent sexual activity or condomuse at last sex- Microcredit loans- Living on the- Increased relationship power [21]- Business skills trainingoutskirts of Harare, Zimbabwe- Increased HIV risk through newmobility and economic strategies- Mentorship- 315 aadolescent girls, orphans,average age 18Randomized clinical trial (RCT)- Increase in HIV-related knowledgeand relationship power, no significantchange in current sexual activity orcondom use at last sexStudy- Decrease in food insecurityDuration 24 months, Adaptationof Stepping Stones, includingexpanded training includingnegotiation skills, Integrated socialsupport- Increase in equitable gender normsPhase II study:Wamoyi et al. Reproductive Health 2014, ntent/11/1/88Table 1 Descriptions for iterventions for young people- Physical and sexual violence reduce by58% over a 2-year periodAccess to HIV and reproductivehealth services2) Intervention with Microfinance for Reduced HIV risk behaviourAIDS & Gender Equity (IMAGE) [22,23],South AfricaCluster randomised trial, durationof 3 year- 55% increase in experience of IPV- A sample of 430 poor womenaged 14-35 years identified through after 1 yearparticipatory wealth ranking- Increase in HIV knowledge,communication, testing & riskreduction- 32% reduction in communicationwith household members to youngpeople in households- Greater involvement in collectiveaction and social groups- No impact on HIV incidence in widercommunity- No difference in unprotected sexat last occurrence with non-spousalpartner in past 12 monthsAt last sexPage 4 of 15- 11% increase in condom use- Microfinance (individual borrowingand repayment of loans over 10 or20 week cycles)
- Participatory learning and actioncurriculum integrated into loanmeetings (10 training sessionsdone within centre meetingsevery 2 weeks (approx. 6 months))Community mobilization for 6 to9 months following initial training- HIV prevention education3) The Tap & Reposition Youth (TRY)[24,25], KenyaIncreased reproductive health& HIV knowledge Increasedsexual negotiation skillsIncreased Income & savingsPre-test, post-test design, with- A total of Out-of-school femalesmatched comparison (222 pairs),aged 16-22 yearslength of participation ranged from 1 year (n 71), 1 to 2 years (n 81)and 2 to 3 years (n 70)- Increase Savings- Group-based microfinance loans,Livelihoods skills training- RH & HIV prevention training- Increase in liberal attitudes towardsgender roles- Living in low income & slum areasof Nairobi- 1.7 times more likely to refuse sexthan girls in control groupWamoyi et al. Reproductive Health 2014, ntent/11/1/88Table 1 Descriptions for iterventions for young people (Continued)- 3 times more likely to insist oncondom use than girls in controlgroup4) Incentivising safe sex: a randomisedtrial of conditional cash transfers forHIV and sexually transmitted infectionprevention in rural Tanzania [26]To evaluate the use of conditionalcash transfers as a HIV andsexually transmitted infectionprevention strategy toincentivise safe sexAn unblended, individuallyrandomised controlled trial- A sample of 2399 persons aged18-30 years- Intervention arms: low valueconditional cash transfer v.s., highvalue conditional cash transfer- High value CCT arm v.s., low valueCCT arm: RR 0.76 (95% CI0.49 -0.92)- Significant reduction in the combinedpoint prevalence of four curable STIsamong high value CCT arm- Tested participants every 4months over a 12 months periodfor the presence of common STIs5) Survival skills training for orphans(SSTOP) [27], MozambiqueTo reduce transactional sexIntervention:Income generating skills- High value CCT arm v.s. controls:adjusted RR 0.073 (95% CI 0.47-0.99)- Females aged 14-19 yearsQualitative & anecdotal evidencefound:- Responsible for- Increased financial organizationcaring for younger siblings, & otherdisadvantaged girls- Increase vocational skills- Reductionin early marriage- Increased economic empowerment- Girls aged 9-13 learned to makesoap, candles, sewing, or knittingPage 5 of 15- Girls aged 14-19 attended sewingclasses; HIV prevention education;& gender training including legalprotection for women- Reduction in early sexual activitywithout protection
6) Creating futures[28] (Durban,South Africa)Objective 1:To strengthen young people’slivelihoods and economic powerthrough reflection and actionObjective 2: Aimed to reducewomen’s experience and men’sperpetration of physical orsexual IPVPilot intervention combiningStepping Stones and CreatingFutures- Piloted in urban informalsettlements in with 232 youngpeople (110 men, 122 women)- The study design was aninterrupted time-series design,with baseline measures at zeroand two weeks and follow-ups atsix and 12 months post-baseline.- Average age of 21.7 years- Consisted of livelihoods andeconomic power interventioninvolving 21 sessions of threehours, delivered by trained peerfacilitatorsObjective 1:- Livelihoods improved for womenand men after the intervention- Mean earnings in the past monthincreased over the 12 months. Forwomen this increased from US 14at baseline to US 49 (a 345% increase(p 0.0001)) at 12 months and formen from US 36 at baseline toUS 104 (a 283% increase (p 0.0001))at 12 monthsFor objective 2:Women reported a statisticallysignificant reduction in theirexperience of sexual or physical IPVin the past three months from 29.9%at baseline to 18.9% at 12 months(a 37% reduction (p 0.046)- Women’s experience of sexual IPValso declined significantly from 11.1%at baseline to 3.6% at 12 months(p 0.018)Wamoyi et al. Reproductive Health 2014, ntent/11/1/88Table 1 Descriptions for iterventions for young people (Continued)- Men’s perpetration of physical orsexual IPV in the past 3 months,while declining from 25% to 21.9%(a 23% reduction) was not statisticallySignificantEconomic empowerment plus school attendance7) Zomba cash transfer [29], MalawiIncreased income IncreasedEducationReduce HIV riskRandomised control trial, 2 yearsCash transfers (CTs) conditionaland on regular school attendancev.s. unconditional CTs (averageamount US 10)A sample of 1289 never marriedgirls aged 13-22 years in 176enumeration areas in ZombaOne-year follow-up:- Reduced onset of sexual activityby 31.1%At 18 months follow-up:- Intervention group had 64%reduction in HIV prevalence and76% reduction in HSV-2 prevalence- Reduced age of partners in thosein interventionTeacher training:Page 6 of 15- No significant differences betweenconditional and unconditionalintervention group, although thestudy was not powered to show this
8) Western Kenya schoolingintervention [30]To reduce HIV incidence inschoolsRandomised control trial, 4 years,Comparing 4 school-basedHIV/AIDS interventions:A sample of 70,000 school boysand girls in school- No impact childbearing- Increase in HIV knowledge Ifpregnant, more likely to be married- Training teachers in HIV/AIDScurriculumCritical thinking:- Critical thinking on role ofcondoms- No impact on sexual activitySchooluniforms:- Reducing the cost of educationby providing school uniforms- Reduction in dropout rates 17% inboys, 14% in girls- Increase knowledge & condom use- Reduction in teen marriage 9% ingirls- Relative risk campaign- Reduced childbearing 12%Relativerisks:- Reduction in childbearing 28%- Increased sexual activity in boys- No impact on pregnant teencouplesWamoyi et al. Reproductive Health 2014, ntent/11/1/88Table 1 Descriptions for iterventions for young people (Continued)- Reduction in cross-generationalpregnancies 61%Gender empowerment and safe spaces for young people9) Binti Pamoja Centre (DaughtersUnited centre) [31,32], KenyaCreate safe spaces for girls toreduce: violence, Female genitalmutilation, Sexual abuse, Rape,Prostitution Poverty and Increase:Reproductive health knowledge,Financial education, Leadership &personal skillsCommunity intervention:- Sampled adolescents from 4ethically distinct villages in KiberaGirls aged 11-18 living in theKibera slum- Mapped all safe spaces in thecommunity2002 to present- Baseline data highlights socialisolation for many girls & 55% ofgirls live with neither or only oneparent- 30 safe spaces establishedreaching 1000 girls- Used photography, drama,writing & group discussion- Positive changes in social networks,mobility & gender norms- Peer education & empowermentworkshops- Increased financial literacy, bankingservices usage, savings, &communication with parents/guardian on financial issues- Developing skills in budgeting,savings, setting financial goals- Increased confidence & positiveself-esteem- Provided educational scholarshipsQuasi-experimental, control arm,18 month follow-up, 4 years Threestudy arms:Boys & girls aged 14-16 in schools- Increased autonomy for girls inhow they spend their money &control their lives- Increased HIV related knowledgePage 7 of 1510) Siyakha Nentsha [33], South Africa A life-orientation program toimprove lifelong skills & wellbeing of young people
- SRH/HIV, social support, financialeducation- Young men had reduced onsetof sexual activity and fewer partners- SRH/HIV & social support- Delayed Intervention (i.e. controlgroup)11) ICRW Vitu Newala [34], TanzaniaUnderstand specific vulnerabilitiesof adolescent girls and empowerthem, increase girls positiveattitudes and beliefs on girls’social protectionPilot project Qualitative assessmentsthroughout:Adolescent girls- Repeating the same participatorylearning activities,- Video parlours, discos & traditionalinitiation ceremonies identified asplaces where girls felt unsafe- Community put in place laws &changed practices to provide socialprotection- Series of IDIs with young people,- An evaluation workshopComprehensive sexuality and behaviour change communication12) Soul City Institute for health &development [35], South AfricaIncrease: social change, Socialmobilization, Advocacy andreduce HIV incidencePromoting health & social changevia TV, radio, & print Soul Buddyz:Soul buddyz:Soul City & Soul Buddys exposure- Spin off of Soul City TV seriesusing edutainment- Children aged 8-14 years, theirteachers & their caregivers- Increased: Self-perceptions on risk,Resistance to peer pressureOne love:- One love: Adults- Statically significant shifts in socialnorms, especially sexual normsWamoyi et al. Reproductive Health 2014, ntent/11/1/88Table 1 Descriptions for iterventions for young people (Continued)- Reduced Perception of- Challenged social norms onmultiple & concurrent partnership13) Stepping Stones [36,37], South Africa Increase: Sexual healthknowledge, Communicationskills, Ccritical reflection andreduce Sexual health riskCluster randomised controlled trial,2 years- 70 villages randomized to either13 3-hour sessions and 3 peergroup meetings, or a 3-hoursession on safer sex and HIV.women’s dependence on men(68% vs. 61%, p 0.05)A sample of 1077 HIV negativePersons aged 15-26 years, mostlyattending school- HIV IRR 0.85 (95%CI: 0.60, 1.20;p 0.35)- HSV2 IRR 0.69 (95%CI: 0.47, 1.03;p 0.07)- Men’s disclosure of perpetratingsevere Intimate partner violencereduced at 12 & 24 months (p 0.11& p 0.05)- Reduced Problem drinking amongmenParenting and socialisation14) Families Matter! (FMP), [38,39], Kenya Reduce age at first sex andincrease ppositive parentingpracticesCommunity-based interventionusing parent-child dyads, 2 years(2004-2006)- Increased Parenting skills &communication about sexuality &risk reduction- Parents’ attitudes regarding sexualityeducation changed positively.Five of the six composite parentingscores reported by parents, and sixPage 8 of 15Five consecutive 3-hour sessionson sexual risks and effectiveparent-child communication375 Parents/carers of 10-12 year-olds
of six reported by children, increasedsignificantly at 1 year post-intervention.15) Mema kwa Jamii (Good Things for Reduce SRH risks in youthCommunities, MkJ), [40,41], Tanzaniathrough improved parentingCommunity-based pilot parentingintervention, 2007-2010Opinion leaders in four communitiestrained to training peer parents onparenting following diffusion ofinnovation theory over a period of1 yearApproximately 1355 parents ofyoung people aged 10-18 yearsQualitative indications of impact on:- Parents socialised their male childrendifferently from female- Improved parent-child relationshipsand collective efficacyWamoyi et al. Reproductive Health 2014, ntent/11/1/88Table 1 Descriptions for iterventions for young people (Continued)Page 9 of 15
Wamoyi et al. Reproductive Health 2014, ntent/11/1/88For the two (e.g. IMAGE and SHAZ!) interventionsthat focused on HIV as one of the outcomes, both pointto little impact on HIV incidence. Interestingly, one ofthe intervention’s activities (SHAZ!) had unforeseen consequences in that it increased young women’s risk toHIV. It was noted that as young people struggled to repay the loan, they adopted risky strategies.IMAGE, incentivising safer sex intervention, combinedstepping stones and creating futures projects presentedstatistical results at the time of this review. At 1-yearfollow-up, the communities receiving the IMAGE intervention saw a 55% reduction in IPV as compared to thecontrol communities. The IMAGE intervention alsoincreased HIV knowledge, communication, testing, andrisk reduction among young women who participated inthe intervention as compared to those in the controlcommunities [22]. Although IMAGE also sought toreduce HIV incidence in the wider community wherethe interventions occurred, there was no difference inHIV incidence between the observed communities at thetime of analysis.At the end of 12 months, the results from incentivisingsafer sex intervention, showed significant reduction inthe combined point prevalence of the four curable STIstested every 4 months in the incentivized group that waseligible for the 20 payments and no such reduction wasfound for the group receiving the 10 payments [26]. DeWalque et al., [26] conclude that their results suggestthat conditional
Background: Young people particularly women are at increased risk of undesirable sexual and reproductive health (SRH) outcomes. Structural factors have been reported as driving some of these risks. Although several interventions have targeted some of the structural drivers for adolescent's SRH risk, little has been done to consolidate such work.